Page 8 of 32
PA24.3 | Viral & Toxic Hepatitis — SDL Guide (Part 3)
Distinguishing Viral vs Toxic vs Autoimmune Hepatitis
Differentiating Viral, Toxic, and Autoimmune Hepatitis
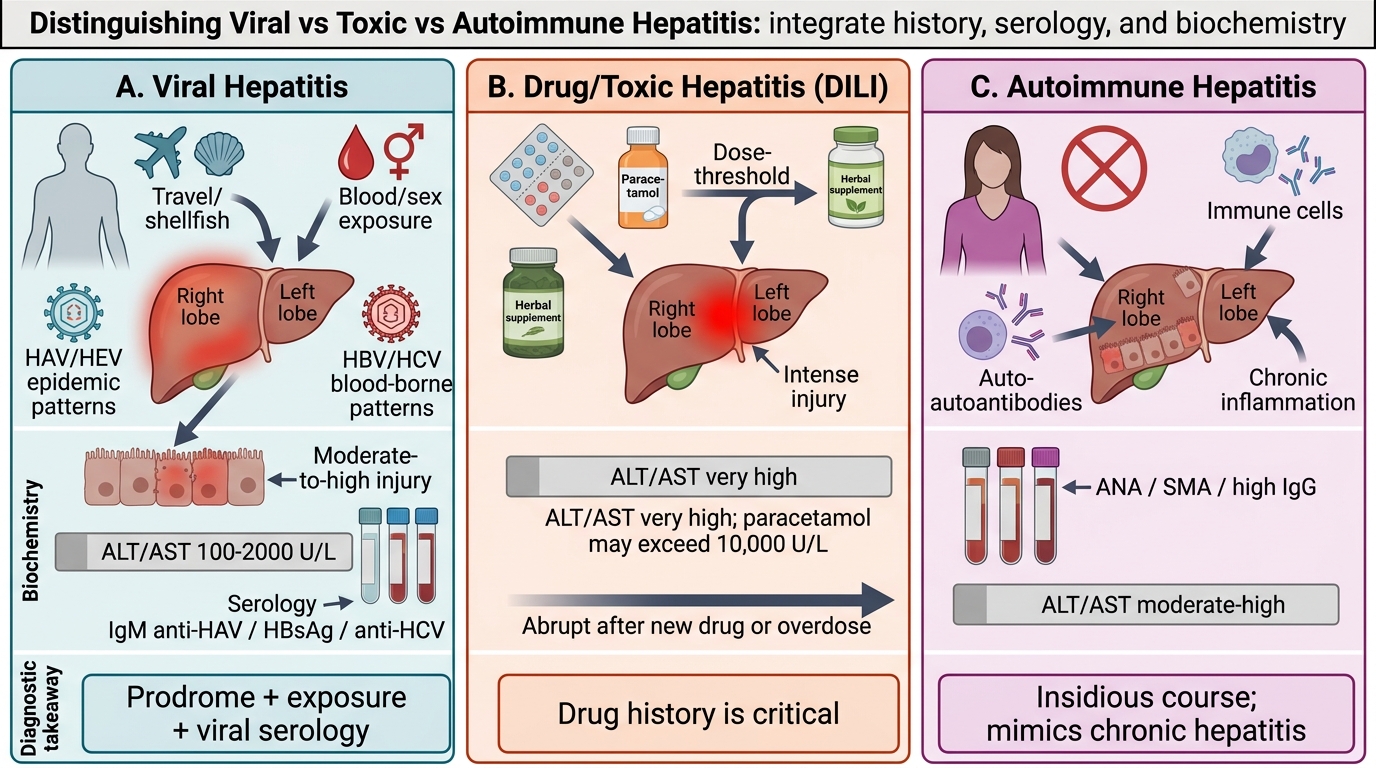
At the bedside and in the lab, differentiating the causes of hepatitis requires integrating history, serology, and biochemistry into a framework:
| Feature | Viral Hepatitis | Drug/Toxic DILI | Autoimmune Hepatitis |
|---|---|---|---|
| Onset | Acute prodrome; chronic insidious | Often abrupt after dose threshold or new drug | Insidious; may mimic chronic hepatitis |
| Age/sex | Any; HAV/HEV epidemic pattern | Any | Young/middle-aged women (type 1) |
| Exposure history | Travel, shellfish (HAV/HEV); sexual/blood exposure (B/C) | Drug history CRITICAL (incl. OTC, herbal) | No clear exposure |
| Transaminases | Moderate–high (100–2000 U/L) | Very high in paracetamol (can exceed 10,000 U/L); variable in idiosyncratic | Moderate–high |
| ALP/GGT | Mildly elevated | Elevated (cholestatic DILI) or mildly elevated (hepatocellular) | Mildly elevated |
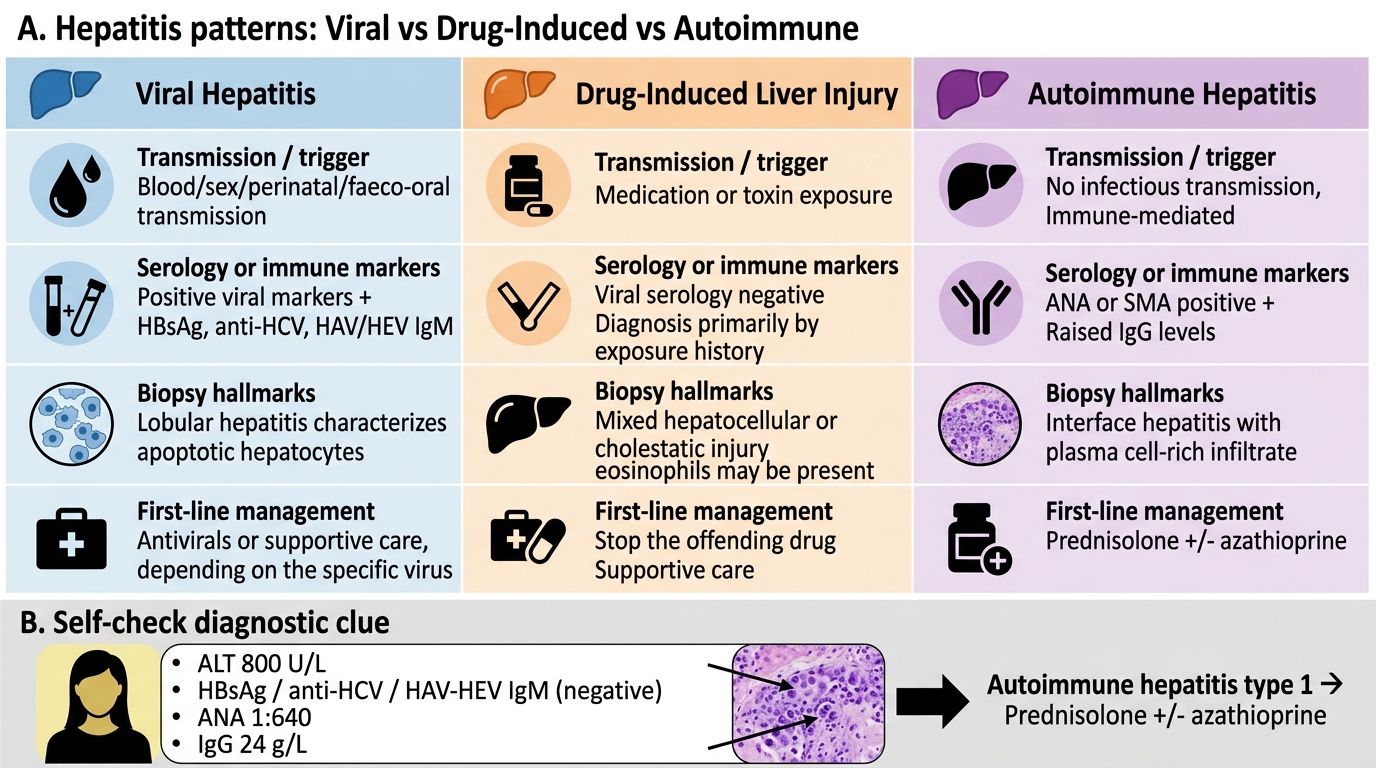
| Serology | HBsAg, anti-HAV IgM, anti-HCV, HCV RNA, anti-HDV, anti-HEV IgM | All viral serologies NEGATIVE | ANA, anti-SMA (anti-smooth muscle Ab), anti-LKM1; IgG elevated |
| Eosinophilia | Absent | Present in immune idiosyncratic DILI (allergic) | Absent |
| Biopsy | Viral cytopathic changes; ground-glass (HBV) | Centrilobular necrosis (paracetamol); eosinophils (idiosyncratic) | Plasma cell infiltrate; rosette formation; interface hepatitis |
| Resolution | Spontaneous (A, E); antiviral therapy (B, C) | Drug withdrawal ± NAC | Steroids + azathioprine |
Key differentiating clues in practice:
- Paracetamol overdose: AST/ALT can exceed 10,000 U/L (a massive spike not seen in viral hepatitis). Ask about tablets taken.
- HAV/HEV: cluster/outbreak pattern; faeco-oral history; no HBsAg/HCV.
- Autoimmune hepatitis: female, associated autoimmunity, responds to steroids, relapses on withdrawal.
- Drug reaction: temporal relationship to starting/stopping drug; eosinophilia; rash.
Distinguishing Viral, Drug-Induced, and Autoimmune Hepatitis
SELF-CHECK
A 28-year-old woman has jaundice, markedly elevated ALT (800 U/L), and fatigue for 3 months. She has no significant drug exposure and denies risk factors for viral hepatitis. Serology shows negative HBsAg, negative anti-HCV, negative anti-HAV/HEV IgM. ANA titre is 1:640, IgG is 24 g/L (raised). Liver biopsy shows interface hepatitis with a plasma cell-rich infiltrate. What is the most likely diagnosis and first-line treatment?
A. Chronic hepatitis B — treat with tenofovir
B. Autoimmune hepatitis — treat with prednisolone ± azathioprine
C. Drug-induced liver injury — withdraw the offending agent
D. Primary biliary cholangitis — treat with ursodeoxycholic acid
Reveal Answer
Answer: B. Autoimmune hepatitis — treat with prednisolone ± azathioprine
The combination of young woman, negative viral serology, elevated IgG, positive ANA (1:640), and plasma cell-rich interface hepatitis on biopsy is the classic presentation of autoimmune hepatitis (AIH) type 1. First-line treatment is immunosuppression: prednisolone (to induce remission) plus azathioprine (to maintain remission and allow steroid tapering). Note: AIH can mimic every form of hepatitis — the critical diagnostic steps are ruling out viral causes and checking autoantibodies + IgG in any unexplained hepatitis.
Fulminant Hepatic Failure — The Critical Complication
Fulminant Hepatic Failure: Massive Necrosis and Clinical Cascade
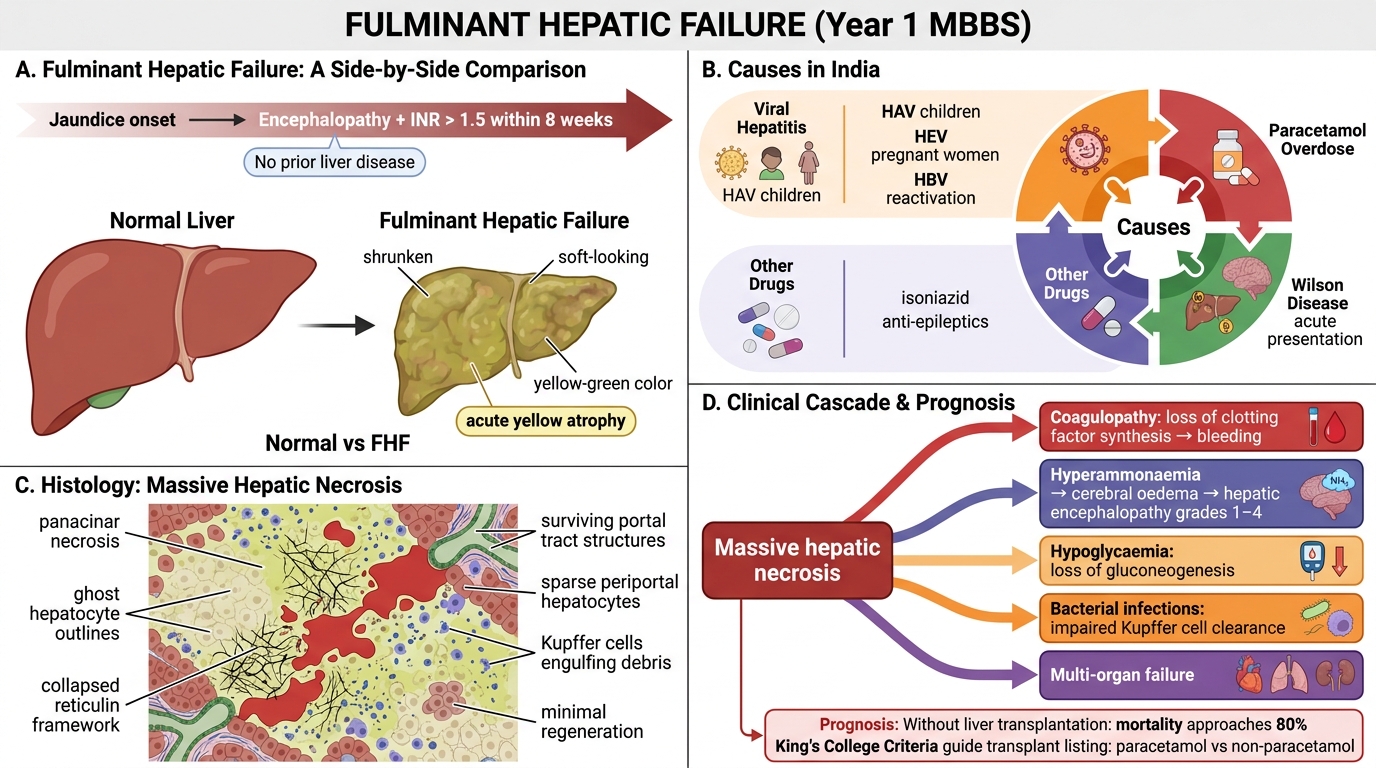
Fulminant hepatic failure (FHF) — also called acute liver failure — is defined as hepatic encephalopathy and coagulopathy (INR >1.5) developing within 8 weeks of onset of jaundice in the absence of prior liver disease.
Causes in India:
1. Viral hepatitis — HAV (in children), HEV (in pregnant women), HBV reactivation
2. Paracetamol overdose
3. Other drugs (isoniazid, anti-epileptics)
4. Wilson disease (acute presentation)
Morphology — massive hepatic necrosis:
- Macroscopically: liver shrunken, soft, yellow-green ('acute yellow atrophy')
- Microscopically: panacinar necrosis — hepatocytes ghost outlines, collapsed reticulin framework, haemorrhagic sinusoids; only portal tract structures and sparse periportal hepatocytes may survive
- Kupffer cells engulf debris; minimal regenerative activity (too rapid)
Clinical cascade:
- Coagulopathy (loss of clotting factor synthesis) → bleeding
- Hyperammonaemia → cerebral oedema → hepatic encephalopathy (grades 1–4)
- Hypoglycaemia (loss of gluconeogenesis)
- Bacterial infections (loss of Kupffer cell-mediated clearance)
- Multi-organ failure
Prognosis: Without liver transplantation, mortality approaches 80%. The King's College Criteria (paracetamol vs non-paracetamol categories) guide transplant listing.