Page 16 of 32
PA24.{5,7} | Portal Hypertension & Hepatocellular Carcinoma — SDL Guide (Part 3)
Aetiology of Hepatocellular Carcinoma
Aetiology of Hepatocellular Carcinoma
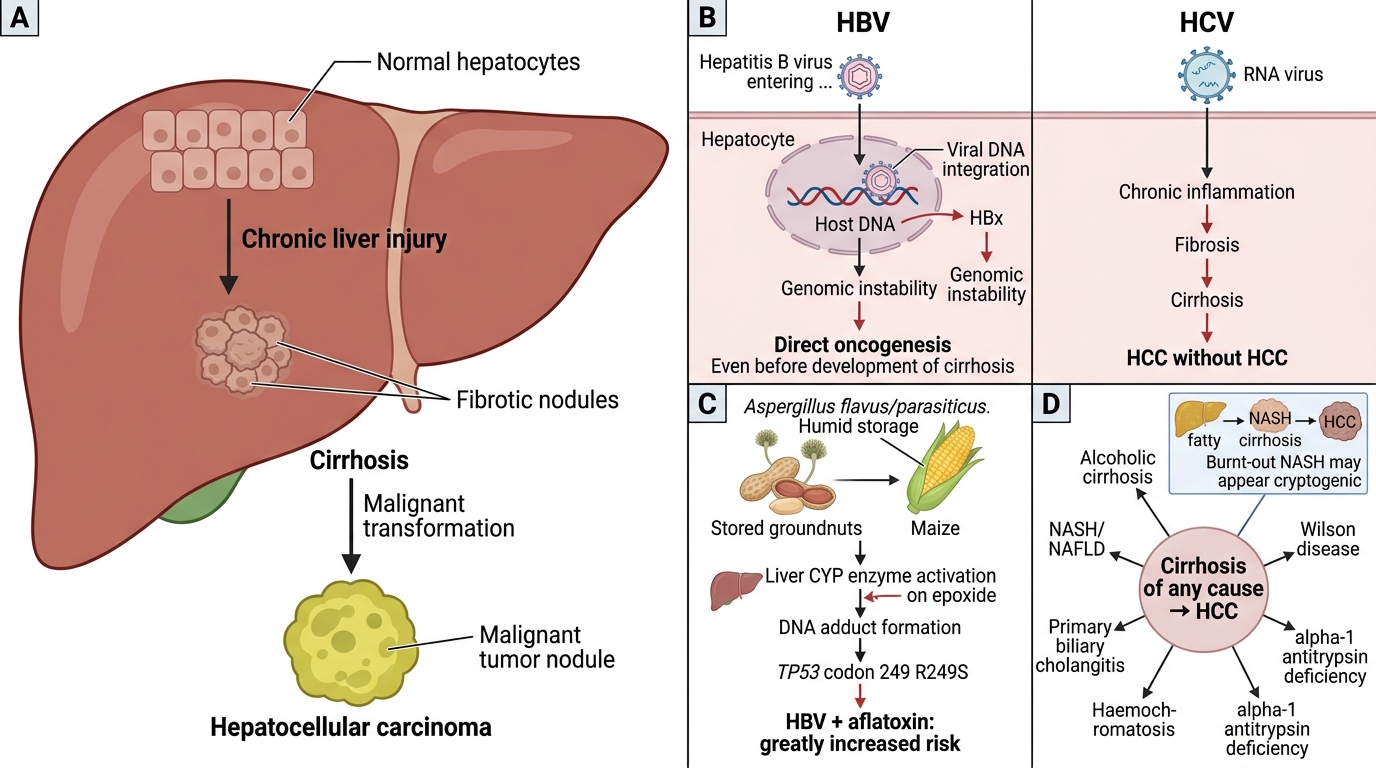
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy, arising from hepatocytes. It almost always arises on a background of chronic liver injury.
Major aetiological factors:
- Chronic HBV infection — globally most important cause; integrates viral DNA (HBx protein) into the hepatocyte genome, causing genomic instability and direct oncogenesis even before cirrhosis. In India, HBV accounts for ~50% of HCC cases.
- Chronic HCV infection — predominantly through cirrhosis-mediated oncogenesis (unlike HBV, HCV does not integrate into DNA); ~25% of HCC in India.
- Aflatoxin B1 — produced by Aspergillus flavus/parasiticus contaminating stored groundnuts and grain (maize, sorghum) in humid conditions. Critically relevant in India, sub-Saharan Africa, and South-East Asia. Aflatoxin B1 is activated by CYP enzymes to an epoxide that causes a specific TP53 codon-249 mutation (R249S). Synergistic with HBV — the combination raises risk ~60-fold.
- Cirrhosis of any cause — alcoholic cirrhosis, NASH-related cirrhosis (rising rapidly with the obesity epidemic), haemochromatosis (10–30% lifetime risk in homozygotes), α1-antitrypsin deficiency, primary biliary cholangitis, Wilson's disease.
- Alcohol — acts primarily through cirrhosis; no direct carcinogenic effect equivalent to aflatoxin.
- NASH/NAFLD — now a major driver in non-drinkers; 'cryptogenic' cirrhosis progressing to HCC often represents burnt-out NASH.
Pathogenesis — From Cirrhosis to Carcinoma
Pathogenesis of Hepatocellular Carcinoma
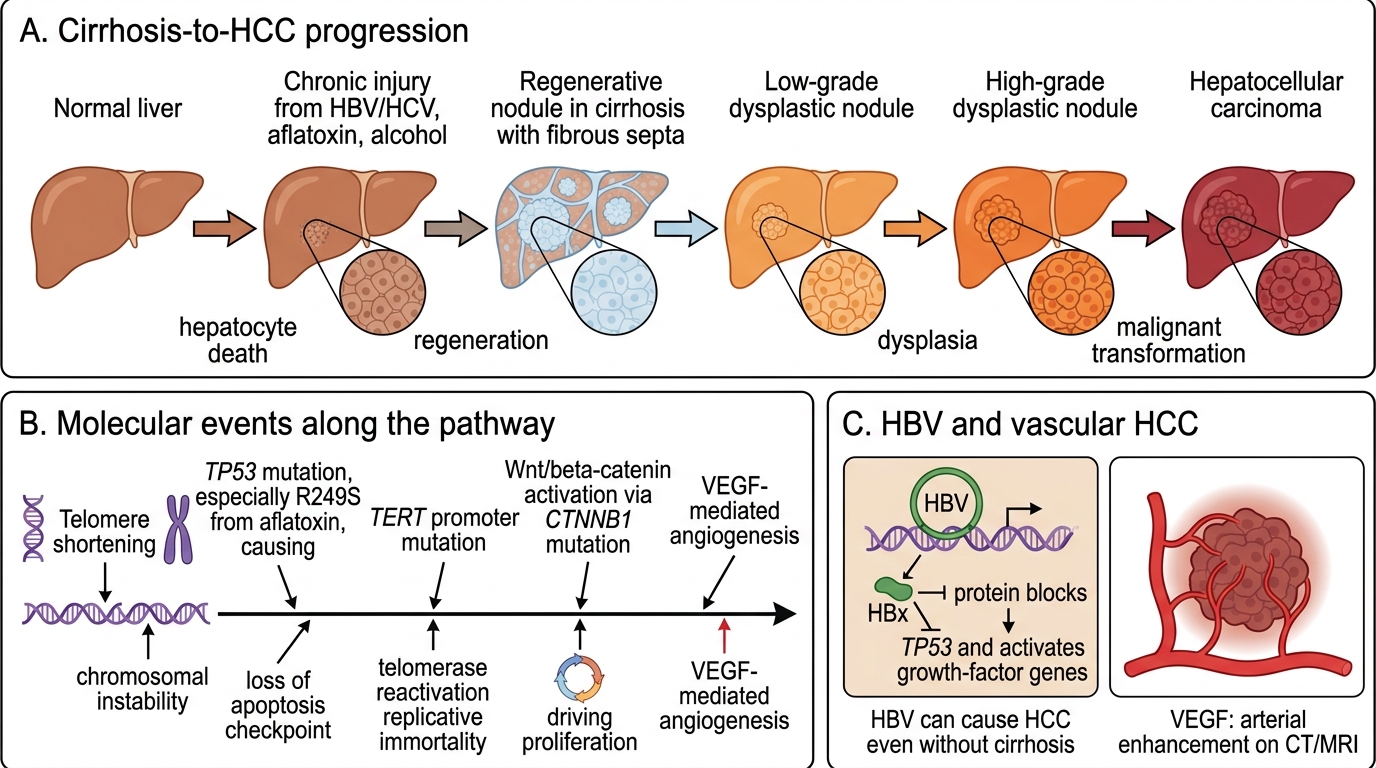
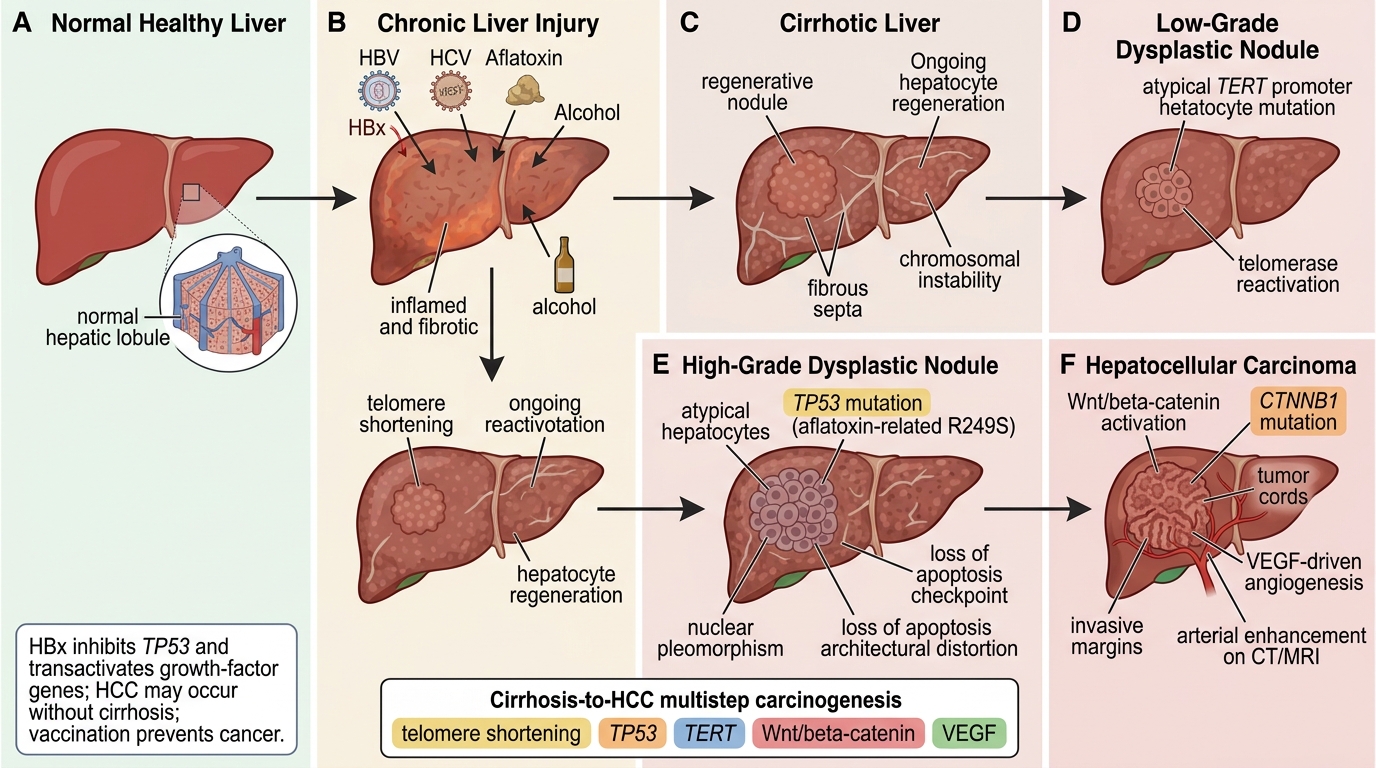
The dominant pathway is: chronic injury → hepatocyte death → regenerative nodules → dysplastic nodules → HCC.
Cirrhosis-to-Hepatocellular Carcinoma Progression
Key molecular events:
• Telomere shortening in regenerating hepatocytes → chromosomal instability.
• TP53 mutation (especially R249S from aflatoxin) — loss of apoptosis checkpoint.
• TERT promoter mutation — the commonest somatic mutation in HCC (~60%); reactivates telomerase, conferring replicative immortality.
• Wnt/β-catenin activation (~30%) — CTNNB1 mutations drive proliferation.
• VEGF and angiogenic signals — HCC is highly vascular (exploited in imaging: arterial enhancement on CT/MRI).
In HBV-related HCC, the HBx protein transactivates growth-factor genes and inhibits TP53 directly, enabling oncogenesis even without cirrhosis — explaining why HBV vaccination in childhood is a genuine cancer prevention strategy.
Gross Morphology of HCC
Gross Morphology and Vascular Invasion of HCC
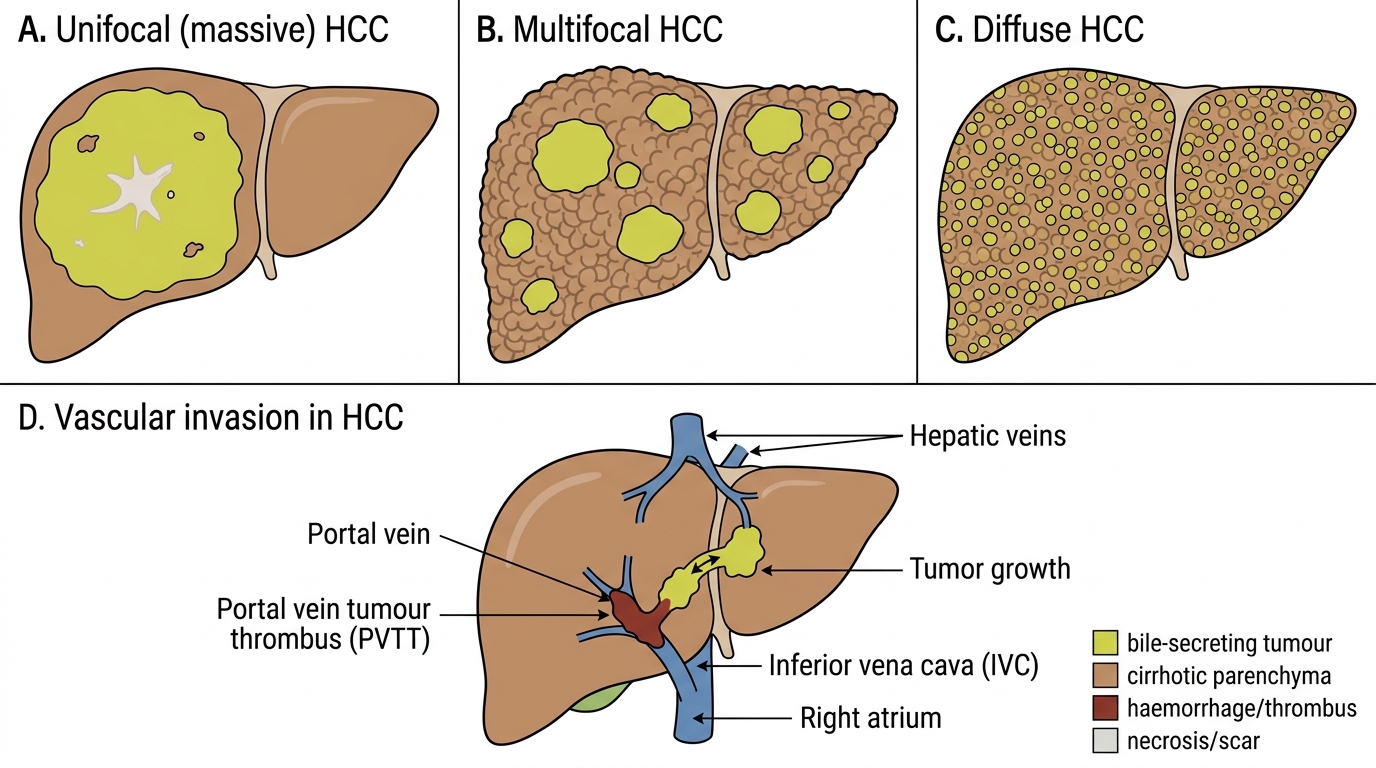
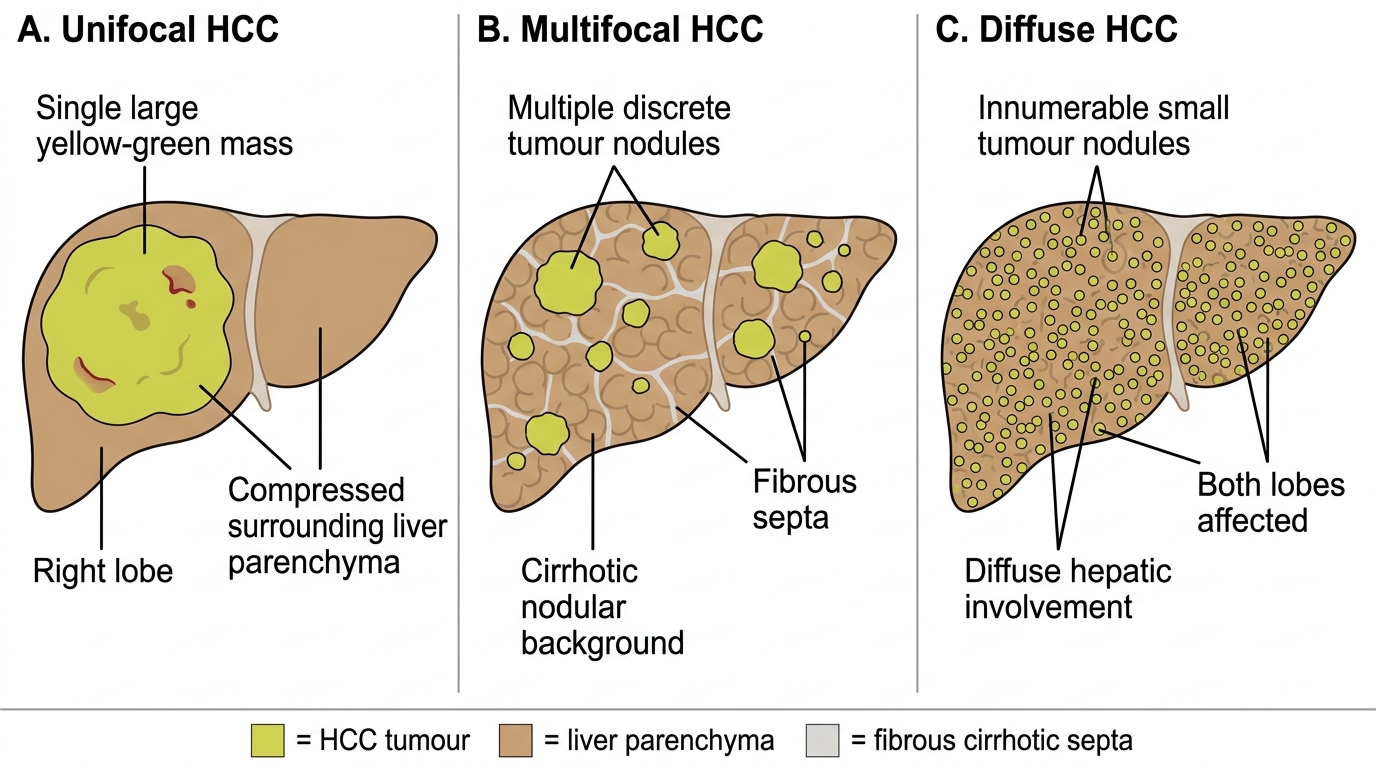
Three gross patterns are recognised:
1. Unifocal (massive) — single large tumour, often replacing an entire lobe; commonest in younger patients with HBV without established cirrhosis. May show a central scar or areas of necrosis.
2. Multifocal — multiple discrete nodules of varying size scattered throughout the liver; typically in a cirrhotic background, arising from independent foci of transformation ('multicentric origin') or intrahepatic satellite metastases.
3. Diffuse — innumerable small tumour nodules permeating the entire liver, mimicking cirrhotic nodules macroscopically; difficult to diagnose radiologically.
Colour: Yellow-green (bile-secreting), green-brown, or white with haemorrhagic foci.
Gross Types of Hepatocellular Carcinoma
Vascular invasion: HCC has a striking propensity to invade vascular channels — particularly the portal vein (portal vein tumour thrombus, PVTT) and hepatic veins. PVTT exacerbates portal hypertension, worsens ascites, and carries a dire prognosis. Tumour may extend into the IVC and right atrium.