Page 14 of 32
PA24.{5,7} | Portal Hypertension & Hepatocellular Carcinoma — SDL Guide
Learning Objectives
- Define portal hypertension and classify its causes as prehepatic, intrahepatic, and posthepatic.
- Explain the pathogenesis of portal hypertension in terms of increased resistance and increased flow.
- Describe the porto-systemic collaterals and their clinical consequences, including variceal haemorrhage, caput medusae, and haemorrhoids.
- Outline the mechanisms of ascites formation in portal hypertension.
- List the major aetiological factors for hepatocellular carcinoma, with emphasis on HBV, HCV, aflatoxin, and cirrhosis.
- Describe the gross morphological types (unifocal, multifocal, diffuse) and microscopic patterns of HCC.
- Explain the significance of alpha-fetoprotein (AFP) in diagnosis and screening of HCC.
- Recognise the fibrolamellar variant of HCC and its distinctive features.
INSTRUCTIONS
Portal hypertension and hepatocellular carcinoma are among the most important and lethal sequelae of chronic liver disease. In Indian wards you will regularly encounter patients with cirrhosis who present with haematemesis from varices, distended abdomens from ascites, or incidentally detected liver masses — the pathology you study here explains every one of those presentations. A firm grasp of porto-systemic anatomy and HCC biology will directly sharpen your clinical reasoning in medicine and surgery postings.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 18 (Liver, Gallbladder, and Biliary Tract) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 20 (Diseases of Liver) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 48-year-old man with known alcoholic cirrhosis is rushed to the emergency department vomiting bright red blood. He collapses, his haemoglobin is 5.2 g/dL, and gastroscopy reveals three columns of bluish, tortuous veins bulging into the lower oesophagus — one of them actively spurting. Meanwhile, his ultrasound report from three months ago flagged a 3.2 cm hyperechoic nodule in the right lobe and an AFP of 820 ng/mL. Two diseases. One damaged liver. Both explained by the same pathological chain you are about to trace.
WHY THIS MATTERS
Portal hypertension is the engine that drives the most dramatic complications of chronic liver disease — variceal bleeding accounts for up to 30% of mortality in cirrhotics in Indian hospitals. HCC is the fourth leading cause of cancer death globally; India's dual burden of HBV infection and aflatoxin exposure from stored grains makes this doubly relevant. Understanding these diseases is not optional for any clinician who will work in a district or tertiary hospital.
RECALL
Before proceeding, revisit these anchor concepts from Year 1:
- The portal venous system drains the GI tract and spleen into the liver via the portal vein (normal pressure ≈ 5–10 mmHg).
- Porto-systemic anastomoses are pre-existing connections between portal tributaries and systemic veins — normally low-flow, they enlarge when portal pressure rises.
- Sinusoidal blood flow passes from portal triads → sinusoids → central vein → hepatic veins → IVC.
- Starling forces in the peritoneal capillaries: fluid filtration depends on hydrostatic pressure, oncotic pressure, and lymphatic drainage.
- Cirrhosis = diffuse hepatic fibrosis + regenerative nodules, disrupting both architecture and vascular resistance.
Defining Portal Hypertension
Portal Hypertension: Definition, Mechanism, and Classification
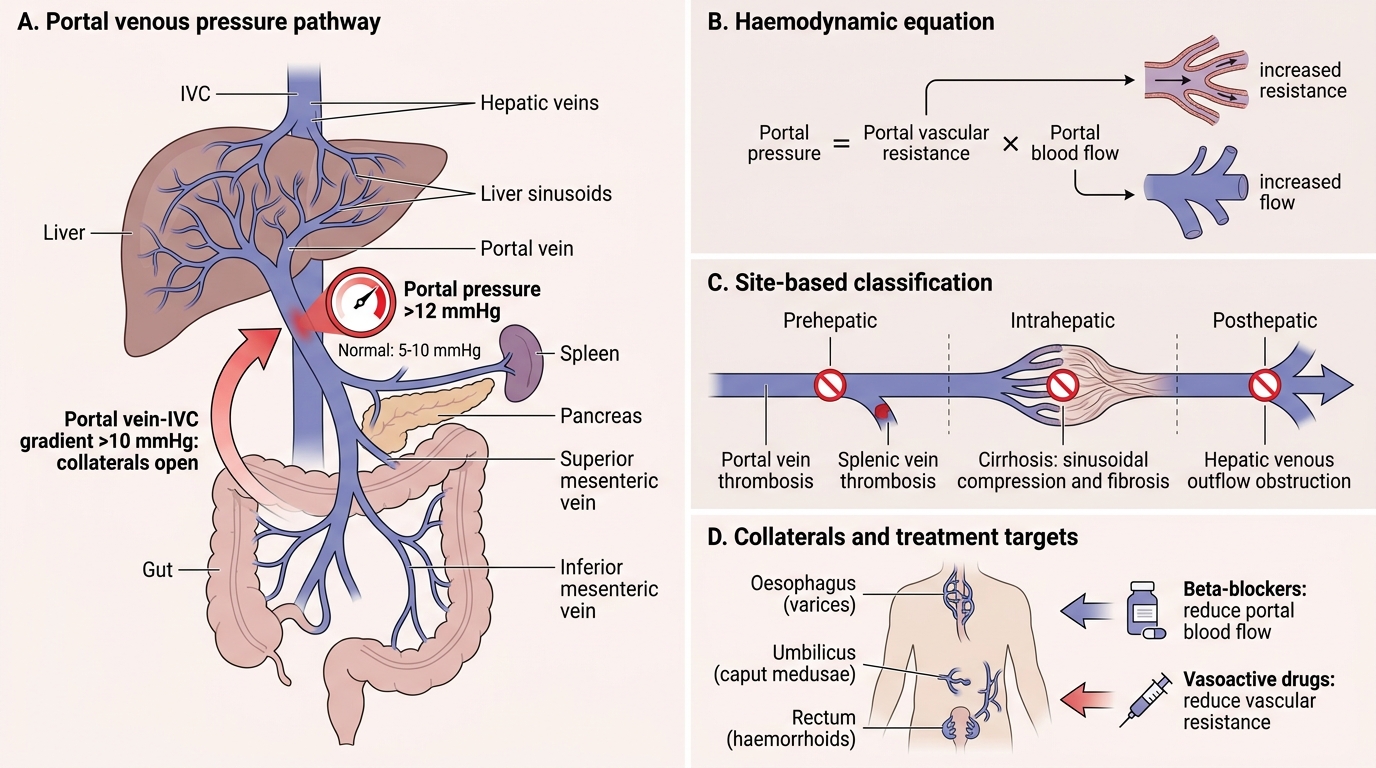
Portal hypertension is sustained elevation of pressure in the portal venous system above 12 mmHg (normal 5–10 mmHg). A gradient >10 mmHg between the portal vein and IVC is the haemodynamic threshold at which porto-systemic collaterals begin to open and complications develop.
The fundamental haemodynamic equation is:
Portal pressure = Portal vascular resistance × Portal blood flow
Most causes act through increased resistance (the denominator), but a secondary hyperdynamic circulation — splanchnic vasodilation mediated by nitric oxide and glucagon — amplifies flow and sustains the hypertension even after partial resistance relief. This dual mechanism is why β-blockers (reducing flow) and vasoactive drugs (reducing resistance) are both used therapeutically.
Classification of Causes by Site
Portal Hypertension: Classification of Causes by Site of Obstruction
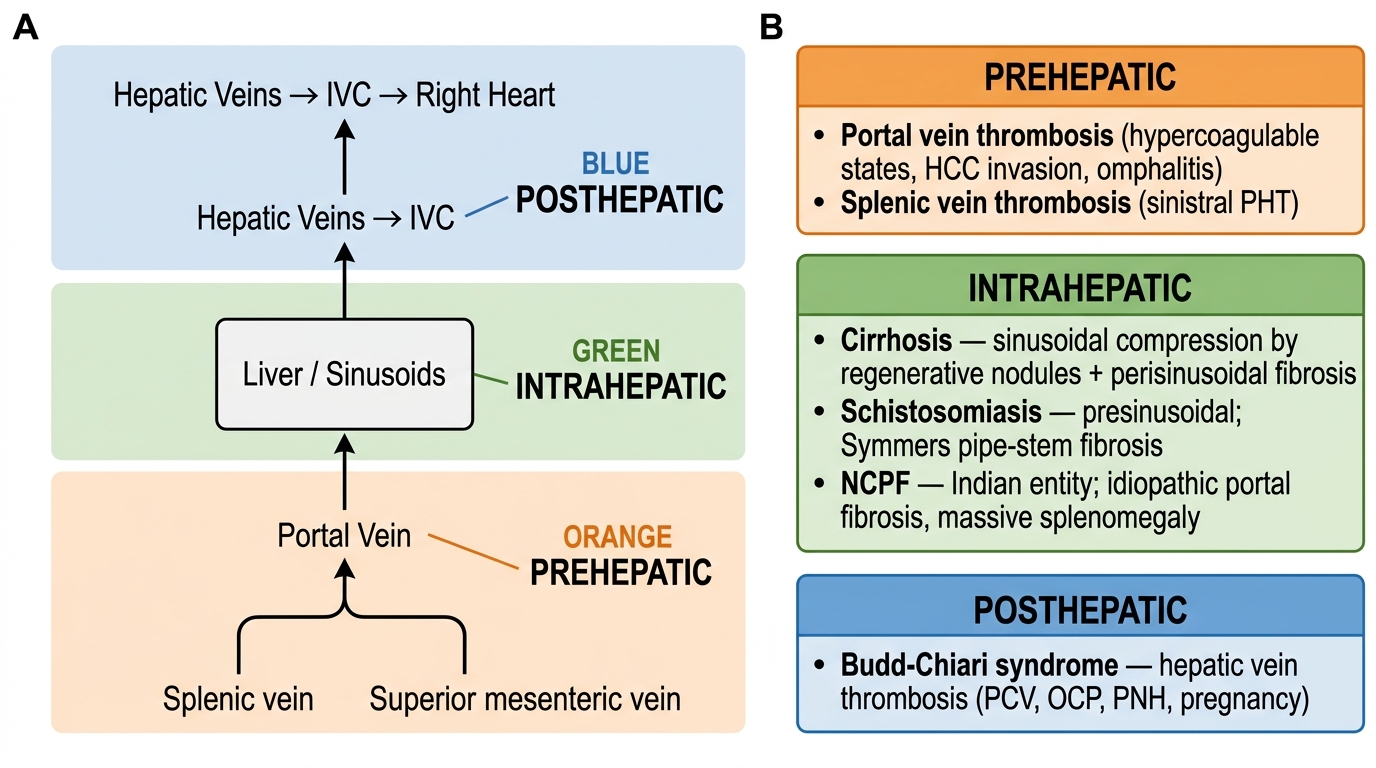
Classifying by the anatomical site of obstruction directs both investigation and management.
Prehepatic (obstruction before the liver)
• Portal vein thrombosis — commonest prehepatic cause; seen with hypercoagulable states, omphalitis in neonates, abdominal sepsis, hepatocellular carcinoma (which invades the portal vein), and polycythaemia vera.
• Splenic vein thrombosis (left-sided, or sinistral, portal hypertension).
Intrahepatic (obstruction within the liver parenchyma)
• Cirrhosis — overwhelmingly the commonest overall cause worldwide; sinusoidal compression by regenerative nodules plus perisinusoidal fibrosis elevates resistance at the sinusoidal level.
• Schistosomiasis (presinusoidal) — Schistosoma mansoni/japonicum eggs deposit in portal tracts, eliciting granulomatous fibrosis and 'pipe-stem' (Symmers' fibrosis). Critical in sub-Saharan Africa and Egypt; seen in endemic pockets in India.
• Non-cirrhotic portal fibrosis (NCPF) — Indian-specific entity; idiopathic portal fibrosis without nodule formation, presents with massive splenomegaly.
• Hepatic vein involvement: Budd-Chiari syndrome (see posthepatic).
Posthepatic (obstruction after the liver, impeding hepatic venous outflow)
• Budd-Chiari syndrome — hepatic vein thrombosis (classically from polycythaemia vera, OCP, pregnancy, paroxysmal nocturnal haemoglobinuria). Acute form: painful hepatomegaly, ascites, jaundice. Chronic: centrizonal fibrosis.
• Right heart failure (RHF) and constrictive pericarditis — raised central venous pressure transmitted retrogradely through the IVC into hepatic veins ('cardiac cirrhosis' in long-standing RHF).
• IVC obstruction (membranous obstruction of IVC — endemic in South Africa, Japan, India).
SELF-CHECK
A 30-year-old woman on oral contraceptive pills presents with sudden painful hepatomegaly, ascites, and markedly raised hepatic venous pressure gradient. The liver biopsy shows centrizonal congestion and fibrosis with no portal tract involvement. The most likely diagnosis is:
A. Portal vein thrombosis
B. Non-cirrhotic portal fibrosis
C. Budd-Chiari syndrome
D. Schistosomal hepatic fibrosis
Reveal Answer
Answer: C. Budd-Chiari syndrome
Budd-Chiari syndrome (hepatic vein thrombosis) is strongly associated with prothrombotic states including OCP use and pregnancy. It causes posthepatic portal hypertension. The histological hallmark is centrizonal (zone 3) congestion and fibrosis because zone 3 hepatocytes are drained by the central vein that is obstructed. Portal vein thrombosis would show prehepatic pattern; NCPF and schistosomiasis are presinusoidal intrahepatic causes and do not show centrizonal fibrosis.
Porto-Systemic Collaterals and Their Complications
Porto-Systemic Collaterals in Portal Hypertension
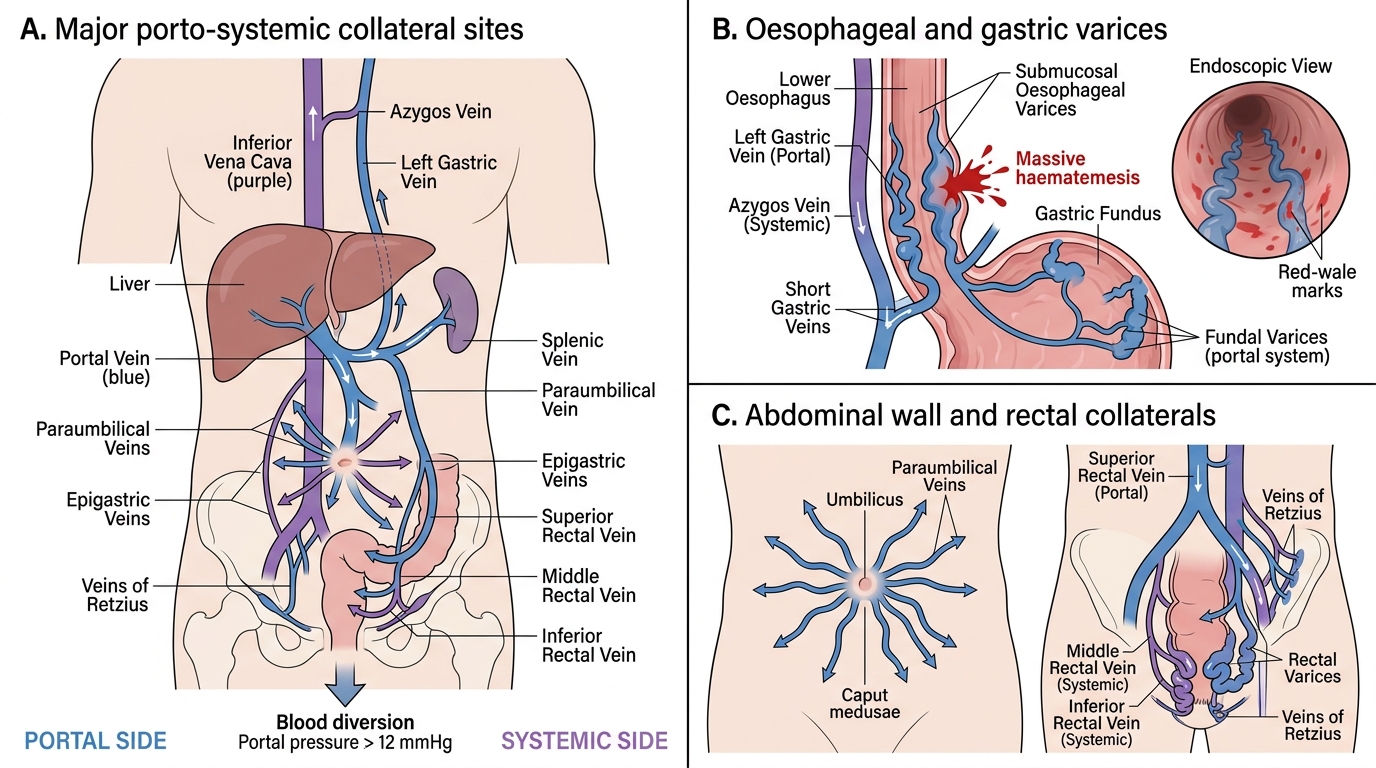
When portal pressure is sustained above 12 mmHg, pre-existing microscopic porto-systemic connections dilate to form clinically significant collaterals. Each connection site produces characteristic clinical findings.
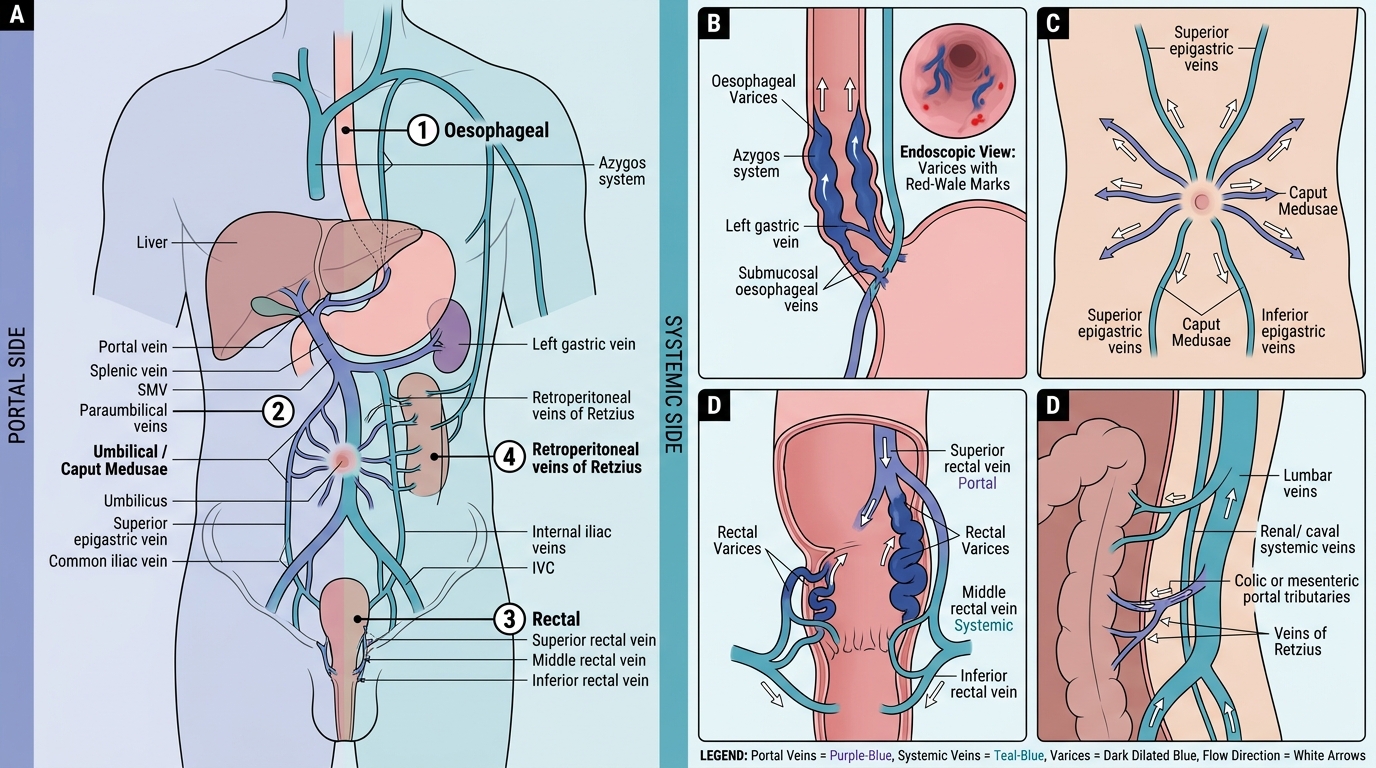
Porto-Systemic Anastomoses in Portal Hypertension
1. Oesophageal and gastric varices — left gastric (coronary) vein connects to the azygos system via submucosal oesophageal veins. These become oesophageal varices, visible as tortuous blue columns in the lower oesophagus on endoscopy. Gastric fundal varices form via short gastric veins. Rupture causes massive haematemesis — this is the single most important and most lethal complication of portal hypertension, accounting for ~30% of deaths in cirrhotics. Risk of rupture rises with variceal size and the presence of 'red-wale marks'.
2. Caput medusae — dilated para-umbilical veins radiate from the umbilicus across the abdominal wall, reconnecting with the umbilical remnant. Named after Medusa's serpentine hair; clinically they appear as dilated veins visible under the abdominal skin, with flow directed away from the umbilicus (distinguishes from IVC obstruction where flow is upward).
3. Rectal varices / haemorrhoids — superior rectal vein (portal) connects to middle and inferior rectal veins (systemic, internal iliac). Dilation produces rectal varices; lower rectal involvement may mimic haemorrhoids but true portal haemorrhoids differ from common haemorrhoids.
4. Retroperitoneal (veins of Retzius) and spleno-renal shunts — lesser clinical significance but contribute to the collateral network.