Page 6 of 32
PA24.3 | Viral & Toxic Hepatitis — SDL Guide
Learning Objectives
- List the hepatotropic viruses (A–E) and classify each by genome type, transmission route, and chronicity potential
- Describe the immune-mediated pathogenesis of hepatocyte injury in hepatitis B
- Identify the microscopic hallmarks of acute hepatitis (ballooning degeneration, Councilman bodies, spotty necrosis) and chronic hepatitis (interface hepatitis, ground-glass hepatocytes, fibrosis staging)
- Explain the clinical phases, outcomes, and complications of viral hepatitis including fulminant hepatic failure, carrier state, and HCC risk
- Distinguish predictable from idiosyncratic drug-induced liver injury with examples, and outline the paracetamol toxicity mechanism
- Differentiate viral, toxic, and autoimmune hepatitis using clinical features, laboratory findings, and serology
INSTRUCTIONS
Hepatitis means inflammation of the liver — but not all hepatitis is the same. In the emergency ward you will see a jaundiced student who took 20 paracetamol tablets; in the OPD a 45-year-old who has been a 'silent' hepatitis B carrier for two decades and now has early cirrhosis. This module unpacks how five different viruses and a diverse array of drugs each reach the same endpoint — hepatocyte death — by entirely different mechanisms, and how you can tell them apart at the bedside, in the lab, and under the microscope.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 18 (Liver) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 20 (textbook)
- WHO Hepatitis B & C Fact Sheets (2023) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old dental student presents to the casualty at 3 AM with sudden-onset jaundice, fever, and nausea after returning from a camp two weeks ago. His roommate had a similar illness last month. Simultaneously, a 48-year-old bus driver is admitted with haematemesis; incidental labs show ALT 680 U/L, HBsAg positive for 'years'. Same organ, same yellow skin — but entirely different stories. By the end of this module, you will know not just what is happening to each liver but why — and how to tell them apart before the serology returns.
WHY THIS MATTERS
India carries one of the world's largest burdens of viral hepatitis: ~4 crore people live with chronic hepatitis B, and hepatitis C affects ~60 lakh. Together they drive the majority of cirrhosis and hepatocellular carcinoma (HCC) cases you will encounter in a busy tertiary hospital. Drug-induced liver injury (DILI) is the leading cause of acute liver failure in paracetamol-overdose countries — and is entirely preventable. Understanding hepatitis at the mechanistic level lets you explain prognosis to patients, order the right serology, and identify the rare but fatal fulminant case before it deteriorates.
RECALL
Before diving in, activate your Year-1 foundations:
- Hepatocyte anatomy — hepatic acinus zones 1-3; zone 3 (centrilobular) is most susceptible to ischaemia and paracetamol toxicity.
- Kupffer cells — resident hepatic macrophages; your first line of innate defence.
- Bilirubin metabolism — conjugated vs unconjugated; how hepatocyte damage raises both transaminases (AST, ALT) and bilirubin.
- Apoptosis vs necrosis — apoptosis = shrinkage + dense body, necrosis = swelling + cell lysis. You will see both in the same section of hepatitis biopsy.
- Immune memory — CD8⁺ cytotoxic T cells recognise MHC-I-presented viral peptides. This is the engine of HBV-driven hepatocyte killing.
The Hepatotropic Viruses at a Glance
The Hepatotropic Viruses at a Glance
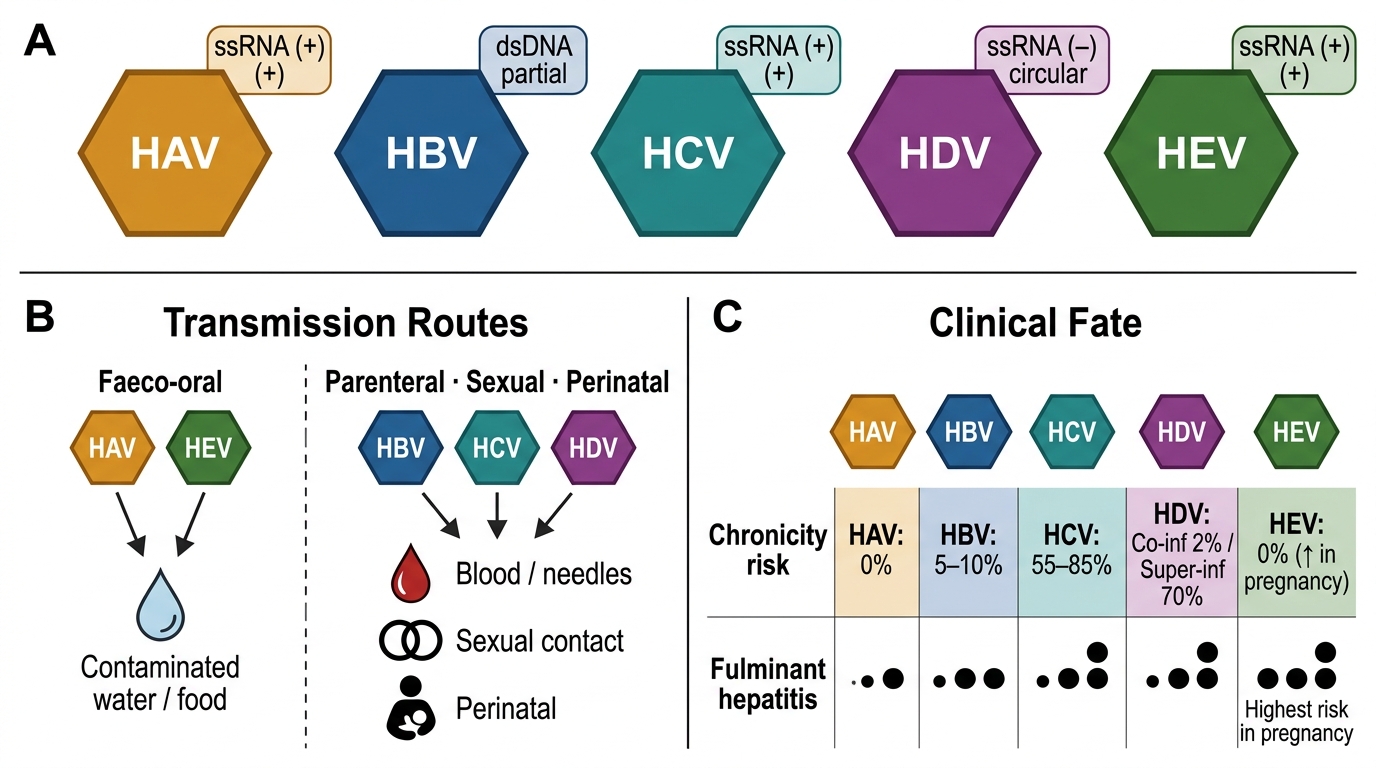
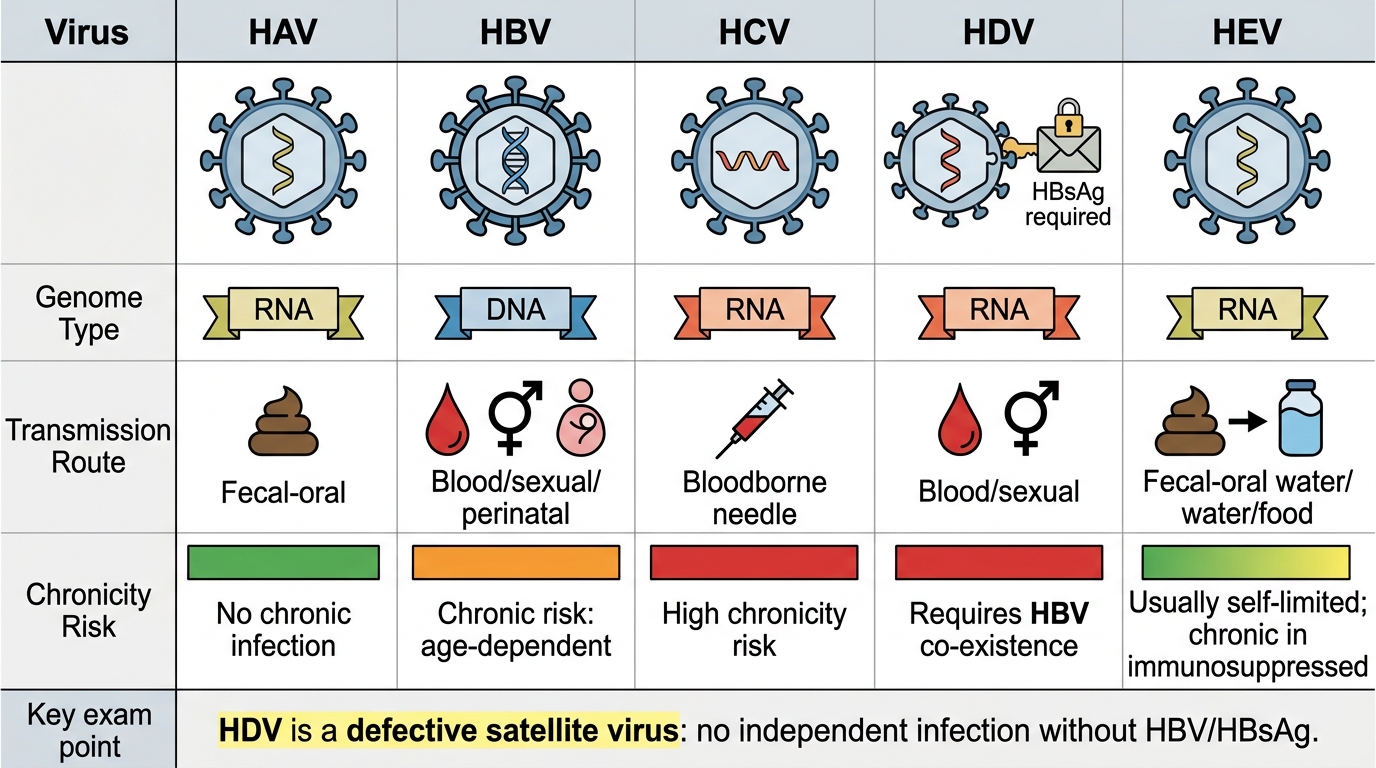
Five viruses preferentially infect hepatocytes and are together called the hepatotropic viruses: HAV (Hepatitis A), HBV (Hepatitis B), HCV (Hepatitis C), HDV (Hepatitis D), and HEV (Hepatitis E). They differ fundamentally in genome, transmission, and fate.
| Feature | HAV | HBV | HCV | HDV | HEV |
|---|---|---|---|---|---|
| Genome | ssRNA (+) | dsDNA (partially) | ssRNA (+) | ssRNA (−), circular | ssRNA (+) |
| Transmission | Faeco-oral | Parenteral/sexual/perinatal | Parenteral (blood) | Parenteral (needs HBV) | Faeco-oral |
| Incubation | 15–45 d | 45–160 d | 14–180 d | 30–60 d | 15–60 d |
| Chronic potential | None | Yes (~5–10% adults) | Yes (~85%) | Co-infection rare; super-infection ~70% | None (except pregnancy) |
| Carrier state | No | Yes | Yes | Yes | No |
| Special risk | None | Perinatal infection → >90% chronic | Highest chronicity | Needs HBsAg to replicate | Fulminant in pregnancy |
IMPORTANT EXAM SHORTCUT: A and E = fAEcal-oral, never chronic. B, C, D = blood/body fluids, can be chronic. D = Defective (needs B).
Hepatitis A-E: Genome, Transmission, and Chronicity
SELF-CHECK
A 30-year-old healthcare worker has an accidental needlestick from an HBsAg-positive patient. He is confirmed non-immune to HBV. Which hepatitis virus CANNOT establish independent chronic infection in this worker even if transmitted via the same needle?
A. Hepatitis B virus
B. Hepatitis C virus
C. Hepatitis D virus
D. Hepatitis E virus
Reveal Answer
Answer: C. Hepatitis D virus
HDV (Hepatitis D) is a defective satellite virus — it cannot replicate or cause infection without the HBsAg envelope provided by HBV. The healthcare worker cannot have independent HDV infection; he would need concurrent or prior HBV infection. HCV (C) can cause independent chronic infection. HEV (E) is typically self-limited but is faeco-oral, not blood-borne. The correct answer is HDV (option C, index 2).
Pathogenesis of Hepatocyte Injury — Focus on HBV
HBV Pathogenesis: CTL-Mediated Hepatocyte Injury and Clinical Outcomes
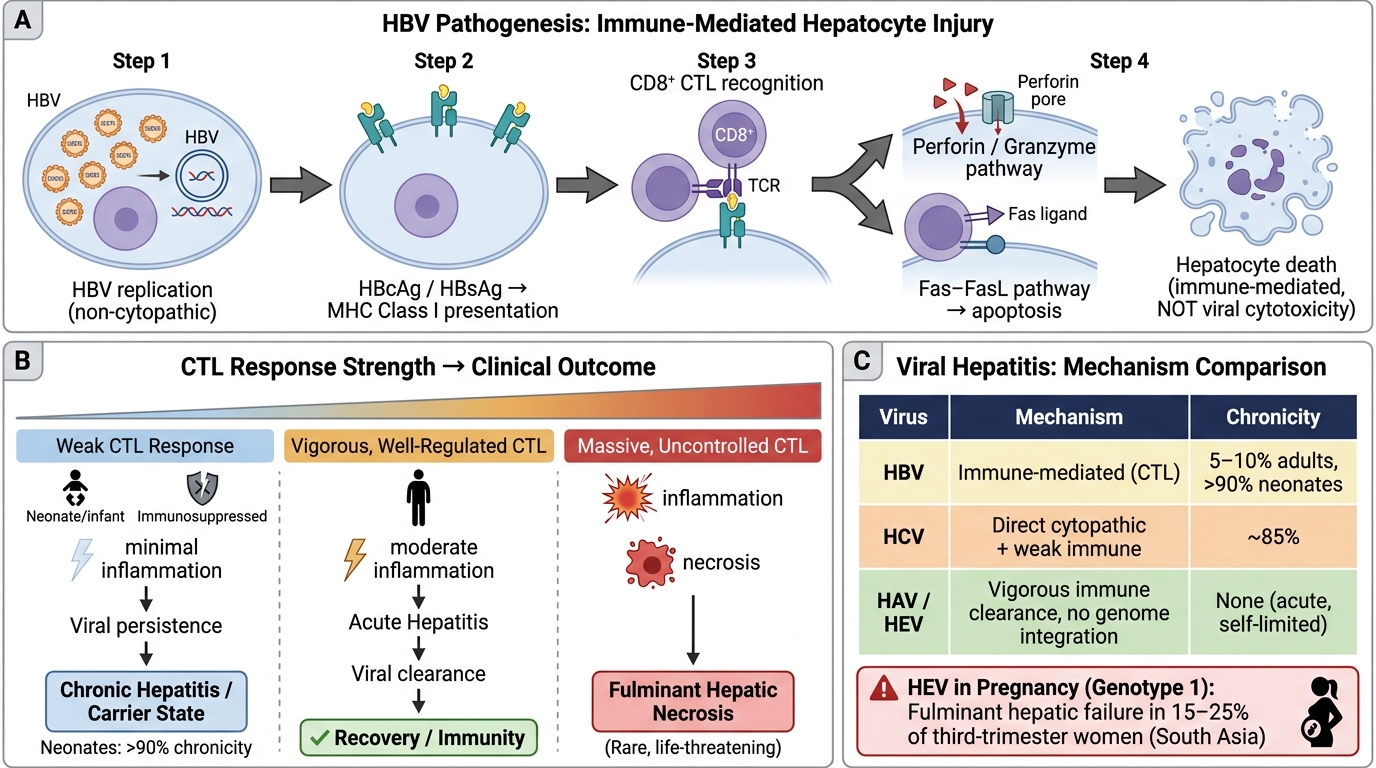
HBV is not directly cytopathic. The virus replicates inside hepatocytes but does not kill them directly. Injury is immune-mediated:
1. HBV infects hepatocytes → viral antigens (HBcAg, HBsAg) are processed and presented on MHC class I molecules.
2. CD8⁺ cytotoxic T lymphocytes (CTLs) recognise HBV-specific peptides on infected cells and kill them via perforin/granzyme and Fas–FasL pathways.
3. The strength and adequacy of this CTL response determines the outcome:
- Vigorous, well-regulated CTL → acute hepatitis → viral clearance → recovery.
- Weak CTL (neonates, immunocompromised) → minimal inflammation → viral persistence → chronic hepatitis or carrier state.
- Massive, uncontrolled CTL response → fulminant hepatic necrosis (rare, life-threatening).
This explains why neonates infected perinatally have >90% chance of becoming chronic carriers — their immature immune system mounts a weak response, the virus is 'tolerated', but the liver pays the long-term price.
HCV uses a different mechanism: direct cytopathic effect plus weak immune response, explaining its very high chronicity (~85%).
HAV and HEV both cause acute, self-limited illness — vigorous immune clearance, no integration into host genome.
CLINICAL PEARL
Why is HEV so dangerous in pregnancy? HEV genotype 1 (South Asia) causes fulminant hepatic failure in 15–25% of pregnant women in their third trimester — a mortality far higher than in non-pregnant adults (~1%). The exact mechanism is debated but involves hormonal immune modulation, increased viral replication, and reduced liver reserve in late pregnancy. Always ask about travel history and gestation when you see a young woman with acute hepatitis and encephalopathy.
Morphology of Acute Hepatitis
Morphology of Acute Hepatitis
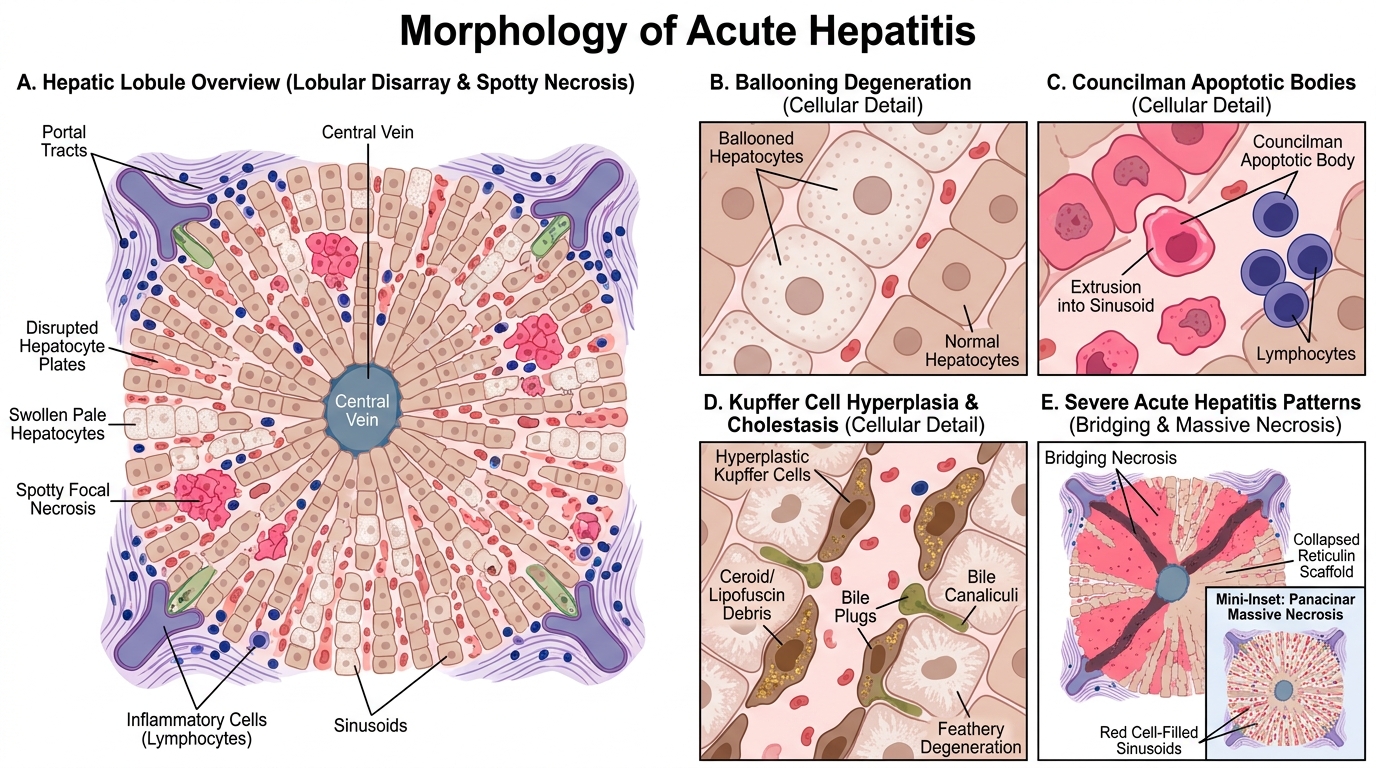
Whether the cause is HAV, HBV, HCV, or a drug, the morphology of acute hepatitis shares common features. Learn these as a set:
Hepatocyte changes (cellular level):
• Ballooning degeneration — hepatocytes swell due to impaired ion transport; cytoplasm becomes pale, rarefied, and granular. The most common change in acute hepatitis.
• Councilman bodies (now also called apoptotic bodies) — shrunken, eosinophilic, rounded hepatocytes that have undergone apoptosis. Key histological hallmark. May be extruded into sinusoids.
• Acidophilic change — diffuse cytoplasmic condensation; precedes frank apoptosis.
Lobular architecture changes:
• Spotty (focal) necrosis — individual hepatocyte death scattered across lobules; associated with lymphocytic infiltrate.
• Lobular disarray — loss of the neat cord-and-sinusoid arrangement due to swelling and dropout of hepatocytes.
• Kupffer cell hyperplasia — resident macrophages enlarge and proliferate; contain engulfed lipofuscin and cellular debris (ceroid pigment).
• Cholestasis — bile plugs in canaliculi and feathery degeneration of hepatocytes in the cholestatic variant.
In severe/fulminant cases:
• Bridging necrosis — necrosis linking portal tracts to central veins (portal-central bridges) or portal tract to portal tract.
• Panacinar (massive) necrosis — entire lobules destroyed; red cell-filled sinusoids and collapsed reticulin scaffold persist; liver shrinks dramatically (acute yellow atrophy). This is fulminant hepatic failure territory.
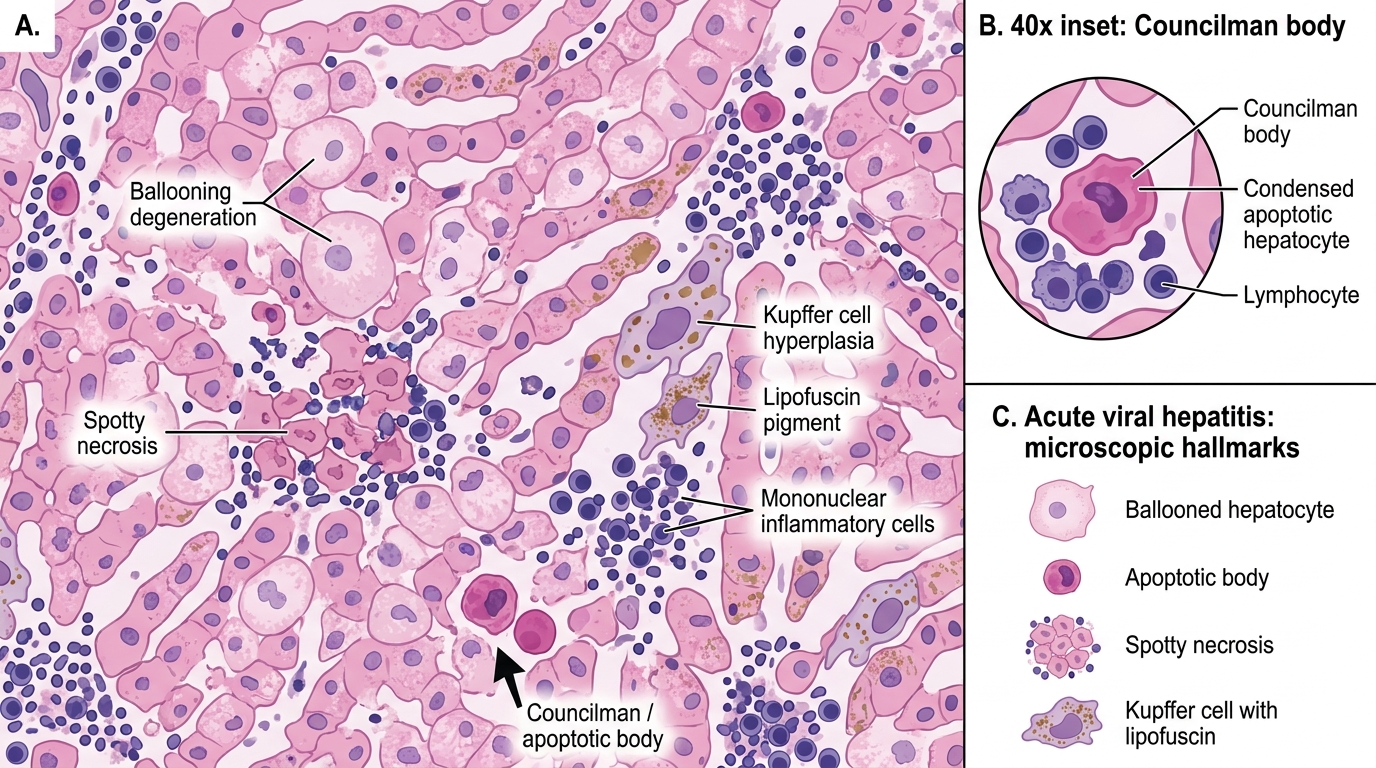
Acute Viral Hepatitis: H&E Microscopic Features
SELF-CHECK
A liver biopsy from a patient with acute hepatitis shows swollen hepatocytes with pale, rarefied cytoplasm alongside shrunken eosinophilic rounded cells extruded into sinusoids. What are the shrunken eosinophilic cells called, and what cell death process do they represent?
A. Ballooning bodies — oncotic necrosis
B. Councilman bodies — apoptosis
C. Mallory–Denk bodies — hepatocyte swelling
D. Ground-glass hepatocytes — viral antigen accumulation
Reveal Answer
Answer: B. Councilman bodies — apoptosis
The shrunken, eosinophilic rounded cells extruded into sinusoids are Councilman bodies (also called apoptotic bodies). They represent individual hepatocyte apoptosis — programmed cell death with cell shrinkage, dense eosinophilic cytoplasm, and nuclear condensation/fragmentation. Ballooning degeneration (A) is the swollen form (oncotic). Mallory–Denk bodies (C) are intracytoplasmic keratin aggregates seen in alcoholic/steatohepatitis. Ground-glass hepatocytes (D) reflect HBsAg accumulation in chronic HBV — a chronic hepatitis finding, not acute.