Page 25 of 32
PA24.9 | Liver Disease & Tumour Morphology — Practical — SDL Guide (Part 3)
The 4-Panel Comparison: Reading Composite Specimens
Four-Panel Liver Histology Comparison
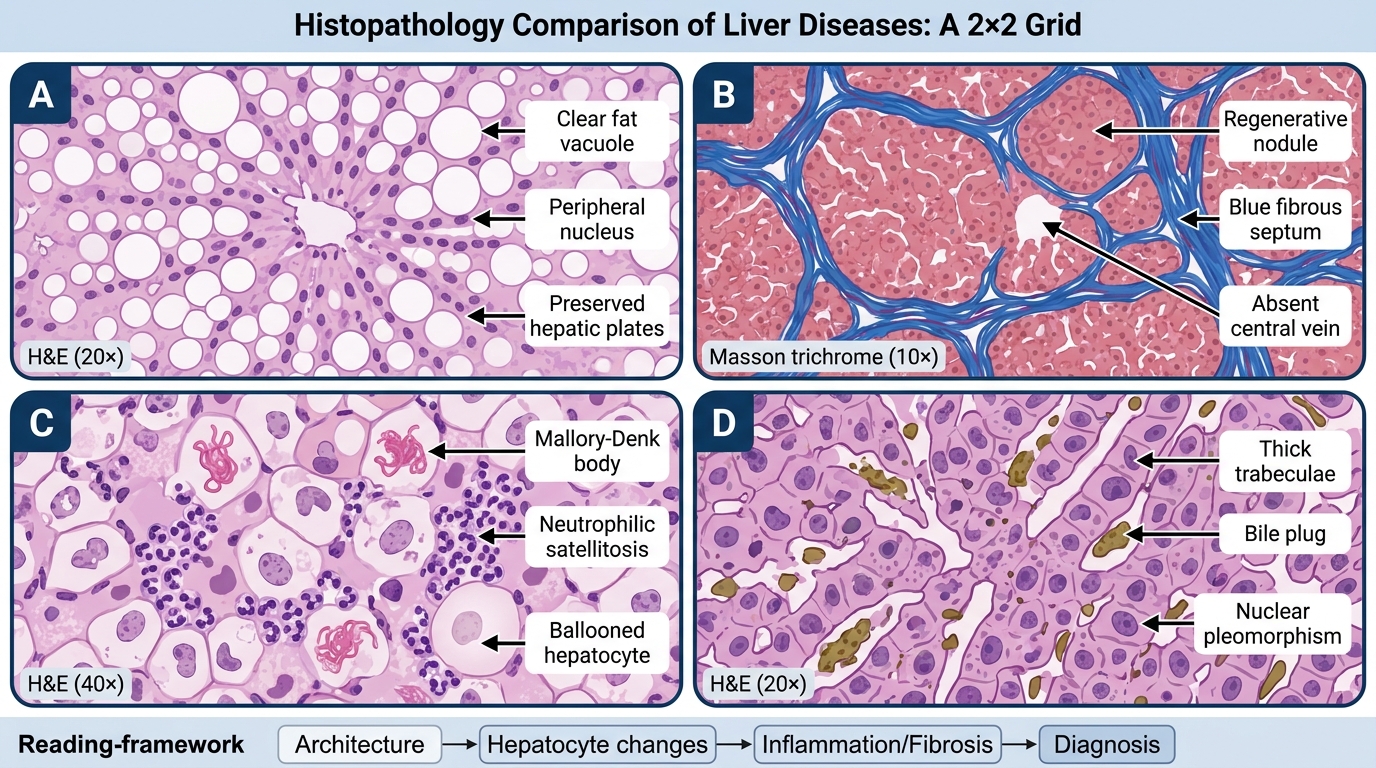
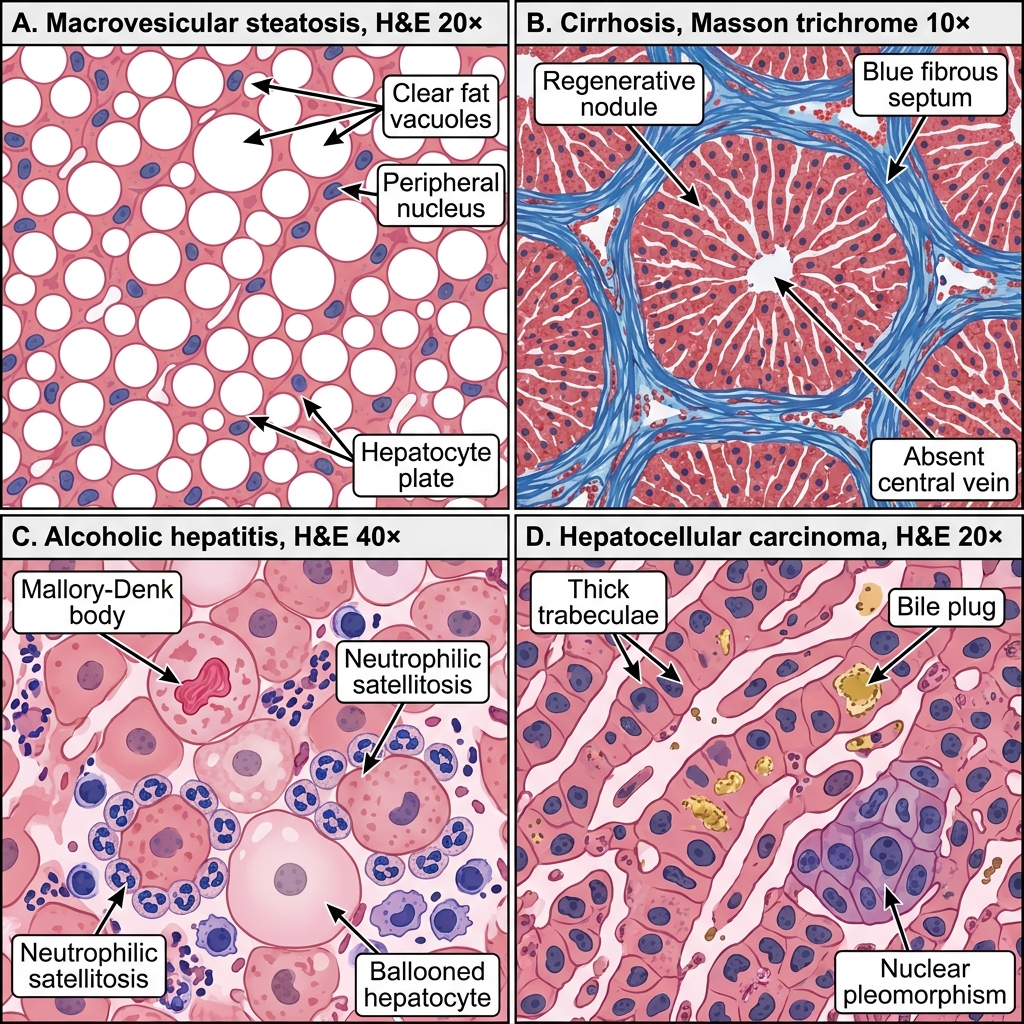
The following composite image shows four liver conditions side-by-side in a 2×2 grid. Use it to practise rapid pattern recognition before attempting the final quiz.
Four-Panel Liver Histology Comparison
For each panel, apply the reading framework: architecture → hepatocyte changes → inflammation/fibrosis → diagnosis. Note how architecture is the first discriminator:
- Panels A and C preserve lobular architecture (disease is ongoing but not yet restructured).
- Panel B has lost it entirely — no central vein, only nodules.
- Panel D shows an entirely different architecture: neoplastic trabeculae replacing normal plates.
Hepatocellular Carcinoma (HCC)
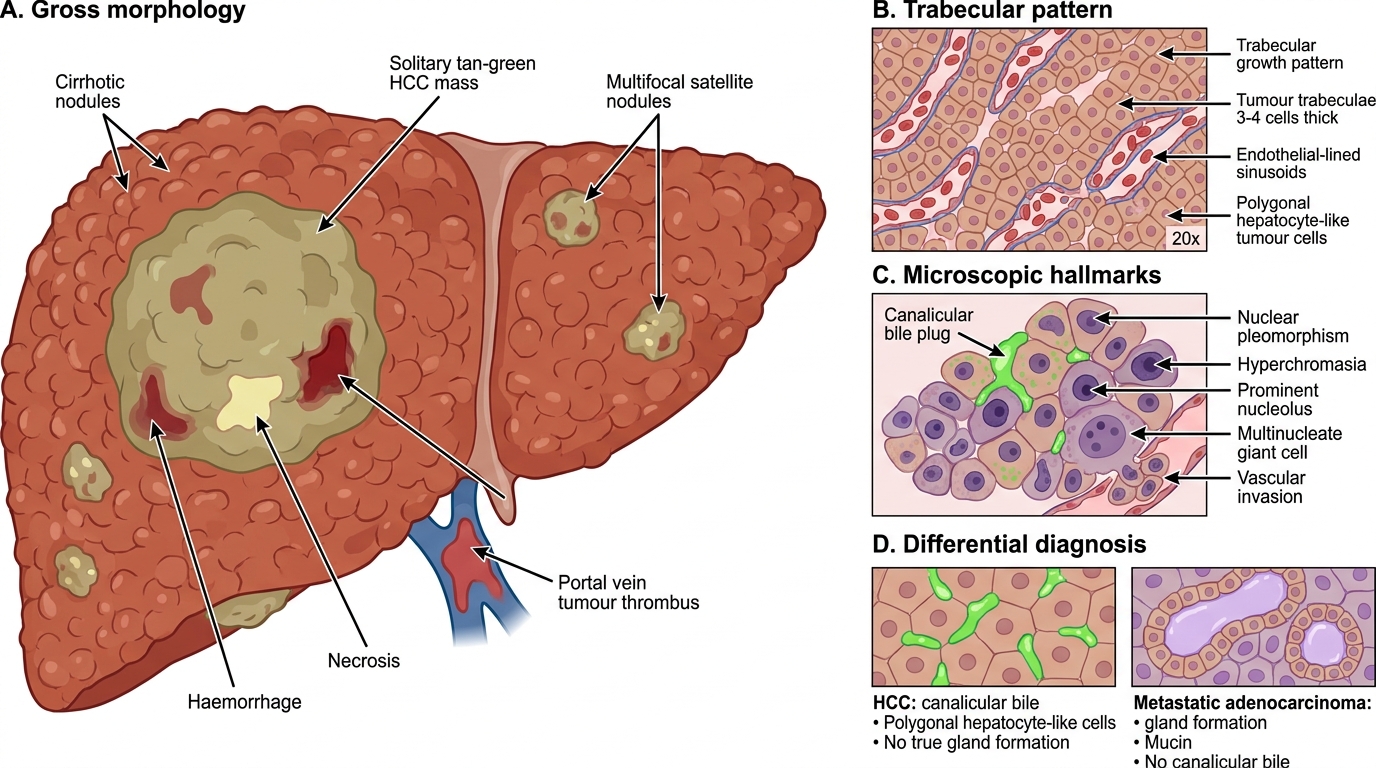
Hepatocellular Carcinoma: Gross and Microscopic Features
HCC is the most common primary liver malignancy; ~85% arise in cirrhotic livers (HBV, HCV, alcohol, NAFLD, haemochromatosis).
Gross:
- Solitary large mass, or multifocal nodules on a cirrhotic background.
- Cut surface: tan-green (bile-producing), haemorrhagic, necrotic.
- Portal vein tumour thrombus — a naked-eye clue to vascular invasion.
Microscopic hallmarks:
1. Trabecular pattern — Tumour cells arranged in trabeculae (plates) 2-20 cells thick, lined by endothelial-like sinusoids. The most common HCC pattern (>80%).
2. Bile production — Bile plugs (green canalicular deposits) within tumour trabeculae. Present in ~50%; pathognomonic of hepatocellular (not cholangiocarcinoma or metastasis) origin.
3. Cellular atypia — Nuclear pleomorphism, hyperchromasia, prominent nucleoli, multinucleate giant cells; loss of nuclear:cytoplasmic ratio regularity.
4. Vascular (sinusoidal) invasion — Tumour cells within vascular channels; associated with satellite nodules and portal vein thrombus.
Growth patterns beyond trabecular: acinar (pseudoglandular, mimics adenocarcinoma), solid/compact, and scirrhous (fibrous stroma).
Distinguishing HCC from metastatic adenocarcinoma: HCC has canalicular bile (not mucin), polygonal cells resembling hepatocytes, and lacks gland formation. IHC: HepPar-1, Arginase-1, GPC3 positive in HCC.
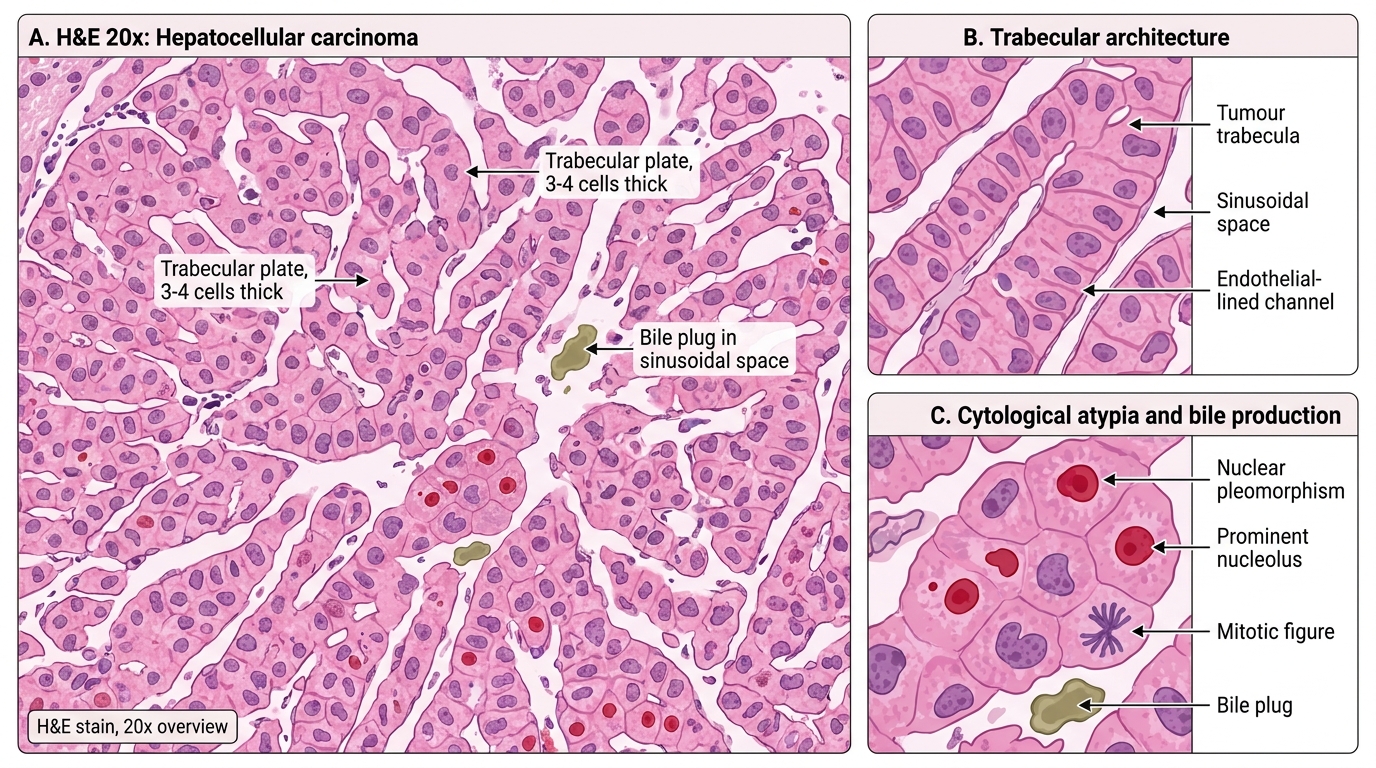
Hepatocellular Carcinoma: Trabecular Pattern on H&E
SELF-CHECK
A liver biopsy from a 60-year-old man with known HCV cirrhosis shows a mass composed of polygonal cells with prominent nucleoli arranged in trabeculae 4-5 cells thick, with green canalicular deposits between tumour cells. Which feature is MOST specific for hepatocellular (rather than cholangiocarcinoma or metastatic) origin?
A. Nuclear pleomorphism and prominent nucleoli
B. Polygonal cell shape
C. Canalicular bile (bile plugs) within tumour trabeculae
D. Vascular invasion
Reveal Answer
Answer: C. Canalicular bile (bile plugs) within tumour trabeculae
Bile production is the most specific marker of hepatocellular differentiation. Bile plugs (green canalicular deposits) represent actual bile secretion by tumour cells — only hepatocytes and HCC can produce bile, not biliary epithelial cells (cholangiocarcinoma) or metastatic adenocarcinoma. Nuclear pleomorphism (A) and vascular invasion (D) are features of malignancy in general. Polygonal shape (B) is a helpful clue but not specific, since some metastases mimic hepatocyte morphology.
Differential Diagnosis at a Glance
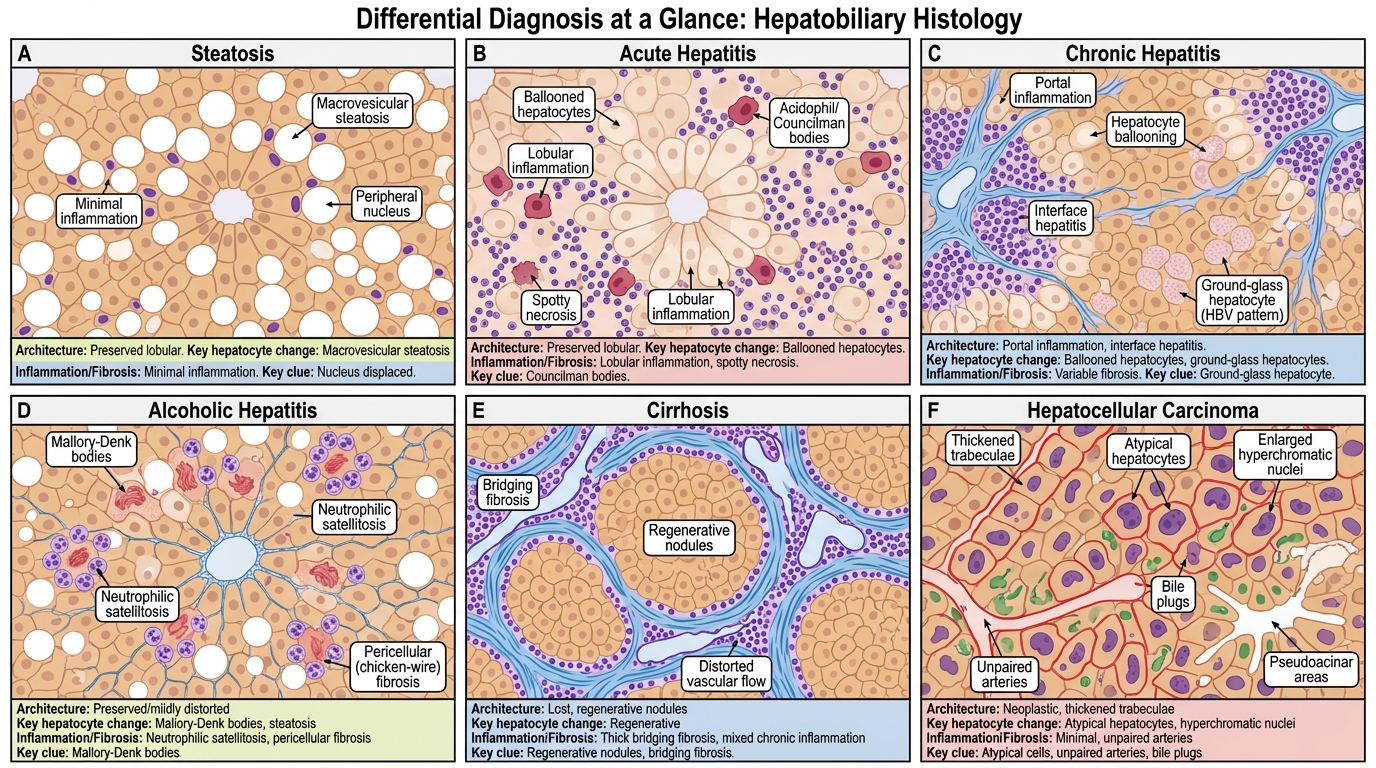
Hepatobiliary Differential Diagnosis at a Glance
A quick-reference comparison across all six conditions:
| Feature | Steatosis | Acute Hepatitis | Chronic Hepatitis | Alcoholic Hepatitis | Cirrhosis | HCC |
|---|---|---|---|---|---|---|
| Architecture | Preserved | Preserved | Preserved → disrupted | Preserved | Lost (nodular) | Neoplastic |
| Key hepatocyte change | Fat vacuoles, peripheral nucleus | Ballooning, Councilman bodies | Ground-glass (HBV), ballooning | Mallory-Denk bodies, ballooning | Regenerative plates | Thick trabeculae, atypia |
| Inflammation | Absent/minimal | Lobular lymphocytes | Portal lymphocytes, interface | Neutrophils (satellitosis) | Variable | Absent/mild |
| Fibrosis | Absent | Absent | Portal → bridging | Perivenular (zone 3) | Diffuse septal | Absent/desmoplastic |
| Specific marker | Lipid on Oil Red O | Councilman body | Ground-glass on orcein | Mallory-Denk bodies | Trichrome septa, reticulin collapse | Bile plugs, HepPar-1 |
Use this table during revision. In practicals, the diagnosis is usually reached after columns 1-4 of the reading framework.