Page 17 of 32
PA24.{5,7} | Portal Hypertension & Hepatocellular Carcinoma — SDL Guide (Part 4)
Microscopic Patterns of HCC
Microscopic Patterns of Hepatocellular Carcinoma
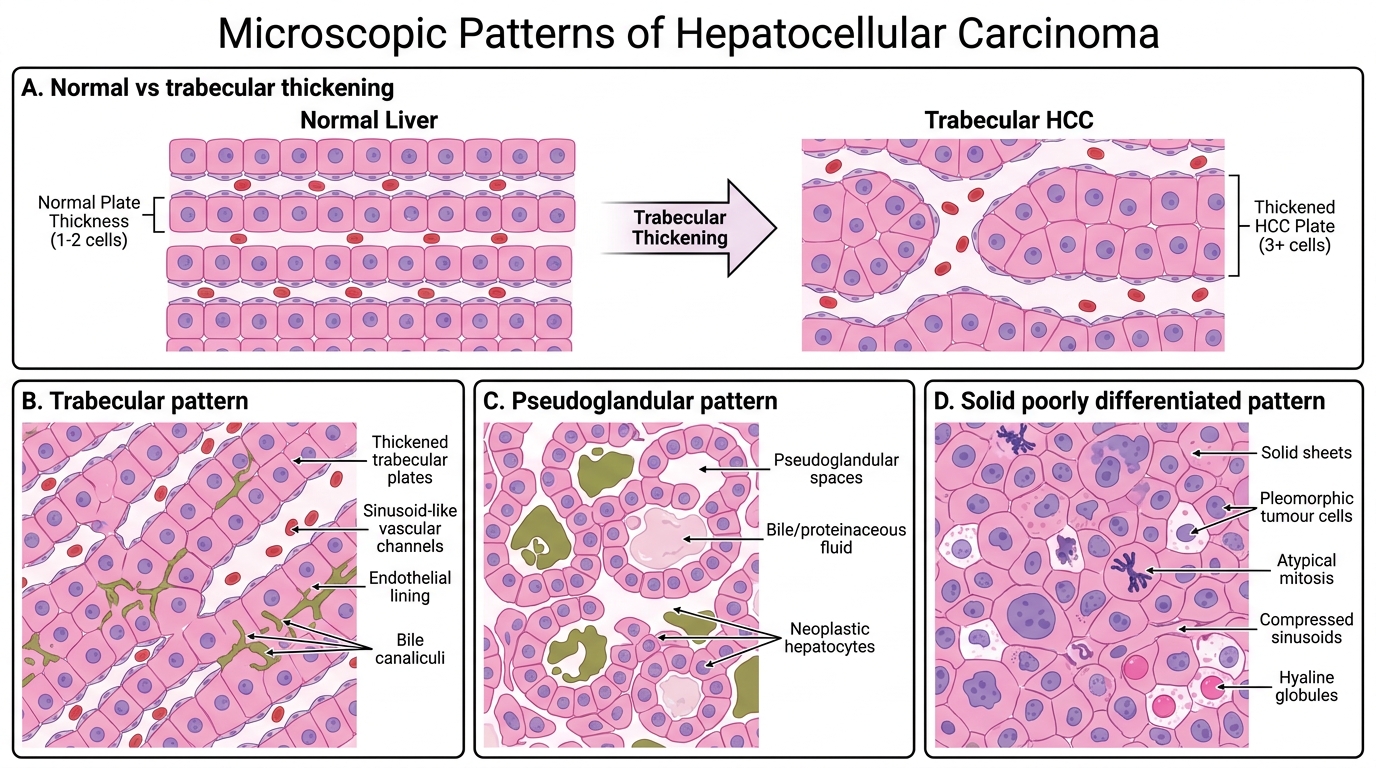
Histological examination shows neoplastic hepatocytes arranged in various patterns, recapitulating (imperfectly) normal liver architecture.
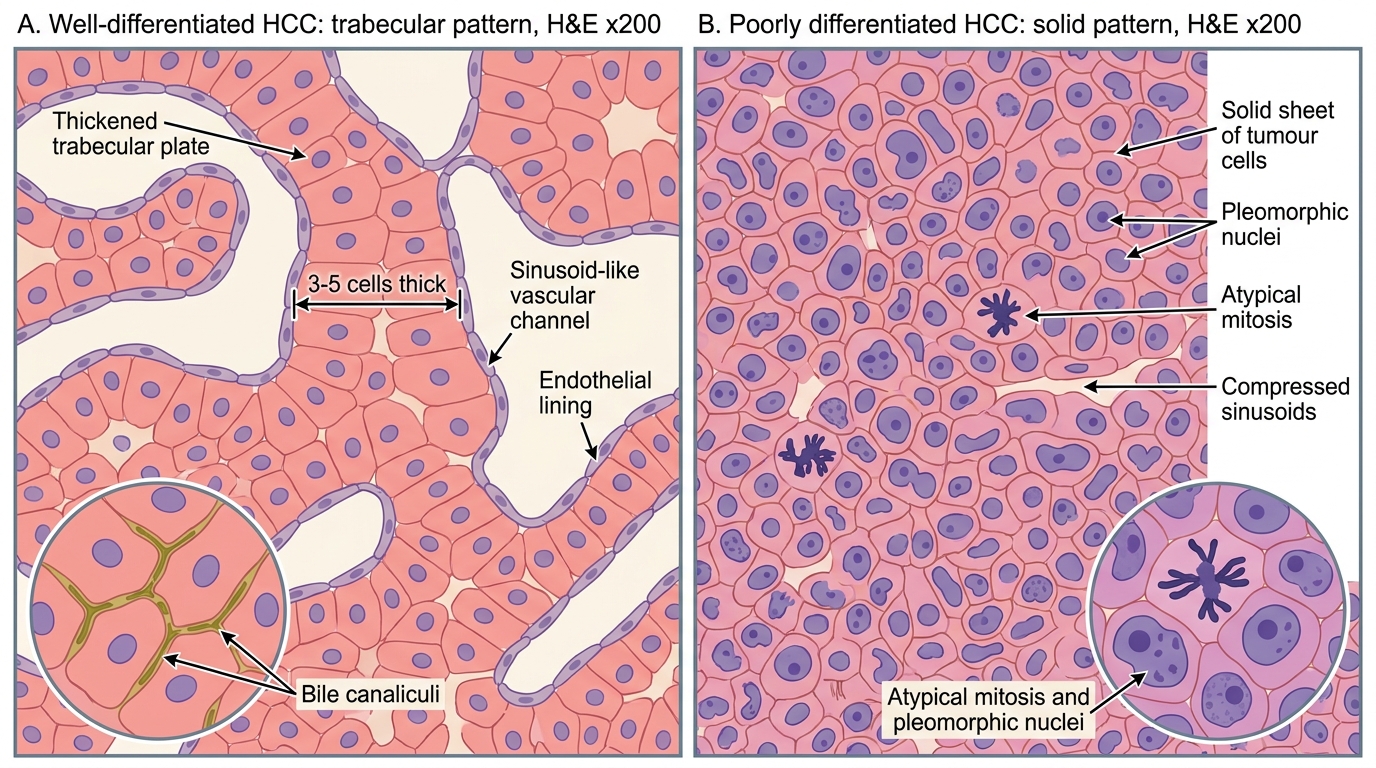
Trabecular (sinusoidal) pattern — commonest; tumour cells form plates 2–3 (or more) cells thick, separated by sinusoid-like vascular channels lined by endothelial cells. Normal liver plates are only 1–2 cells thick — thickened plates are a diagnostic clue.
Pseudoglandular (acinar) pattern — tumour cells form gland-like spaces containing bile or proteinaceous fluid.
Solid (compact) pattern — sheets of cells with compressed sinusoids; seen in poorly differentiated tumours.
Cytological features:
• Cells resemble hepatocytes: abundant eosinophilic cytoplasm, central nucleus, prominent nucleolus.
• Bile production within tumour cells — pathognomonic of hepatocellular origin (distinguishes from metastatic adenocarcinoma, cholangiocarcinoma).
• Intracellular hyaline globules (α1-antitrypsin or fibrinogen), Mallory hyaline.
• In poorly differentiated HCC, cells may be pleomorphic, giant, or clear-cell type.
Microscopic Patterns of Hepatocellular Carcinoma
SELF-CHECK
A liver biopsy in a 55-year-old man shows thickened hepatocyte plates (3–4 cells thick) separated by sinusoid-like channels. Tumour cells have abundant eosinophilic cytoplasm and some contain greenish intracellular deposits. AFP is 1,200 ng/mL. The microscopic finding that MOST specifically confirms hepatocellular origin of this carcinoma is:
A. Prominent nucleoli in tumour cells
B. Intracellular bile production
C. Elevated serum AFP
D. Trabecular growth pattern
Reveal Answer
Answer: B. Intracellular bile production
Intracellular bile production is pathognomonic of hepatocellular differentiation — no other tumour type produces bile. Trabecular pattern and prominent nucleoli are characteristic but not exclusive to HCC. Elevated AFP supports the diagnosis but is a serum marker, not a histological finding. AFP can also be raised in germ cell tumours and, less markedly, in hepatic metastases.
Alpha-Fetoprotein, Screening, and Complications
AFP Screening and Complications in HCC
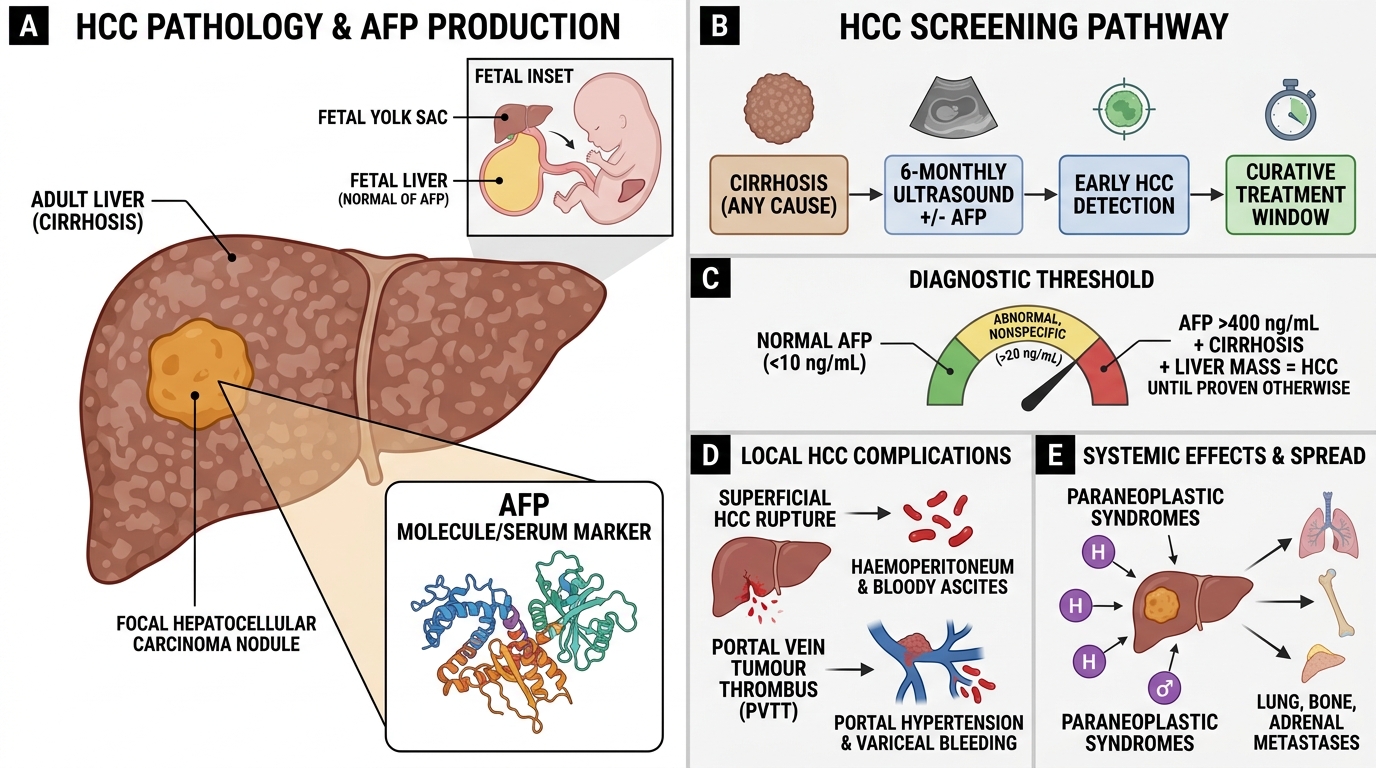
Alpha-fetoprotein (AFP) is a glycoprotein normally produced by the fetal yolk sac and liver; it is virtually absent in adults (normal < 10 ng/mL). In HCC, AFP is elevated in ~70% of cases.
Diagnostic thresholds:
• AFP > 400 ng/mL in a cirrhotic with a liver mass = HCC until proved otherwise (Barcelona BCLC criteria).
• AFP > 20 ng/mL is abnormal but not specific (also elevated in germ cell tumours, hepatic regeneration, hepatitis).
Screening protocol in cirrhotics: 6-monthly ultrasound ± AFP in all patients with cirrhosis (any cause). This detects HCC at an earlier, potentially curative stage. Cost-effective even in resource-limited settings.
Complications of HCC:
• Tumour rupture → haemoperitoneum — spontaneous rupture of a superficial HCC causes acute abdominal pain, circulatory collapse, and bloody ascites; mortality > 50% without emergency intervention.
• Portal vein invasion — PVTT precipitates acute portal hypertension, variceal haemorrhage.
• Paraneoplastic syndromes — hypoglycaemia (ectopic IGF-II or insulin-like activity), hypercalcaemia (ectopic PTHrP), polycythaemia (ectopic erythropoietin), hypercholesterolaemia.
• Metastases — haematogenous to lungs, bone, adrenals.
Fibrolamellar Variant of HCC
Fibrolamellar Variant of Hepatocellular Carcinoma
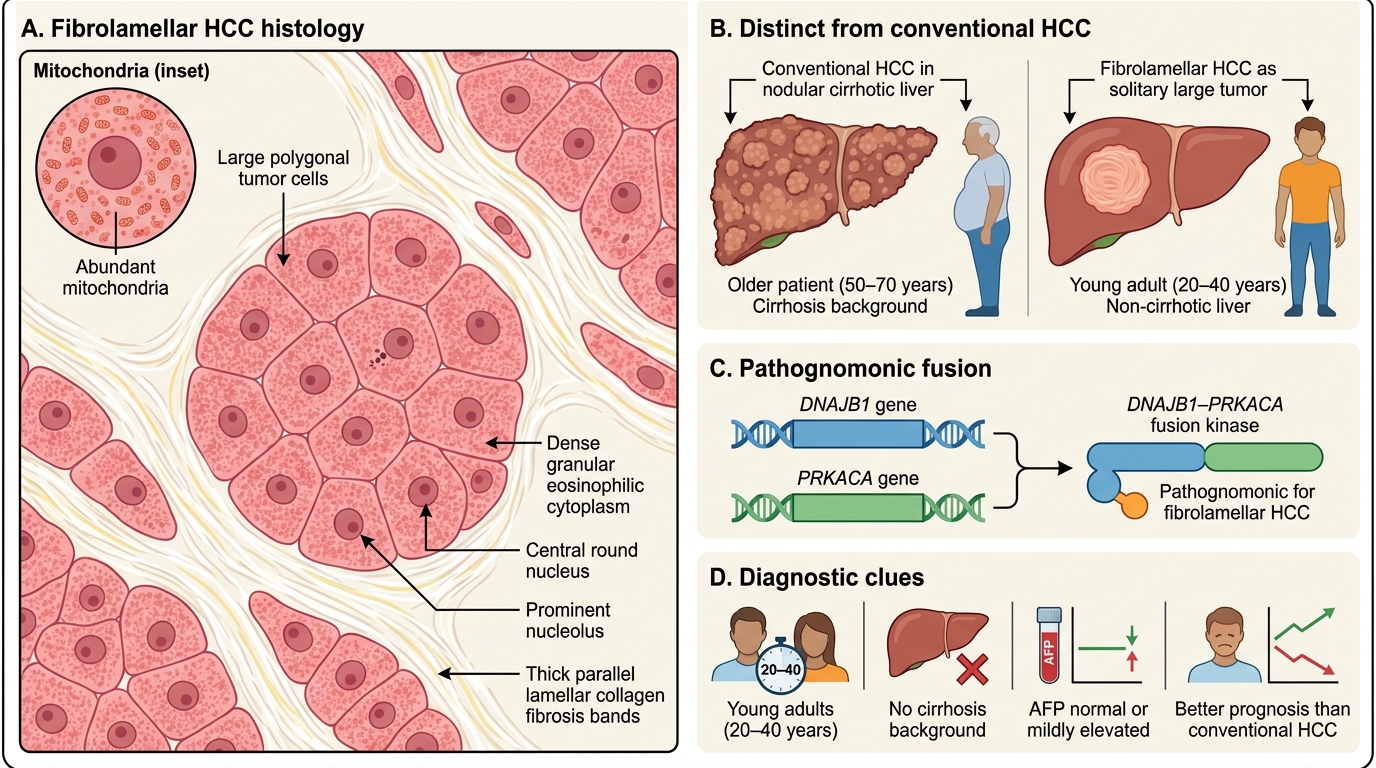
The fibrolamellar HCC is a distinct clinicopathological entity — not a subtype of conventional HCC but a separate tumour with different biology, demographics, and prognosis.
Key distinctions from conventional HCC:
| Feature | Conventional HCC | Fibrolamellar HCC |
|---|---|---|
| Age | Middle-aged/elderly | Young adults (20–40 yr) |
| Cirrhosis background | Yes (>80%) | No |
| AFP | Elevated ~70% | Normal or mildly elevated |
| Morphology | See above | Large polygonal cells with dense granular eosinophilic cytoplasm (abundant mitochondria), separated by dense lamellar fibrosis bands |
| Molecular driver | TP53, TERT, HBx | DNAJB1–PRKACA fusion (pathognomonic) |
| Prognosis | Poor (overall 5-yr <15%) | Relatively better if resectable |
Pathognomonic molecular feature: The DNAJB1–PRKACA fusion gene (created by a focal deletion on chr 19) is present in virtually 100% of fibrolamellar HCC and absent in conventional HCC — diagnostic on molecular testing when histology is ambiguous.
SELF-CHECK
A 24-year-old non-drinker with no viral hepatitis markers presents with a solitary 8 cm liver mass and a normal AFP. Histology shows large polygonal hepatocytes with deeply eosinophilic granular cytoplasm arranged in nests separated by parallel bands of dense fibrous stroma. The molecular alteration MOST characteristic of this tumour is:
A. TP53 codon-249 mutation
B. TERT promoter mutation
C. DNAJB1–PRKACA fusion
D. HBx protein integration
Reveal Answer
Answer: C. DNAJB1–PRKACA fusion
The clinical and histological description is classic for fibrolamellar HCC — young patient, no cirrhosis, normal AFP, lamellar fibrosis. The DNAJB1–PRKACA fusion gene, created by a focal deletion on chromosome 19, is present in virtually 100% of fibrolamellar HCCs and is absent in conventional HCC. TP53 R249S is the aflatoxin signature; TERT promoter mutation is the commonest alteration in conventional HCC; HBx integration is the HBV-related carcinogenesis mechanism.