Page 11 of 21
PA28.{2,6} | Penile Carcinoma & Male Genital Morphology — SDL Guide
Learning Objectives
- Describe the pathogenesis, risk factors, and HPV-related pathways in penile carcinoma (PA28.2)
- Distinguish the premalignant lesions of the penis — Bowen disease, erythroplasia of Queyrat, and bowenoid papulosis — by site, HPV type, and malignant potential (PA28.2)
- Describe the gross types (papillary vs flat/ulcerative) and microscopic features of invasive penile squamous cell carcinoma, including spread and staging (PA28.2)
- Identify on gross and microscopic images: seminoma, mixed/non-seminomatous germ cell tumor, nodular hyperplasia of prostate, prostatic adenocarcinoma (Gleason grading), condyloma acuminatum, and penile SCC — as required for the morphology practical (PA28.6)
- Apply the Gleason grading system to describe prostatic adenocarcinoma patterns and understand the Gleason score (PA28.6)
- Explain the distinguishing histological features that allow pattern recognition in the male genital tract for exam-based image identification (PA28.6)
INSTRUCTIONS
This is the morphology consolidation SDL for the Male Genital Tract cluster. It is written primarily for the practical examination — you must be able to look at a gross specimen or a microscopic slide and NAME the disease. Read each block, study the image markers carefully, and ask yourself: 'If I see this in the practical, what do I say?' The micro_quiz questions are typical spotting-type viva questions. Complete SDL1 (Testicular Tumors) and SDL2 (Prostate Pathology) before this session.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 21 (textbook)
- Harsh Mohan Textbook of Pathology, 7th ed., Ch. 24 (textbook)
- WHO Classification of Tumours of the Urinary System and Male Genital Organs, 5th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man from rural Rajasthan presents with a 3-month history of a painless, slowly enlarging ulcer on the glans of his penis. He has never been circumcised. He mentions he had difficulty retracting his foreskin for years. On examination, there is a 2 cm indurated, crater-like ulcer with raised, everted margins on the glans and adjacent prepuce, with firm, non-tender left inguinal lymph nodes. His wife asks: 'Doctor, is this cancer? Is it because of something he did?' — How will you answer her? And before you answer a single clinical question, you need to know exactly what this lesion looks like under the microscope, what predisposed him, and how it spreads. That is what this SDL teaches.
WHY THIS MATTERS
Penile carcinoma and male genital tract morphology appear in the Year-2 Pathology practical exam in two formats: (1) Spot diagnosis — you are shown a gross specimen or histology slide and asked to name the disease; (2) Short questions about pathogenesis and distinguishing features. PA28.2 and PA28.6 together cover the entire male genital tract. This SDL is your morphology consolidation: penile pathology in depth, followed by a systematic review of what to look for in testicular tumors, prostate lesions, and penile lesions — all framed as practical exam recognition. This is the most image-dense SDL in the cluster intentionally. Think of each image marker as a flashcard you will see in the practical hall.
RECALL
Before reading further, recall from SDL1 and SDL2:
- Testicular tumors — seminoma vs non-seminomatous germ cell tumor (NSGCT); tumor markers AFP, β-hCG, LDH; the concept of ITGCN (intratubular germ cell neoplasia unclassified) as the in-situ precursor.
- Prostate — the anatomical zones (peripheral, central, transition); BPH arises in the transition zone; prostatic adenocarcinoma arises predominantly in the peripheral zone; PSA as serum marker.
- HPV biology — HPV is a double-stranded DNA virus; low-risk types (6, 11) → condylomas (warts); high-risk types (16, 18) → dysplasia and carcinoma via E6 (inactivates p53) and E7 (inactivates Rb).
If any of these are hazy, re-read the relevant SDL before continuing.
Penile Anatomy and the Staging Context
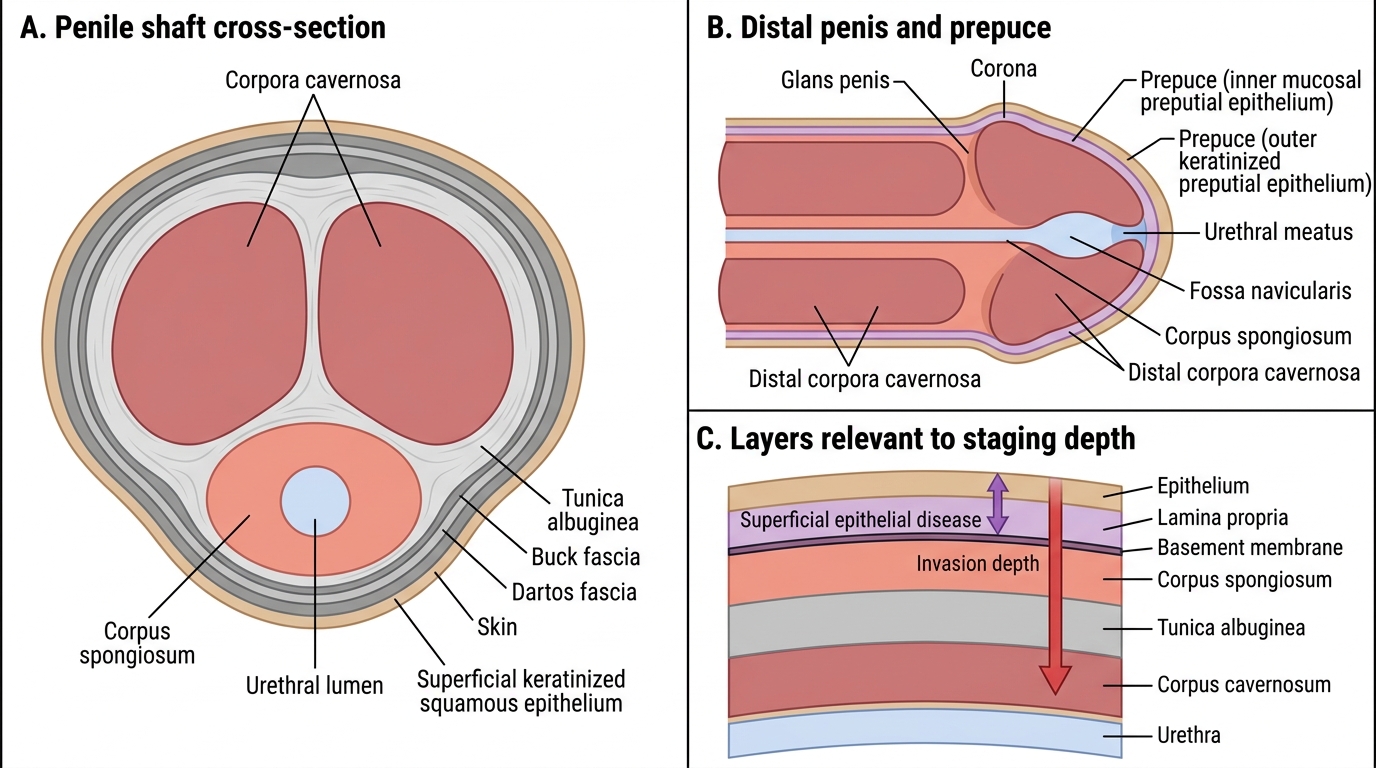
Understanding penile pathology requires a brief anatomical framework. The penis is composed of two corpora cavernosa (paired, dorsal, erectile) and one corpus spongiosum (ventral, surrounding the urethra). The distal expansion of the corpus spongiosum forms the glans penis, covered by the prepuce (foreskin).
The epithelium covering the glans and inner prepuce is non-keratinized stratified squamous epithelium — identical in character to mucosal surfaces. The outer skin of the penile shaft is keratinized squamous epithelium.
Why anatomy matters for staging: TNM staging of penile carcinoma is largely determined by depth of invasion:
- T1a: lamina propria only, no lymphovascular invasion (LVI), grade 1–2
- T1b: lamina propria with LVI, or grade 3
- T2: corpus spongiosum or cavernosum
- T3: urethra
- T4: adjacent structures (scrotum, prostate)
Lymphatic spread follows the inguinal nodes (superficial → deep inguinal → pelvic). Inguinal node status is the single most important prognostic factor.
Penile Anatomy and Staging Depth Zones
Condyloma Acuminatum — HPV 6/11 (Benign)
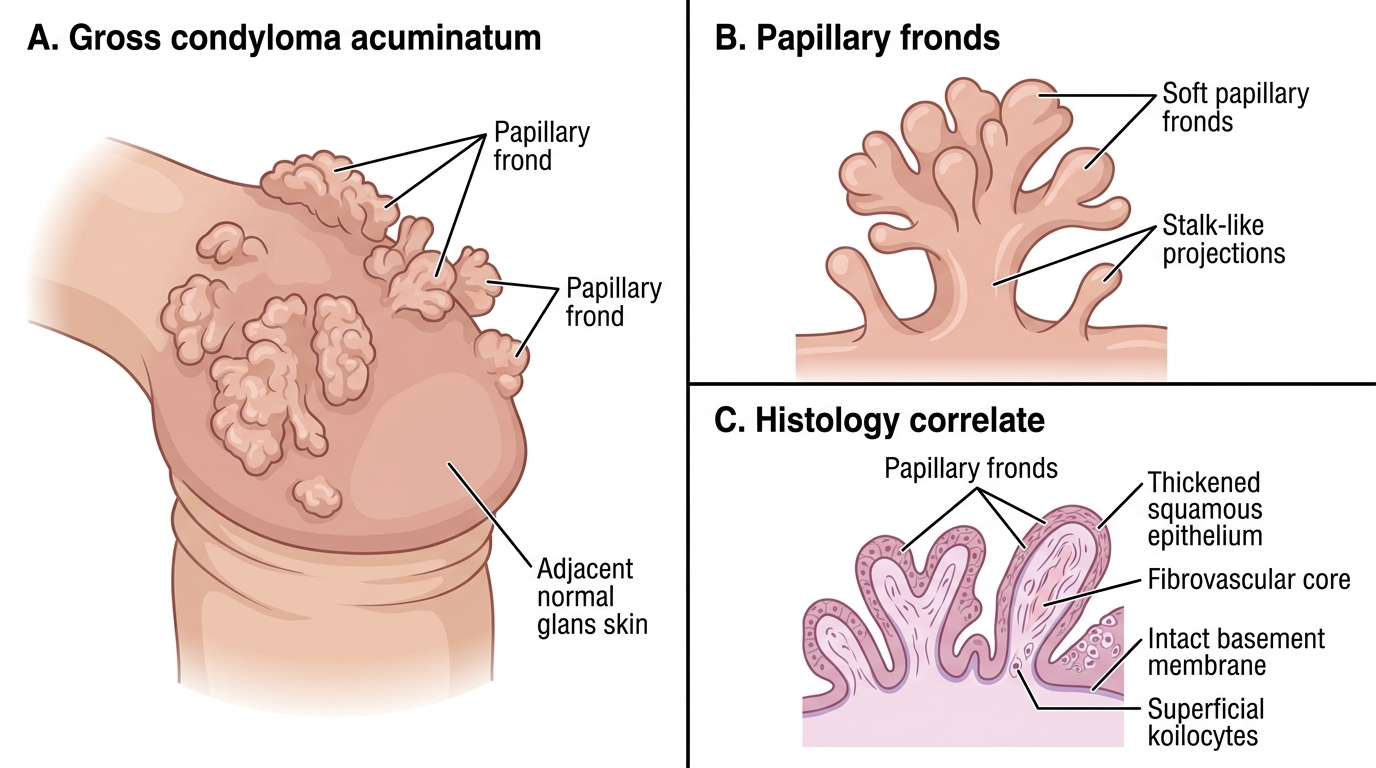
Condyloma acuminatum (plural: condylomata acuminata) — commonly called genital warts — is caused by HPV types 6 and 11 (low-risk types). It is the most common STI-related penile lesion.
Gross appearance: Soft, moist, papillary or cauliflower-like excrescences (projections) on the glans, prepuce, or penile shaft. May be single or multiple. Color varies from skin-colored to pink-red. They do NOT ulcerate unless secondarily infected.
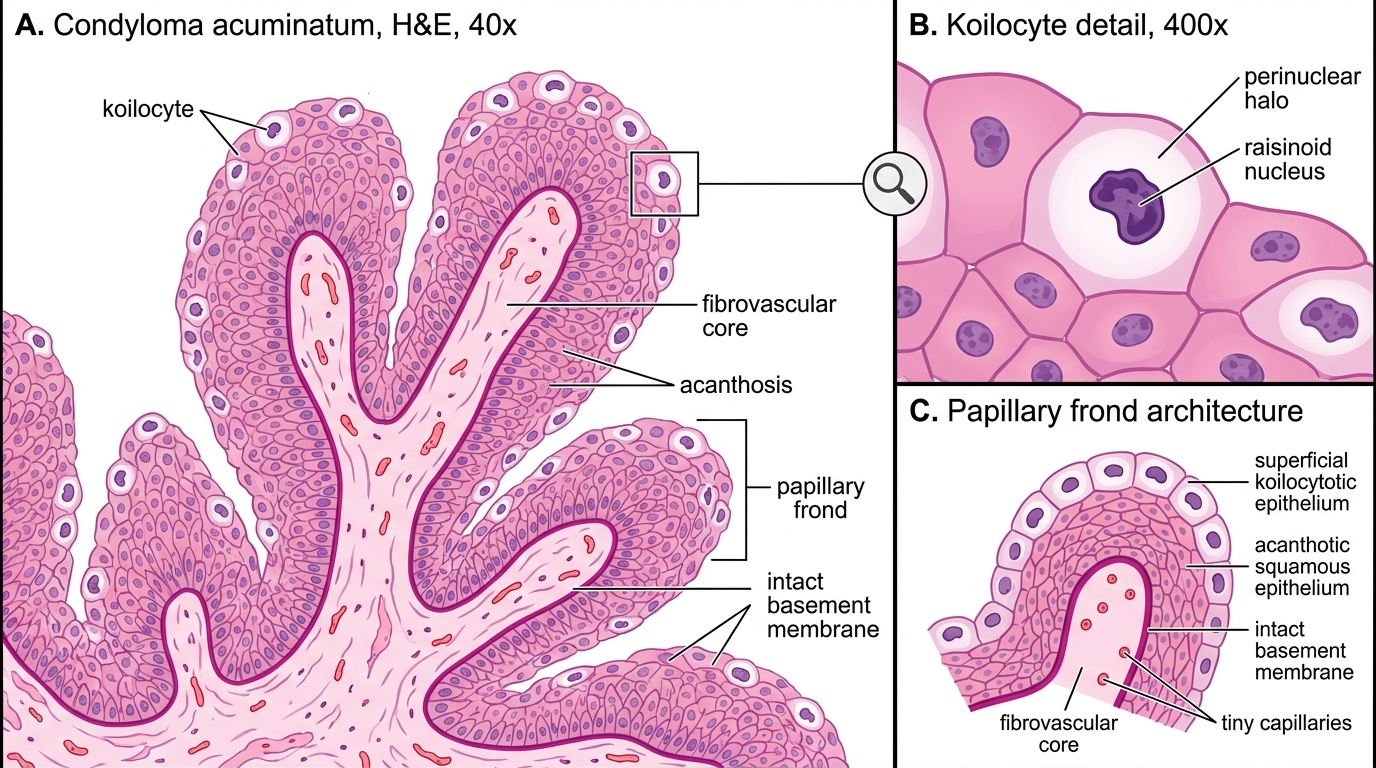
Microscopic features — the hallmark is koilocytosis:
- Koilocytes: squamous cells with perinuclear cytoplasmic halos and dark, wrinkled (raisinoid) nuclei — this is the cytopathic effect of HPV replication
- Papillary architecture with fibrovascular cores (acanthosis + papillomatosis)
- Surface hyperkeratosis (thickened keratin layer) and parakeratosis
- NO dysplasia (no atypia in deeper layers, no abnormal mitoses)
- Basement membrane intact — no invasion
Malignant potential: Negligible for HPV 6/11 condylomas. However, a giant condyloma (Buschke-Löwenstein tumor) is a locally destructive but non-metastasizing variant.
Condyloma Acuminatum: Gross Appearance and Histology Correlate
Condyloma Acuminatum: H&E Histology
Premalignant Penile Lesions — The HPV 16/18 Trio
Three lesions are traditionally grouped as penile intraepithelial neoplasia (PeIN) — all carry high malignant potential, all are linked to HPV 16/18, and all show full-thickness or near-full-thickness squamous dysplasia without invasion. They differ primarily in anatomical location and clinical presentation:
| Feature | Bowen Disease | Erythroplasia of Queyrat | Bowenoid Papulosis |
|---|---|---|---|
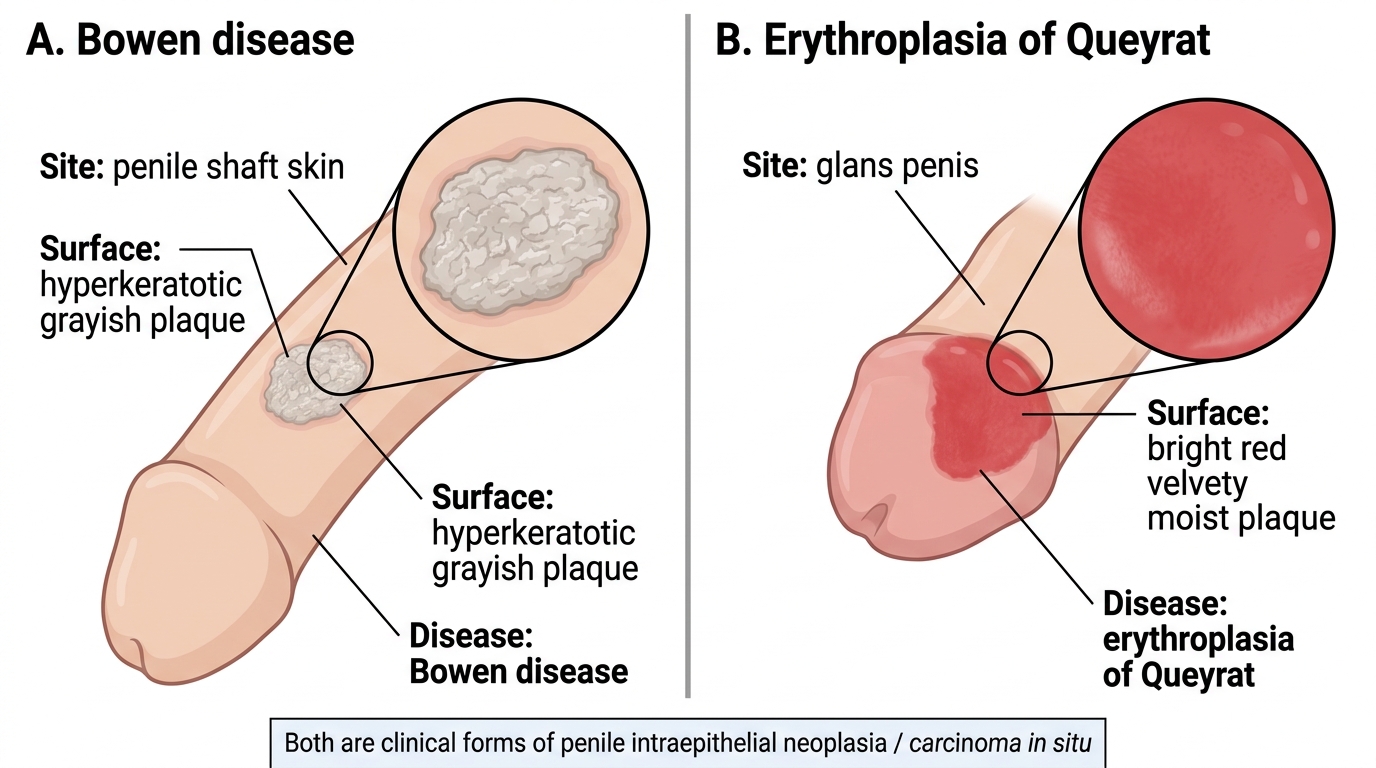
| Location | Penile shaft skin | Glans / inner prepuce | Shaft skin (or glans) |
| Gross | Solitary, thickened, hyperkeratotic, grayish-white plaque | Bright red, velvety, moist plaque | Multiple (1–10 mm) red-brown papules |
| HPV | 16/18 | 16/18 | 16/18 |
| Histology | PeIN — full-thickness dysplasia with hyperkeratosis | PeIN — full-thickness dysplasia, NO hyperkeratosis (mucosa) | PeIN — but often self-limited in young adults |
| Malignant risk | ~10% → invasive SCC | ~10–30% → invasive SCC | LOW in immunocompetent young adults; higher in immunosuppressed |
| Patient age | Older men | Older men | Younger men (often multiple sex partners) |
Key histological feature common to all three: Full-thickness dysplasia — large atypical keratinocytes with hyperchromatism, abnormal mitoses (including tripolar/bizarre forms), loss of normal maturation from base to surface, and dyskeratotic cells. The basement membrane is intact (in-situ lesion).
Exam tip: The most tested distinction is location — Bowen on skin (keratinized, so hyperkeratosis on top), erythroplasia on glans/mucosa (red and moist because no keratin). Histologically identical otherwise.
Gross Comparison of Bowen Disease and Erythroplasia of Queyrat
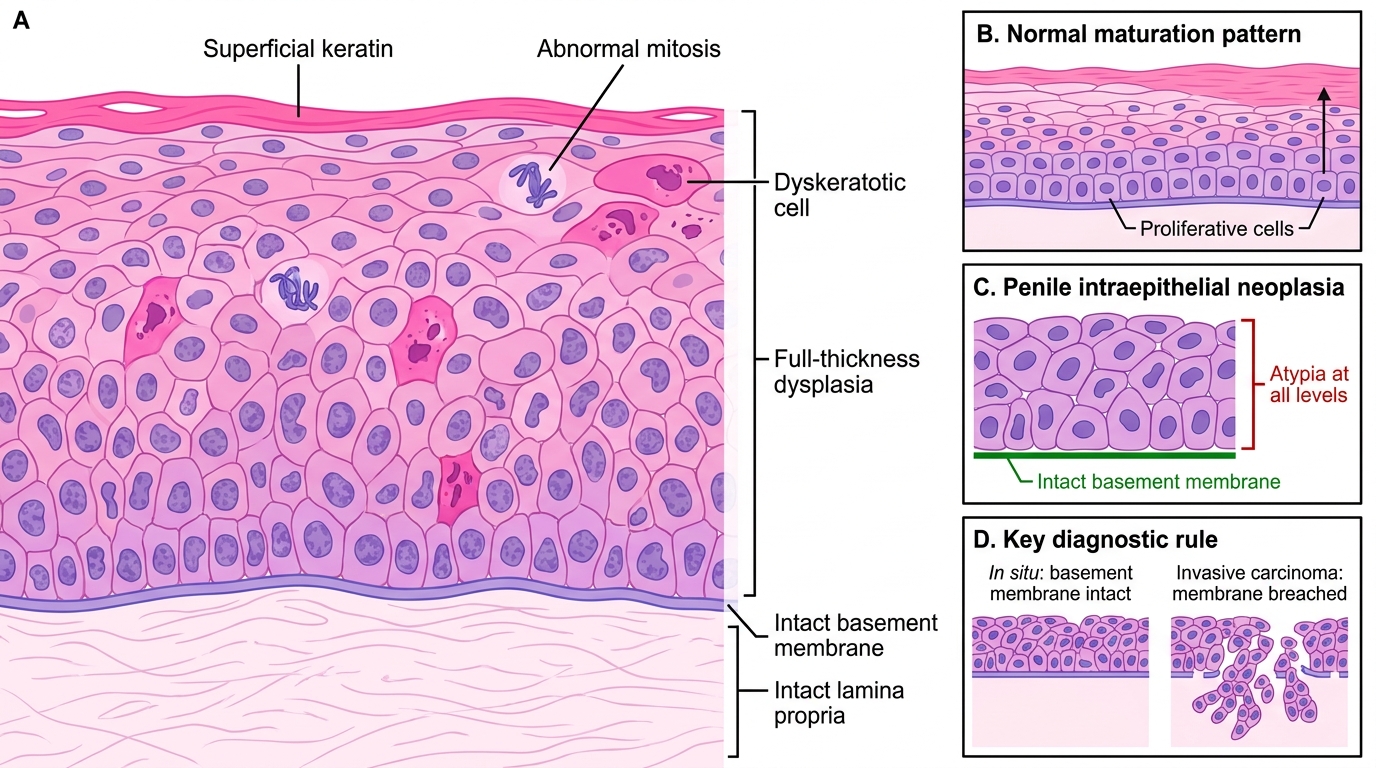
Penile Intraepithelial Neoplasia: Full-Thickness Dysplasia
CLINICAL PEARL
HPV risk stratification in penile lesions — one rule to remember: HPV 6/11 → Condyloma (NO cancer risk). HPV 16/18 → PeIN / SCC (HIGH cancer risk). The same HPV types drive cervical carcinoma. Quadrivalent HPV vaccine (Gardasil) covers 6, 11, 16, 18 — preventing condyloma AND squamous cell carcinoma of both cervix and penis.