Page 12 of 21
PA28.{2,6} | Penile Carcinoma & Male Genital Morphology — SDL Guide (Part 2)
Invasive Squamous Cell Carcinoma of the Penis — Risk Factors & Pathogenesis
Penile squamous cell carcinoma (SCC) is uncommon in developed countries (1% of male cancers) but accounts for up to 10–20% of male cancers in parts of Africa, South America, and Asia. Understanding risk factors is testable and clinically important.
Risk factors and their mechanisms:
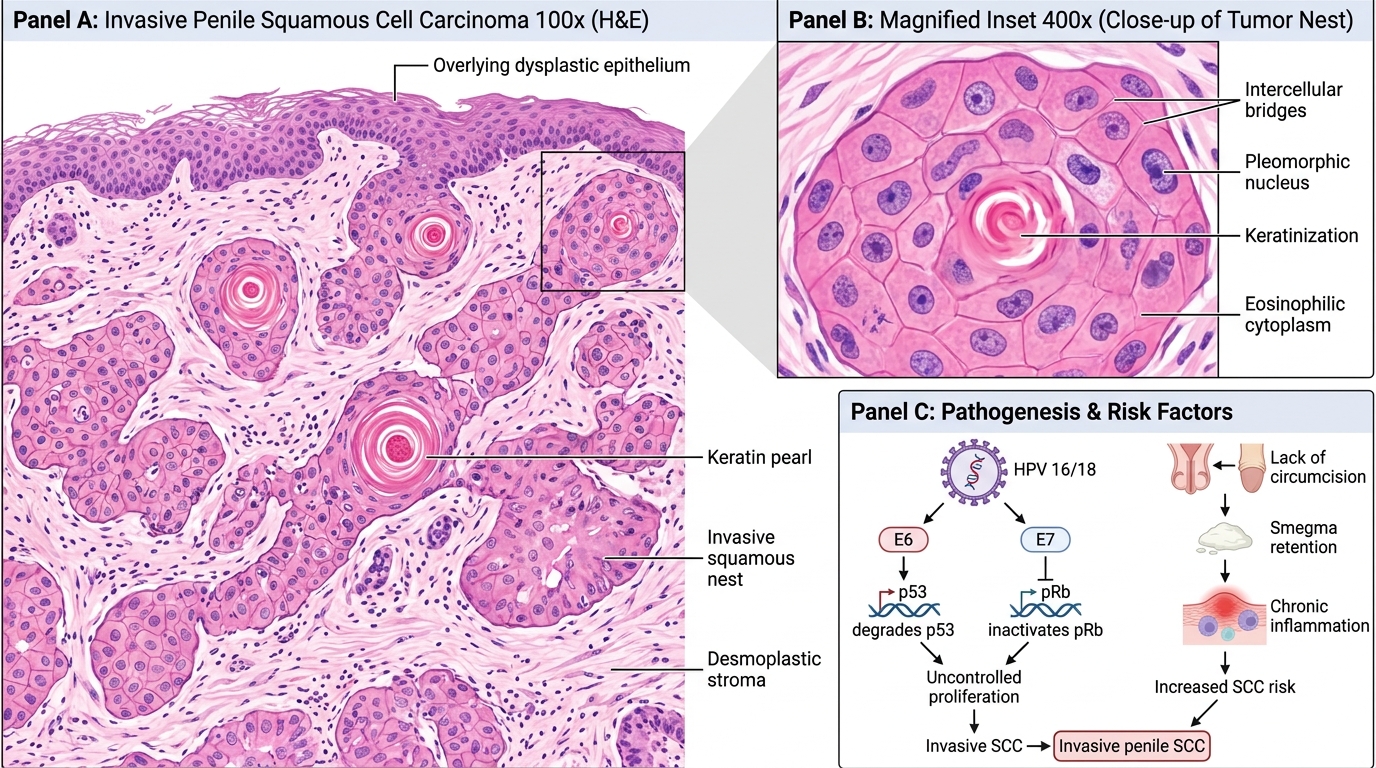
1. HPV infection (types 16, 18) — present in ~40–50% of penile SCCs. HPV E6 protein binds and degrades p53 (guardian of genome); HPV E7 protein inactivates pRb (cell cycle brake). Result: uncontrolled proliferation + blocked apoptosis → SCC.
2. Lack of circumcision — intact foreskin traps smegma (desquamated cells + secretions), causing chronic inflammation. Circumcision at birth reduces risk by ~3–5-fold. (Penile carcinoma is virtually absent in populations with universal neonatal circumcision: Jewish, Muslim communities.)
3. Phimosis — inability to retract the foreskin causes stasis of smegma under the prepuce, chronic inflammation, and occasionally secondary HPV trapping. Present in >50% of penile carcinoma patients.
4. Smoking — tobacco carcinogens excreted in urine and concentrated in preputial space; ~4-fold increased risk.
5. Chronic inflammatory conditions — lichen sclerosus (balanitis xerotica obliterans), lichen planus of the glans.
Two pathogenic pathways:
- HPV-associated pathway (younger patients, ~40%): condyloma → PeIN (basaloid/warty subtype) → basaloid SCC
- HPV-independent pathway (older patients, ~60%): chronic inflammation (lichen sclerosus, phimosis) → differentiated PeIN → keratinizing SCC
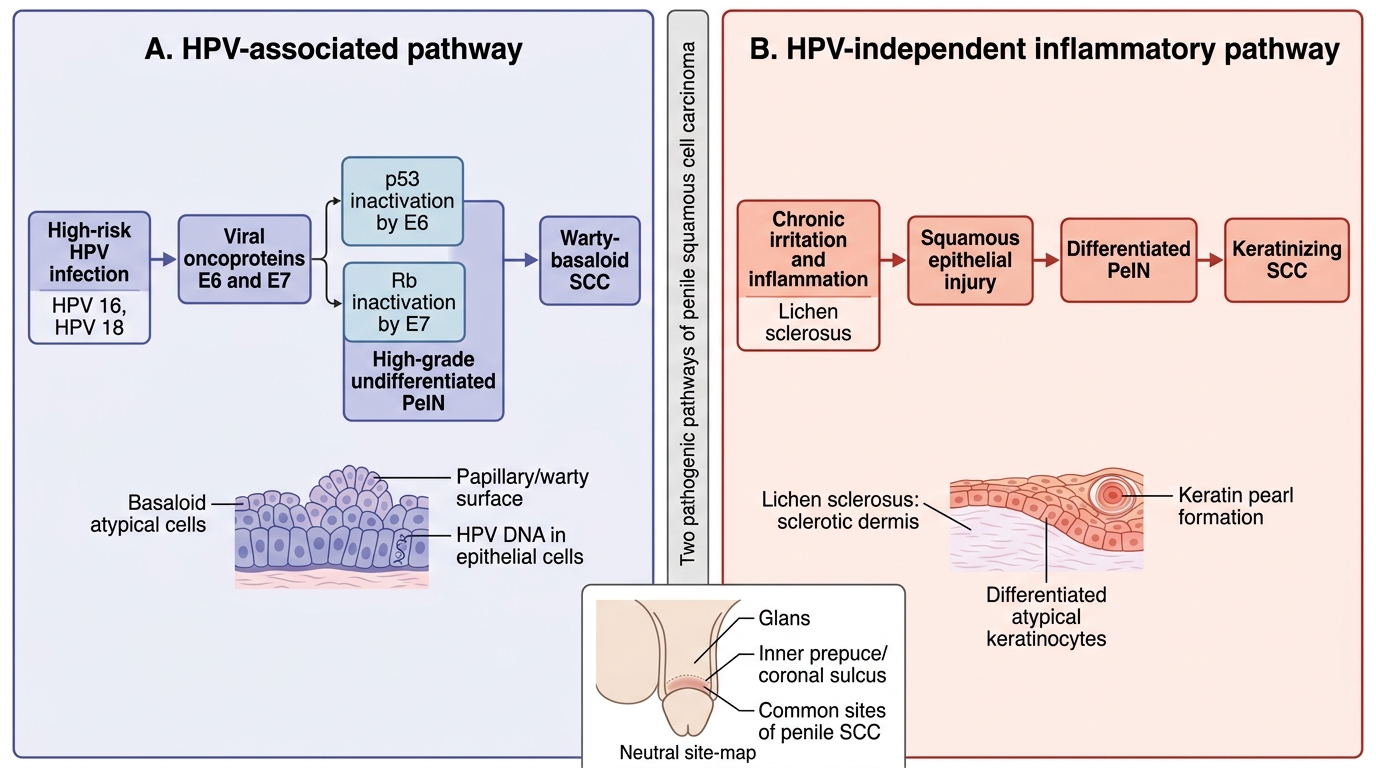
Pathogenic Pathways of Penile Squamous Cell Carcinoma
Gross Morphology of Penile SCC — Papillary vs Flat/Ulcerative
Penile SCC most commonly arises on the glans (~48%) or the inner prepuce/coronal sulcus (~21%), corresponding to the highest HPV exposure and chronic irritation sites.
Two major gross types — exam-critical distinction:
1. Papillary (exophytic) type:
- Irregular, cauliflower-like, or warty papillary mass
- Often gray-white or tan
- May have areas of surface necrosis
- Usually less deeply invasive at presentation
- Corresponds to warty or verrucous histological subtype
2. Flat/ulcerative (endophytic) type:
- Flat, indurated plaque that ulcerates centrally
- Ulcer has raised, rolled/everted margins and a dirty necrotic base
- Surrounding induration from desmoplastic stromal reaction
- Deeper invasion at presentation
- Higher grade, worse prognosis
Cut surface: Firm, gray-white tumor infiltrating the underlying corpus spongiosum or corpora cavernosa; irregular, infiltrating borders.
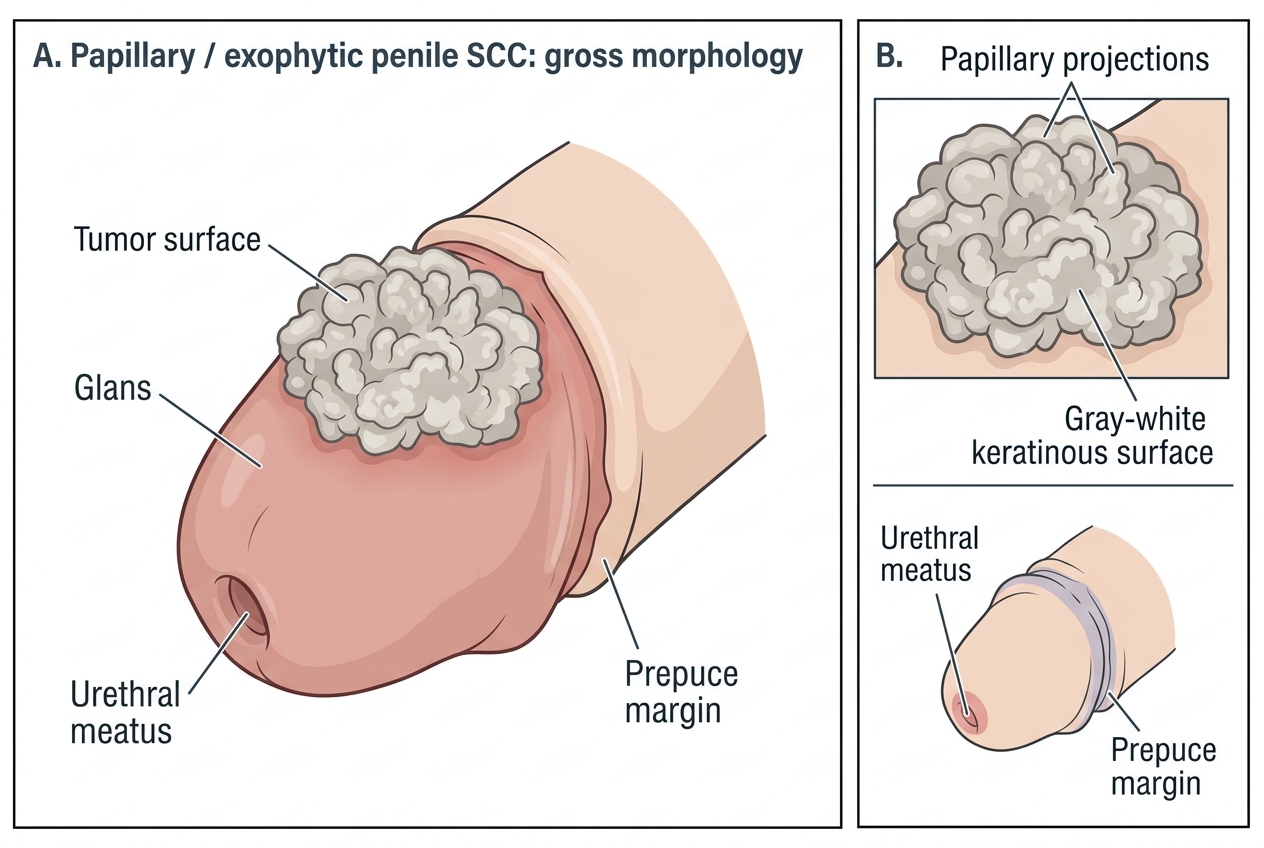
Papillary Exophytic Penile Squamous Cell Carcinoma
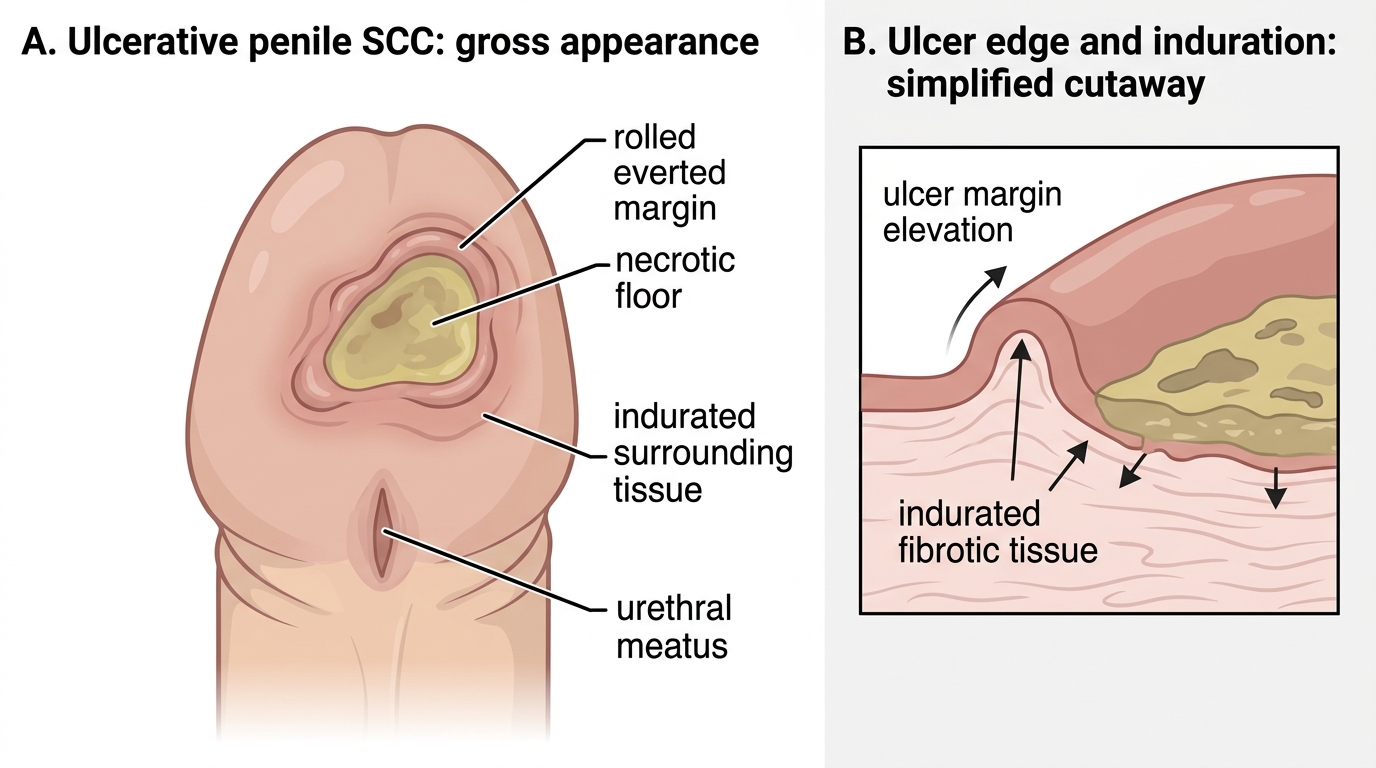
Gross Appearance of Ulcerative Penile SCC
Microscopy of Penile SCC — What to Look For
The majority of penile SCCs are keratinizing (conventional) squamous cell carcinoma. The microscopic features must be committed to memory for practical examination.
Key histological features:
- Irregular nests and cords of malignant squamous cells invading the underlying stroma (dermal or subepithelial connective tissue)
- Keratin pearls (squamous pearls, epithelial pearls) — concentric whorls of squamoid cells with central laminated keratin. A near-pathognomonic feature of well-differentiated (Grade 1) keratinizing SCC.
- Individual cell keratinization — single cells with dense pink cytoplasm and dark nuclei throughout the tumor nests (even in moderately differentiated tumors)
- Intercellular bridges (desmosomes) visible between adjacent tumor cells at high power — confirms squamous lineage
- Stromal desmoplasia — reactive fibrous stroma surrounding tumor nests, dense collagen, inflammatory infiltrate
- Cytological atypia — enlarged, pleomorphic nuclei; prominent nucleoli; abnormal mitoses (tripolar, bizarre forms)
- In poorly differentiated SCC: sheets of anaplastic cells, few or no keratin pearls, more abnormal mitoses
Grading (Grade 1–3):
- Grade 1 (well-differentiated): abundant keratin, good squamous maturation, few mitoses
- Grade 2 (moderately differentiated): moderate keratin, intermediate features
- Grade 3 (poorly differentiated): minimal keratin, marked atypia, many mitoses
Well-Differentiated Penile Squamous Cell Carcinoma
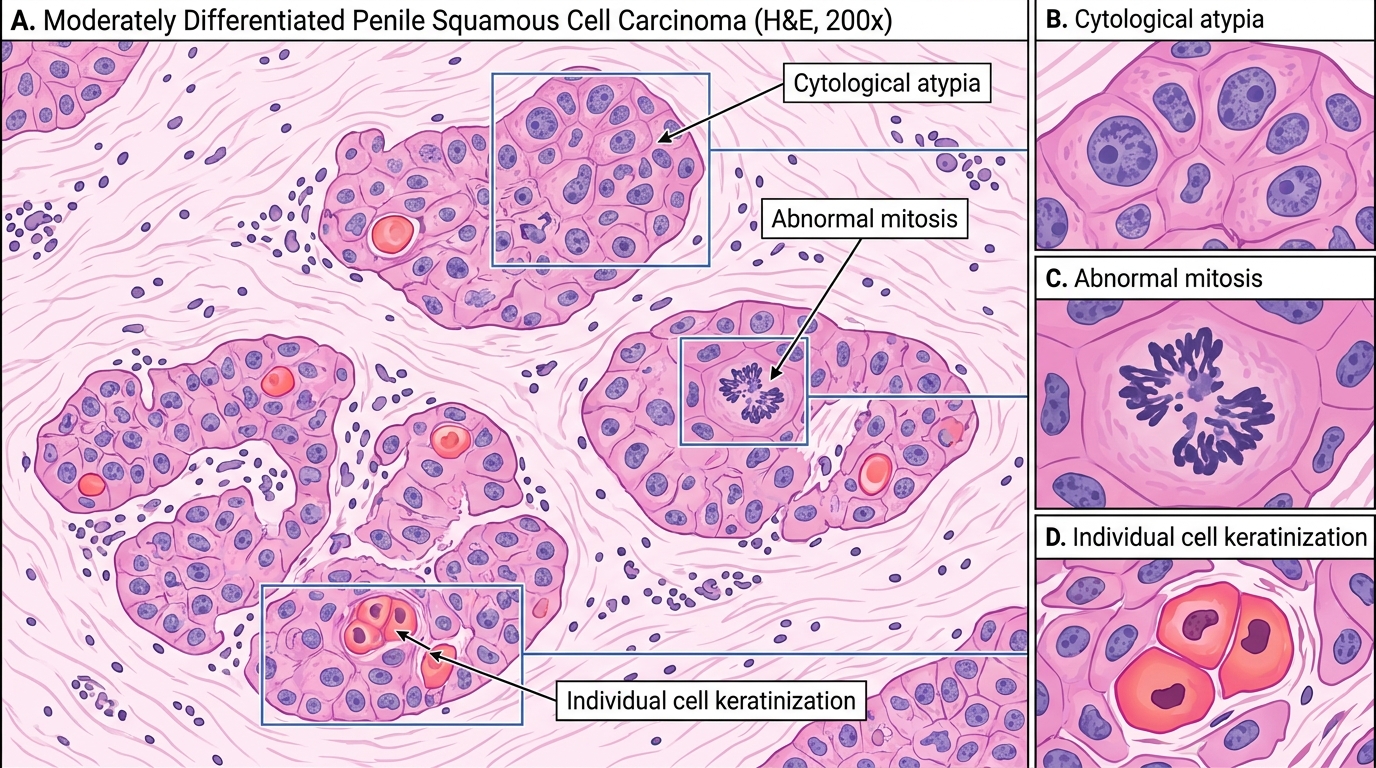
Moderately Differentiated Penile Squamous Cell Carcinoma, H&E 200x