Page 14 of 21
PA28.{2,6} | Penile Carcinoma & Male Genital Morphology — SDL Guide (Part 4)
Morphology Practical Walk-Through: Nodular Hyperplasia of Prostate (BPH)
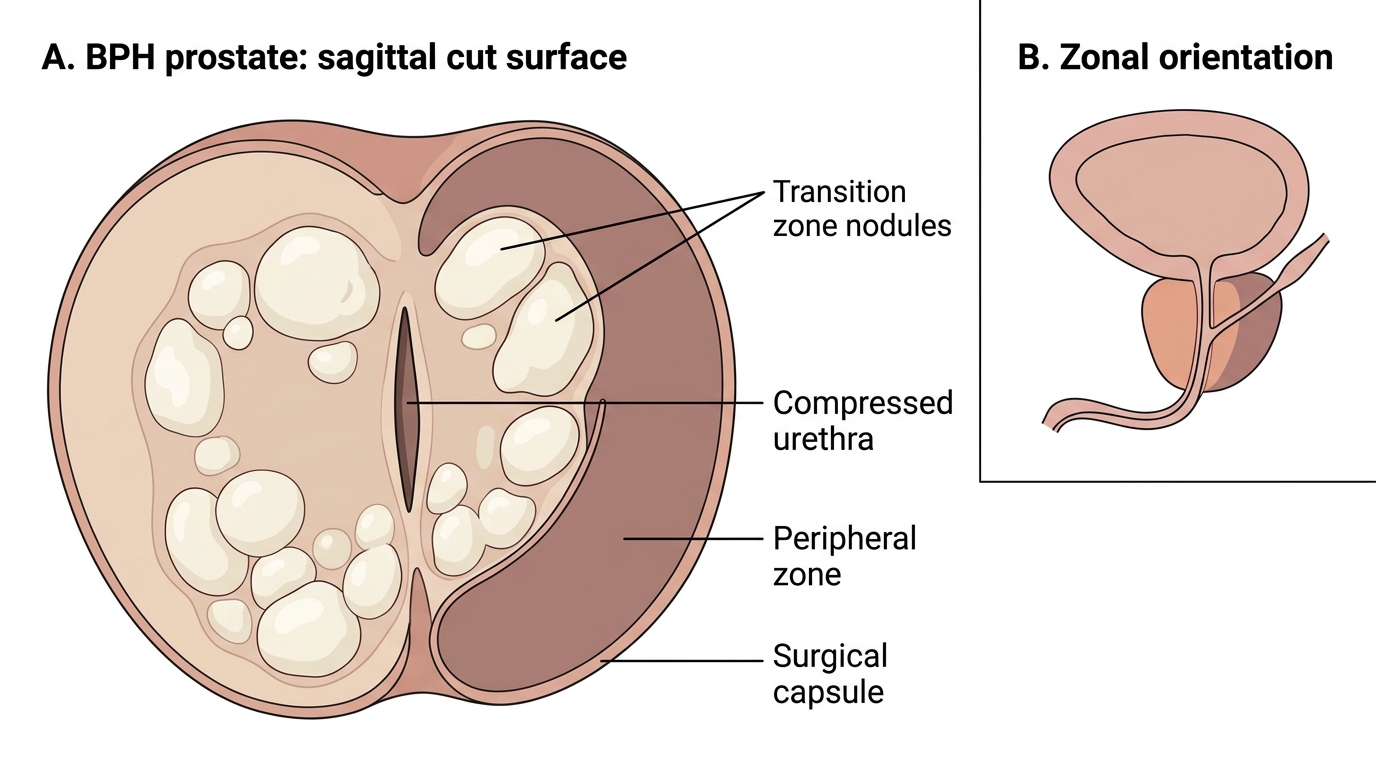
GROSS recognition of BPH:
- Enlarged prostate gland (normal ~20 g; BPH can reach 60–100+ g)
- Nodular enlargement predominantly in the periurethral/transition zone
- Cut surface: well-defined nodules of variable size, cream-white, firm to rubbery
- Central nodules compress the urethra into a slit-like lumen (crescent or slit shape)
- No necrosis, no capsule invasion
- Peripheral zone appears compressed and thinned (pushed outward)
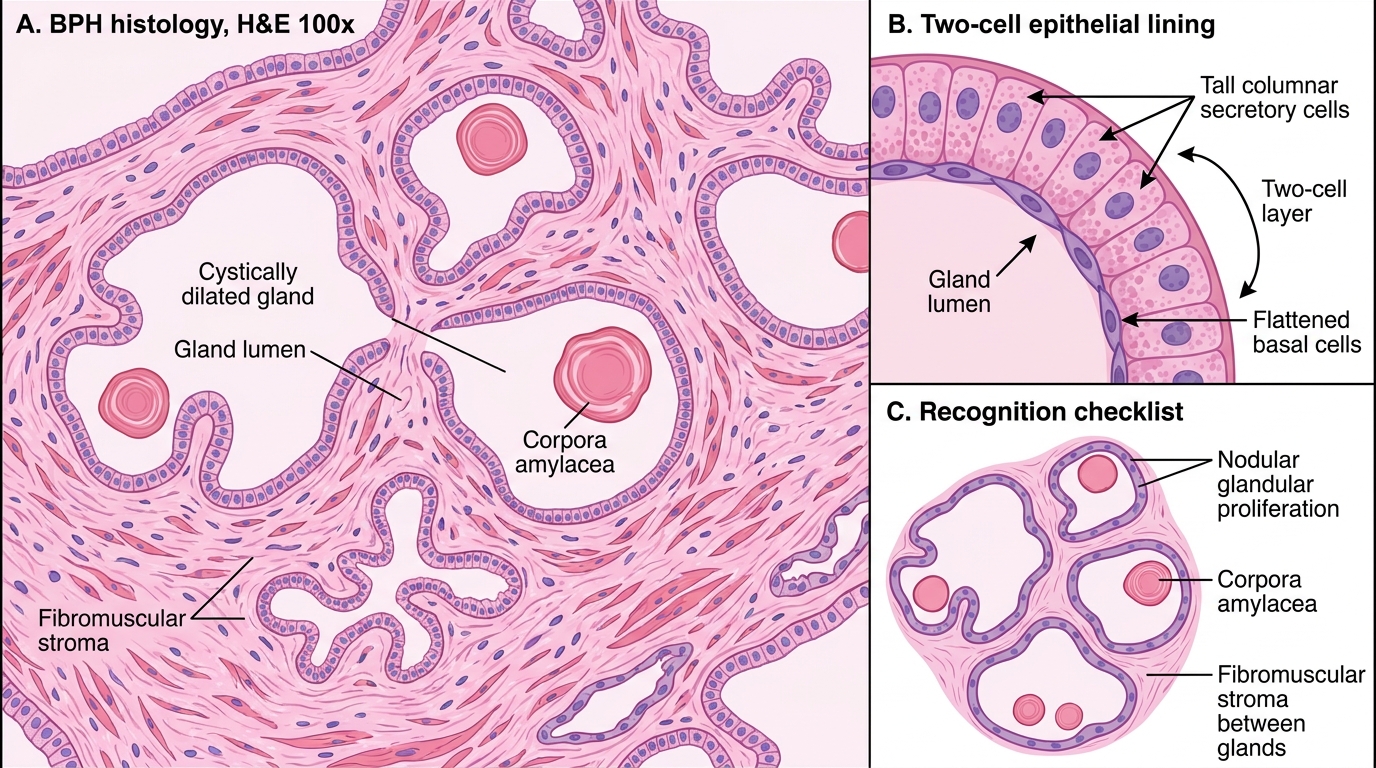
MICROSCOPIC recognition of BPH:
- Nodular proliferation of three components in variable proportions:
1. Glandular component: large, cystically dilated glands lined by two cell layers — inner tall columnar secretory cells and outer flattened basal cells. Gland lumina contain inspissated secretions (corpora amylacea — concentrically laminated calcified bodies, blue-gray on H&E)
2. Fibromuscular stroma: proliferating smooth muscle and fibrous tissue between glands
3. Papillary infoldings of the glandular epithelium into the lumen
- Two-cell layer preservation (columnar + basal) is a key feature distinguishing BPH from carcinoma (which LACKS the basal cell layer)
IHC for basal cells: High-molecular-weight cytokeratin (HMWCK/34βE12) and p63 highlight the basal layer in BPH; this layer is ABSENT in adenocarcinoma.
Gross Morphology of Benign Prostatic Hyperplasia
Histology of Benign Prostatic Hyperplasia
Morphology Practical Walk-Through: Prostatic Adenocarcinoma & Gleason Grading
GROSS recognition of prostatic adenocarcinoma:
- Tumor often not grossly visible, especially in early stages
- Arises in the peripheral zone in ~70% of cases — firm, yellow-white, indurated area on cut surface (NB: the peripheral zone is posterolateral — palpable as a hard nodule on DRE)
- In advanced cases: ill-defined, gritty, gray-white mass in peripheral zone
- Capsule invasion (extraprostatic extension) and seminal vesicle invasion are gross features in locally advanced disease
- On radical prostatectomy specimen: routine inked margins, multisection sampling
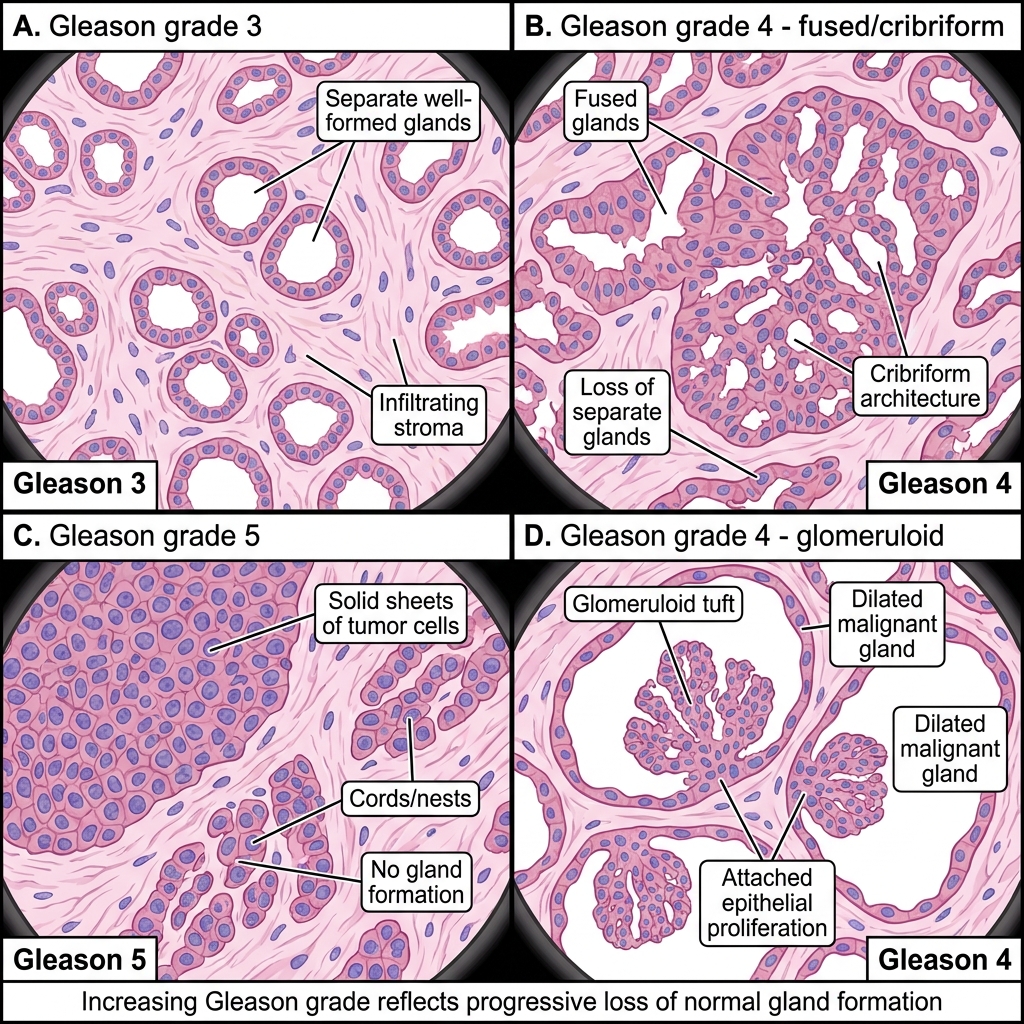
MICROSCOPIC recognition — the Gleason grading system:
Gleason grading is based on the glandular architecture of the tumor (not cytology). There are 5 patterns:
| Gleason Pattern | Architecture | Description |
|---|---|---|
| 1 | Well-formed, closely packed, round uniform glands | (Rarely assigned today) |
| 2 | Well-formed glands, loose arrangement, minimal stromal separation | |
| 3 | Individual, well-formed but variable-sized glands, infiltrating stroma | Most common; glands still well-defined |
| 4 | Poorly formed, fused, or cribriform glands; or glomeruloid pattern | Significant; drives Grade Group 2–4 |
| 5 | No glandular differentiation; sheets, cords, single cells; necrosis | Highest grade |
Gleason score = Primary pattern + Secondary pattern (most common + second most common pattern)
- Score 6 (3+3) = Grade Group 1 — Favorable
- Score 7 (3+4 or 4+3) = Grade Group 2 or 3
- Score 8 = Grade Group 4
- Score 9–10 = Grade Group 5 — Unfavorable
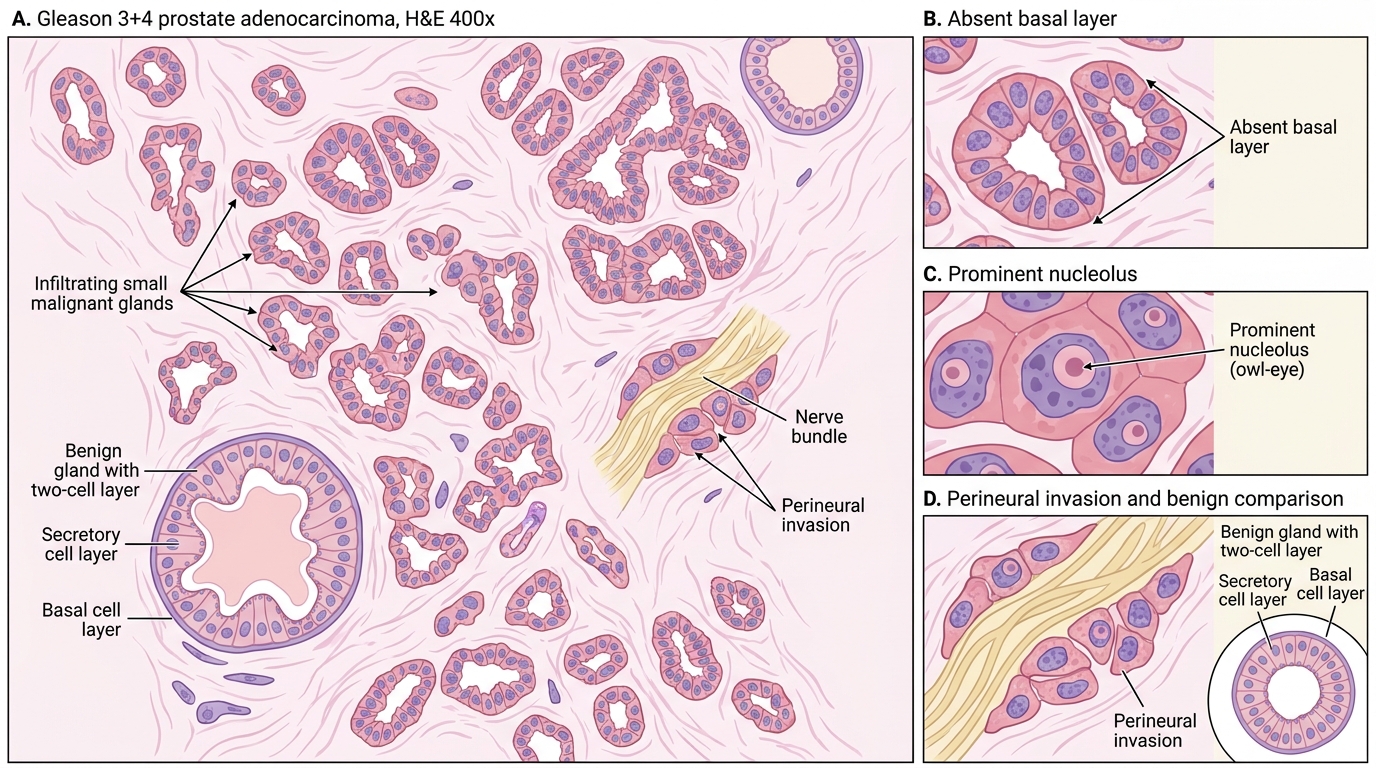
Key microscopic features of adenocarcinoma vs BPH:
- Absent basal cell layer (no HMWCK/p63 staining) — cardinal feature
- Small, irregular infiltrating glands in desmoplastic stroma
- Prominent nucleoli (large, pink — 'owl-eye' nucleoli, ≥1.6 µm)
- Perineural invasion — tumor cells wrapping around nerve bundles in the stroma (pathognomonic)
- Intraluminal crystalloids (hard, angular eosinophilic deposits)
- Luminal blue mucin (amorphous basophilic material)
Gleason Patterns in Prostatic Adenocarcinoma
Gleason 3+4 Prostatic Adenocarcinoma: Key Histologic Features
CLINICAL PEARL
Three 'absent/present' rules for the prostatic adenocarcinoma practical:
1. Absent basal cell layer (HMWCK/p63 negative) — must be absent for carcinoma diagnosis
2. Present perineural invasion — if you see tumor cells around a nerve, it is almost certainly adenocarcinoma
3. Present prominent nucleoli (owl-eye) — in small glands invading stroma, this is carcinoma until proven otherwise
BHP has ALL THREE REVERSED: present basal layer, no perineural invasion, no prominent nucleoli.
Morphology Summary Table — Male Genital Tract Practical Recognition
Use this table as your final revision checklist before the practical:
| Disease | Gross Hallmark | Microscopic Hallmark | Key Marker |
|---|---|---|---|
| Seminoma | Homogeneous cream-white, lobulated | Large cells, clear cytoplasm, prominent nucleoli, lymphocytic stroma | PLAP+, OCT3/4+, CD117+ |
| Embryonal carcinoma | Variegated, hemorrhagic | Anaplastic epithelial sheets/glands, CD30+ | CD30+, OCT3/4+ |
| Yolk sac tumor | Gray-white, mucoid | Schiller-Duval bodies, microcystic | AFP+, serum AFP↑ |
| Choriocarcinoma | Hemorrhagic, necrotic | Cytotrophoblasts + syncytiotrophoblasts | β-hCG+ |
| Mature teratoma | Cystic, cartilage, hair | Tissues from all 3 germ layers | — |
| BPH | Nodular, periurethral, slit-like urethra | Large glands, two-cell layer, corpora amylacea, fibromuscular nodules | HMWCK+ (basal) |
| Prostatic adenocarcinoma | Peripheral zone, firm, yellow-white | Small infiltrating glands, no basal layer, prominent nucleoli, perineural invasion | AMACR(P504S)+, PSA+ |
| Condyloma acuminatum | Cauliflower papillary | Koilocytes, fibrovascular cores, no dysplasia | HPV 6/11 |
| PeIN (Bowen/EQ/BP) | Plaque (keratotic/red) | Full-thickness dysplasia, intact BM | HPV 16/18 |
| Penile SCC | Ulcer with rolled margins | Invasive nests, keratin pearls, desmoplasia | SCC, p16+ (if HPV) |
AMACR (alpha-methylacyl-CoA racemase / P504S) is the most clinically useful IHC stain for prostatic adenocarcinoma — positive in carcinoma, negative in BPH and normal glands.
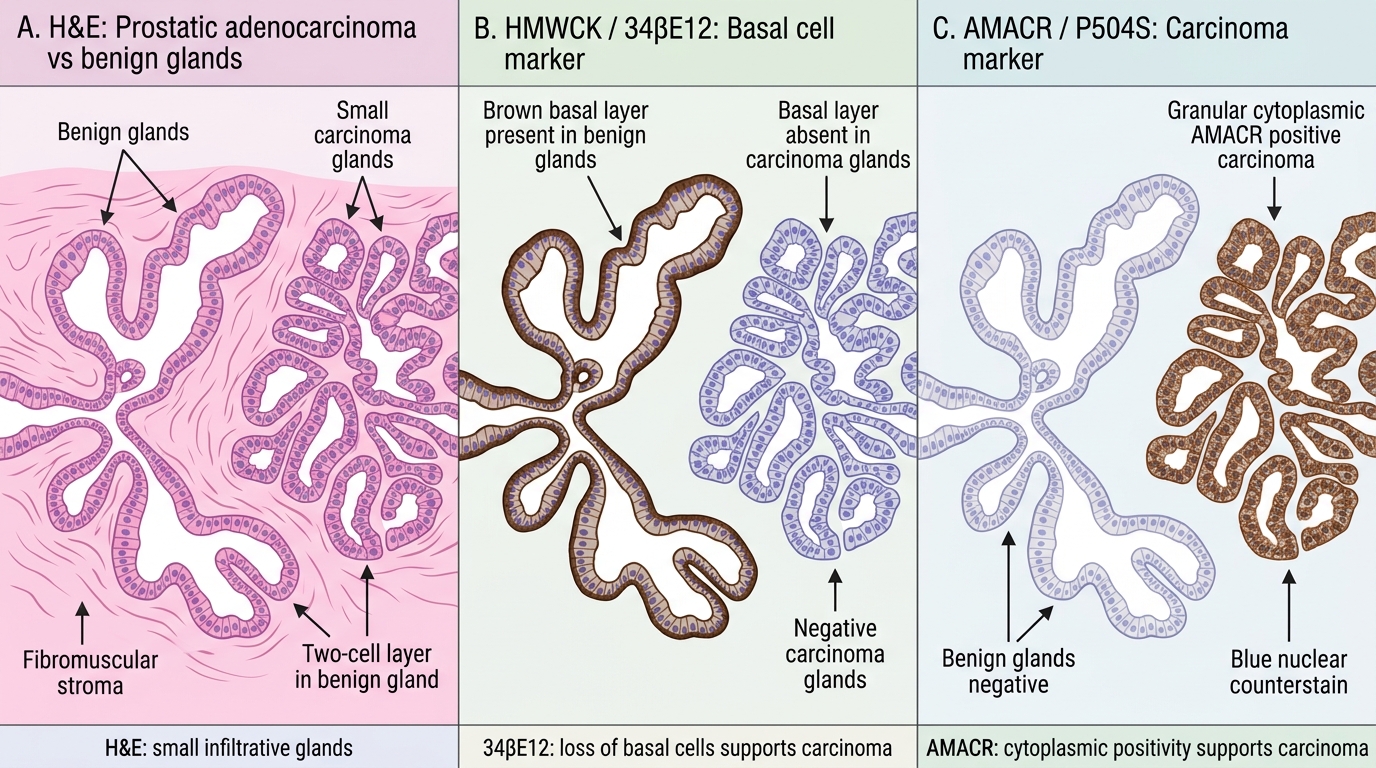
IHC Panel for Prostatic Adenocarcinoma vs BPH
SELF-CHECK
In a pathology practical, a slide shows an enlarged testis with a homogeneous cream-white cut surface divided by fibrous septa. Histology shows sheets of large cells with clear glycogen-rich cytoplasm, prominent central nucleoli, and a dense lymphocytic infiltrate in the fibrous stroma. What is the diagnosis and which immunohistochemical marker is positive?
A. Embryonal carcinoma — CD30 positive
B. Seminoma — PLAP and CD117 positive
C. Yolk sac tumor — AFP positive
D. Mature teratoma — HMWCK positive
Reveal Answer
Answer: B. Seminoma — PLAP and CD117 positive
Seminoma is characterized by a homogeneous cream-white gross appearance, sheets of large clear polygonal cells with prominent nucleoli, and diagnostic lymphocytic infiltrate in fibrous septa. PLAP (placental alkaline phosphatase), OCT3/4, CD117 (c-Kit), and D2-40 are positive. CD30 marks embryonal carcinoma. AFP marks yolk sac tumor. The 'fried-egg' clear cell appearance with lymphocytic stroma is the most tested histological pattern in practical exams.