Page 13 of 21
PA28.{2,6} | Penile Carcinoma & Male Genital Morphology — SDL Guide (Part 3)
Spread, Staging, and Prognosis of Penile SCC
Routes of spread:
1. Direct extension — tumor extends along the penile shaft; deep invasion into corpus spongiosum then cavernosum; late extension to scrotum, perineum, or pubic symphysis.
2. Lymphatic spread — the most important route clinically:
- First station: superficial inguinal nodes (palpable in inguinal region)
- Second station: deep inguinal nodes (Cloquet node — the most cephalad deep inguinal node at the femoral ring; its status on FNA/biopsy determines further pelvic dissection)
- Third station: iliac (pelvic) nodes
- Cross-drainage: bilateral spread from midline tumors
3. Haematogenous spread — late; liver, lung, bone.
TNM staging summary (simplified):
| Stage | Features | 5-year OS |
|---|---|---|
| T1a N0 | LP only, low grade, no LVI | ~90% |
| T2 N0 | Into corpus spongiosum/cavernosum | ~70% |
| Any T, N1 | 1 inguinal node metastasis | ~50% |
| Any T, N2-3 | Multiple/bilateral nodes | <30% |
| M1 | Distant metastasis | <10% |
Prognostic factors: Node status > depth > grade. Inguinal lymph node dissection (ILND) improves survival in node-positive patients.
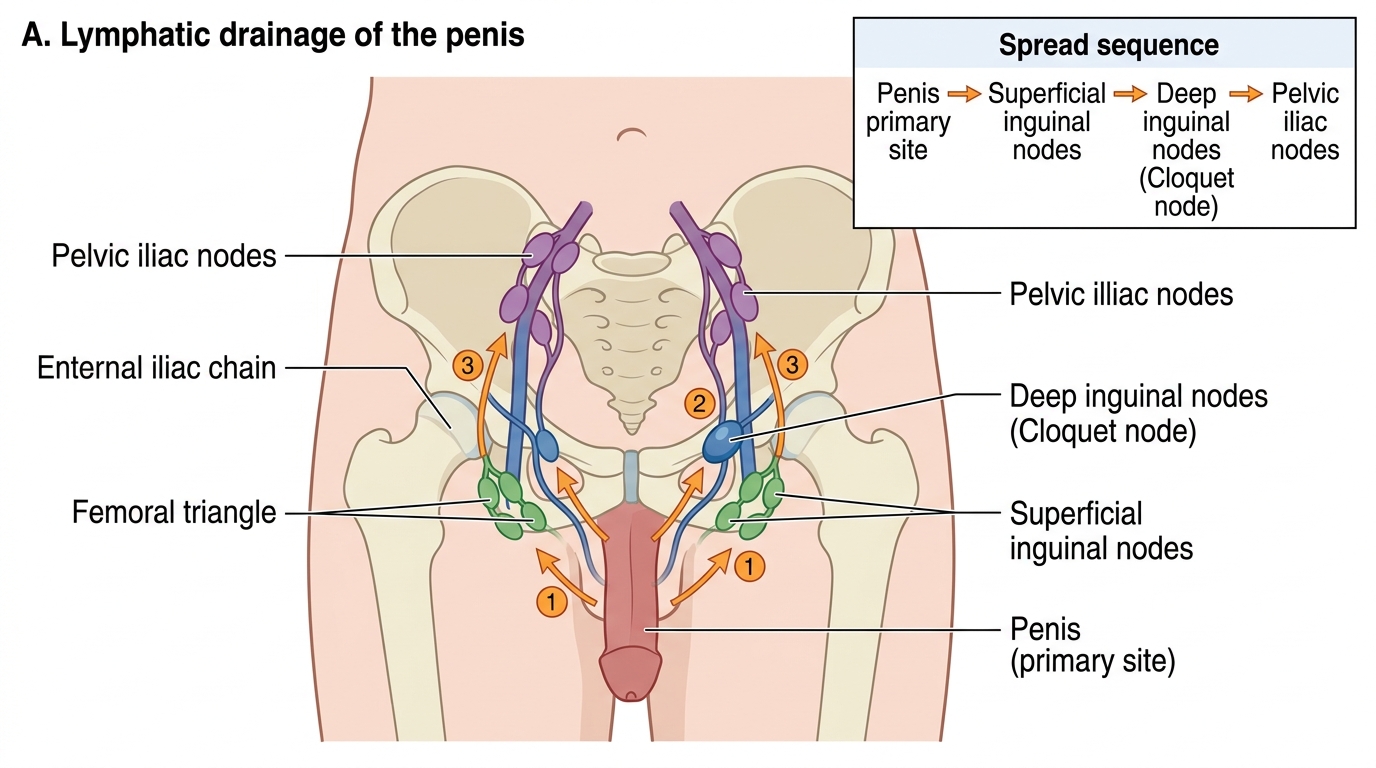
Lymphatic Drainage of the Penis
SELF-CHECK
A 55-year-old uncircumcised man has a 1.5 cm ulcerative lesion on the glans with rolled margins. Biopsy shows irregular nests of squamous cells with keratin pearls invading into the lamina propria, with stromal desmoplasia. HPV 16 is detected by ISH. Which histological feature is most characteristic of well-differentiated SCC?
A. Koilocytes with perinuclear halos
B. Full-thickness epithelial dysplasia with intact basement membrane
C. Concentric whorls of squamoid cells with central laminated keratin (keratin pearls)
D. Fibrovascular cores within papillary fronds
Reveal Answer
Answer: C. Concentric whorls of squamoid cells with central laminated keratin (keratin pearls)
Keratin (squamous/epithelial) pearls — concentric whorls of squamoid cells with central laminated keratin — are the hallmark of well-differentiated keratinizing SCC. Koilocytes are the cytopathic effect of HPV in condyloma (benign). Full-thickness dysplasia with intact basement membrane = PeIN (in-situ, no invasion). Fibrovascular cores in papillary fronds = condyloma acuminatum.
SELF-CHECK
A pathology practical slide shows a bright red, velvety, moist plaque from the glans penis of a 62-year-old. Microscopically there is full-thickness squamous dysplasia with loss of normal maturation, abnormal mitoses, and no surface hyperkeratosis. The basement membrane is intact. What is the diagnosis?
A. Condyloma acuminatum
B. Bowen disease
C. Erythroplasia of Queyrat
D. Invasive squamous cell carcinoma
Reveal Answer
Answer: C. Erythroplasia of Queyrat
Erythroplasia of Queyrat is PeIN occurring on the glans/inner prepuce (mucosal surface). The mucosal location explains the absence of hyperkeratosis (no stratum corneum on mucosa). The red, velvety appearance is classic. Bowen disease occurs on keratinized shaft skin and shows hyperkeratosis. The intact basement membrane rules out invasive SCC.
Morphology Practical Walk-Through: Seminoma
This block begins the systematic morphology identification review. Use it as a recognition guide.
GROSS recognition of seminoma:
- Enlarged testis (may be 3–5× normal size)
- Cut surface: homogeneous, lobulated, cream-white to tan mass with a characteristic 'fish-flesh' appearance
- Soft to firm consistency
- No cystic spaces, no hemorrhage, no necrosis (these features suggest NSGCT)
- Fibrous septa dividing tumor into lobules may be visible
- Tunica albuginea usually intact (late breech)
MICROSCOPIC recognition of seminoma:
- Large cells arranged in sheets and nests separated by fibrous septa
- Individual cells: large, polygonal, with clear/pale cytoplasm (rich in glycogen — PAS-positive) and prominent central nucleoli
- Nuclei: round, vesicular, with 1–2 prominent nucleoli ('fried-egg' appearance)
- Lymphocytic infiltrate in the fibrous stroma (T-lymphocytes) — diagnostic feature
- Granulomatous reaction in ~20% (mimics TB on gross!)
- ITGCN (intratubular germ cell neoplasia) in adjacent seminiferous tubules
IHC markers (for viva): PLAP+, OCT3/4+, D2-40+, CD117(c-Kit)+; CD30−, AFP−, β-hCG− (a few syncytiotrophoblasts may cause faint β-hCG)
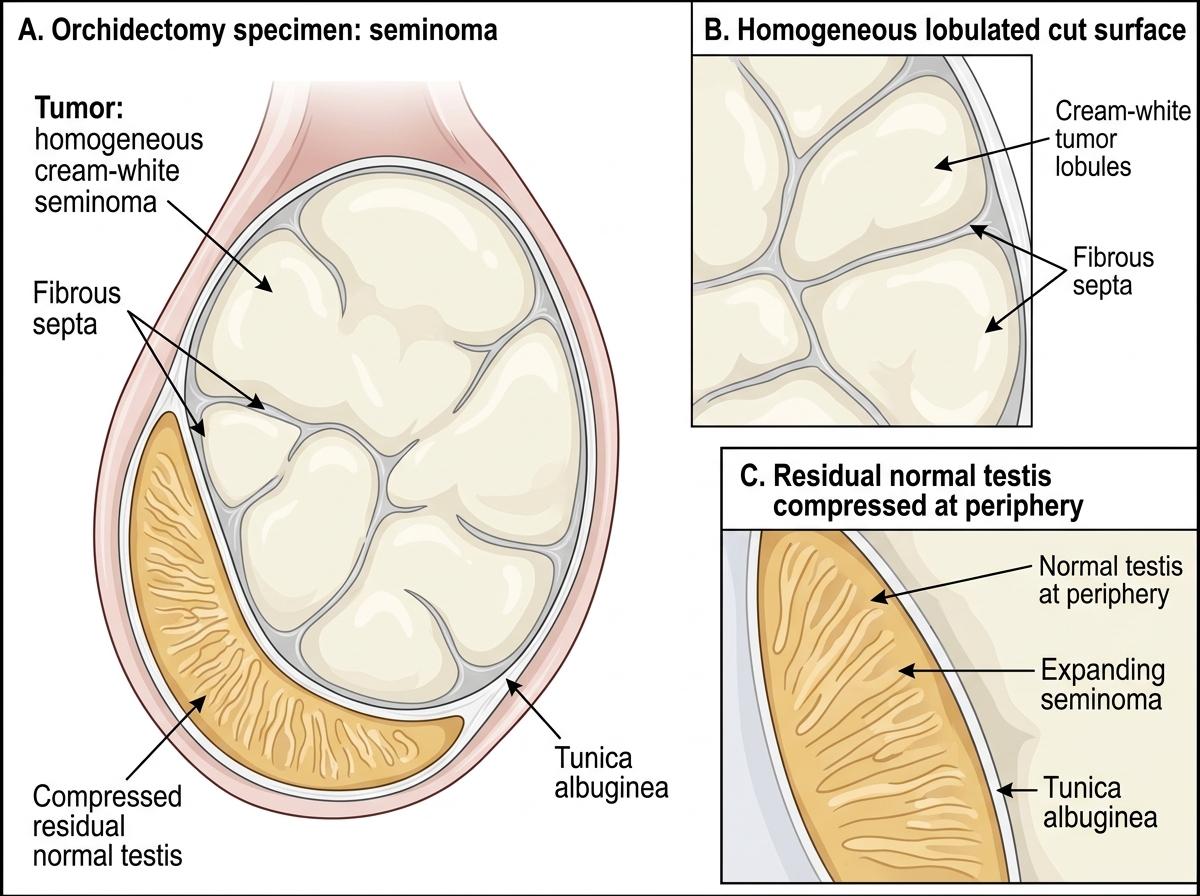
Gross Appearance of Seminoma in Orchidectomy Specimen
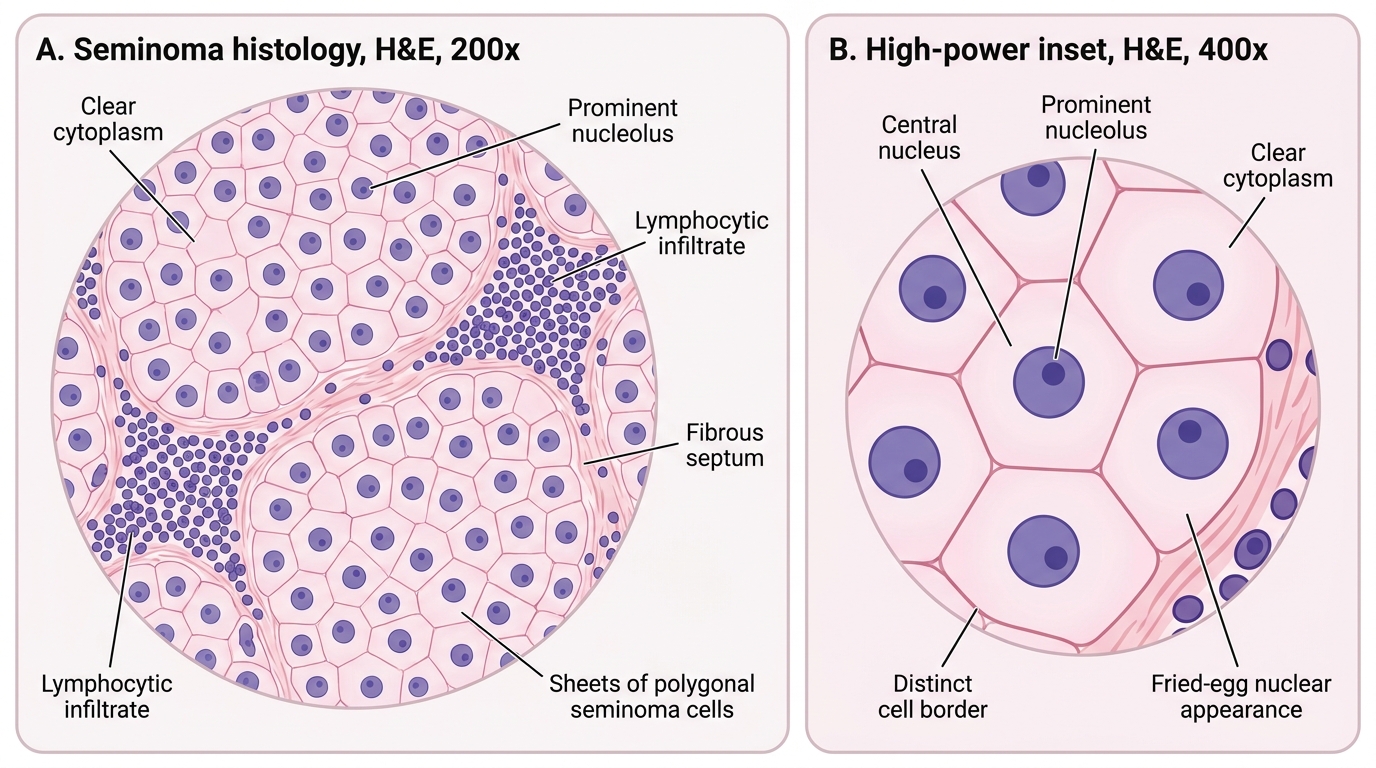
Histology of Seminoma
Morphology Practical Walk-Through: Non-Seminomatous GCT (NSGCT)
GROSS recognition of NSGCT (e.g., mixed GCT, embryonal carcinoma, teratoma):
- Enlarged testis with variegated cut surface — the key distinguishing feature from seminoma
- Areas of hemorrhage (dark red-brown), necrosis (yellow-white), cystic spaces (teratoma), and solid tan-gray areas
- Non-homogeneous, heterogeneous appearance — 'mixed' macroscopic picture
- Cartilage or bone may be palpable in mature teratoma
Individual component histology:
Embryonal carcinoma:
- Sheets, glands, tubules of large, anaplastic epithelial cells with indistinct cell borders
- Marked nuclear pleomorphism, prominent nucleoli, many mitoses and apoptoses
- Necrosis common
- IHC: CD30+, OCT3/4+, AFP− (usually)
Yolk sac tumor (endodermal sinus tumor):
- Schiller-Duval bodies — diagnostic: glomeruloid structures with central capillary surrounded by tumor cells in a loose stroma (resembles glomerulus)
- AFP strongly positive (serum AFP elevated)
- Microcystic/reticular pattern common
Choriocarcinoma:
- Biphasic pattern: cytotrophoblasts (mononucleate, pale) + syncytiotrophoblasts (multinucleate, dark, produces β-hCG)
- Extensive hemorrhage and necrosis
- Worst prognosis of GCTs
Mature teratoma: Well-differentiated tissues from all three germ layers — skin (with sebaceous glands), cartilage, intestinal epithelium, neural tissue
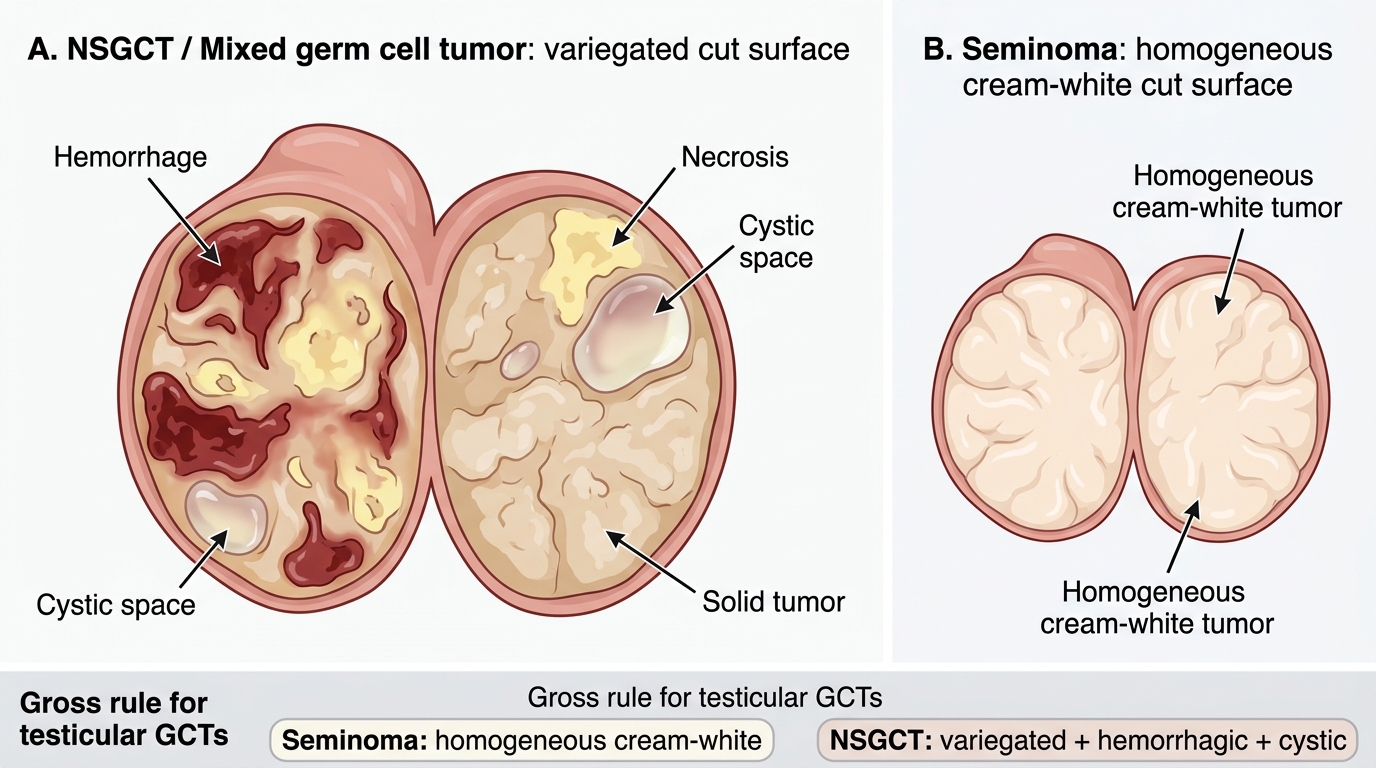
Gross Appearance of NSGCT Versus Seminoma
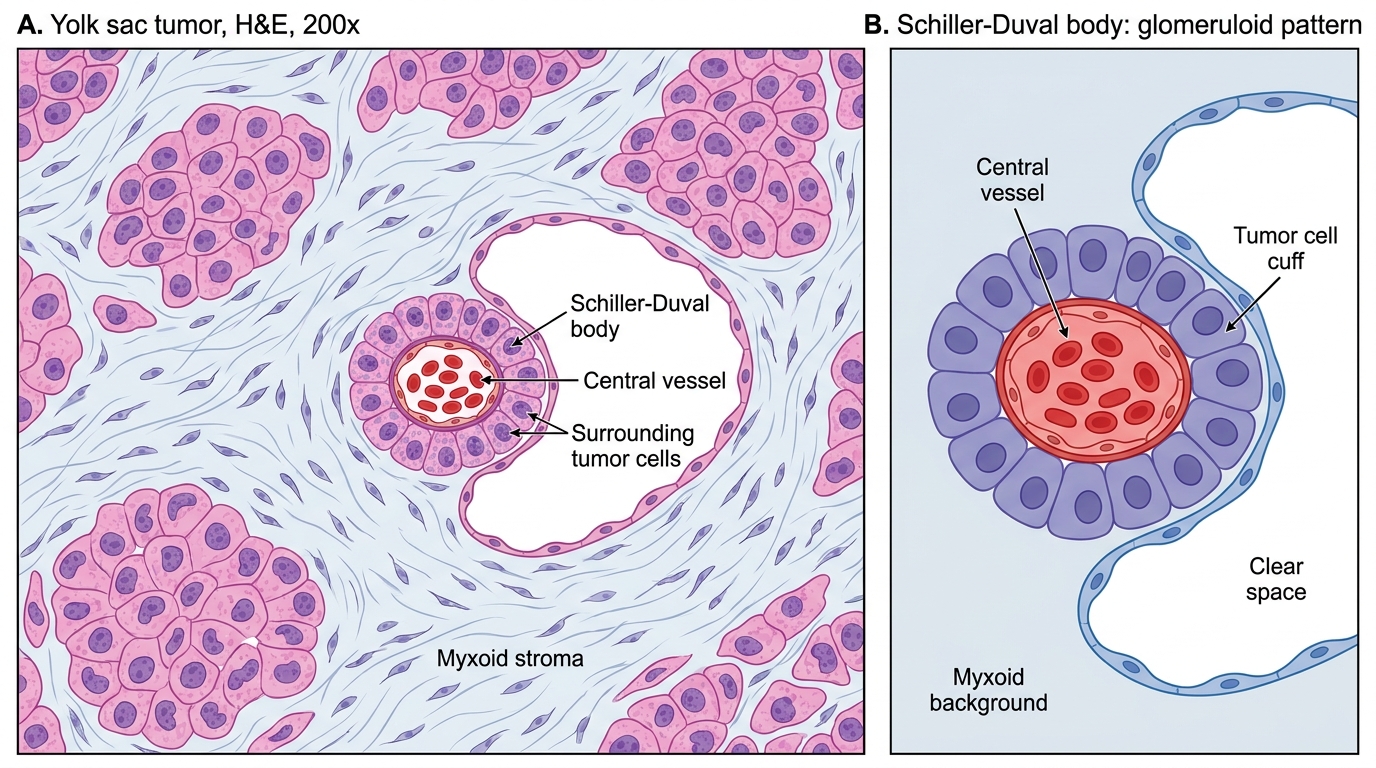
Yolk Sac Tumor: Schiller-Duval Body
CLINICAL PEARL
The 'variegated gross' rule for testicular GCTs: Homogeneous cream-white cut surface = Seminoma. Variegated, hemorrhagic, cystic cut surface = NSGCT. This single gross observation guides the first clinical decision — because seminomas are exquisitely radiosensitive while NSGCTs require BEP chemotherapy. Get this distinction right in the practical and you will impress the examiner.