Page 6 of 21
PA28.3-5 | Prostate: BPH, Carcinoma & Prostatitis — SDL Guide
Learning Objectives
- Classify prostatitis into its four clinical categories and describe the distinct pathogenesis, causative organisms, pathology, and clinical features of each
- Explain the hormonal basis of BPH, focusing on the role of DHT and 5α-reductase in the transition zone
- Describe the nodular hyperplasia morphology of BPH — glandular versus stromal — and correlate with lower urinary tract symptoms (LUTS)
- Enumerate the urological complications of BPH: acute urinary retention, hydronephrosis, UTI, and chronic kidney disease
- Interpret PSA in the context of BPH versus carcinoma, recognising the limits of PSA specificity
- Outline medical management (α-blockers, 5α-reductase inhibitors) and surgical management (TURP) of BPH
- Describe the peripheral zone origin of prostatic adenocarcinoma and explain its androgen-dependent pathogenesis, including the TMPRSS2-ETS fusion
- Apply the Gleason grading system and ISUP grade groups to predict behaviour and guide treatment
- Describe the gross and microscopic features of prostatic adenocarcinoma — small crowded glands, prominent nucleoli, absent basal layer, perineural invasion
- Explain the routes of spread of prostate cancer, with emphasis on osteoblastic bone metastases
- Outline PSA screening, staging, and the principles of androgen deprivation therapy
INSTRUCTIONS
Prostate disease is among the most common cause of morbidity in aging men worldwide — BPH affects more than half of men over 60, and prostate cancer is the second most common cancer in men globally. In India, an ageing population and rising screening awareness are pushing these diseases into the clinical spotlight. This module builds your mechanistic framework — from DHT signalling in the transition zone to Gleason grade groups in the peripheral zone — so that you can confidently interpret a PSA report, describe a biopsy finding, and counsel a patient on treatment choices. Year-1 foundations you will use here: anatomy of the prostate zones (McNeal), androgen physiology (testosterone → DHT via 5α-reductase), and basic concepts of tumour grading.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 21 (Male Genital System) (textbook)
- Harsh Mohan — Textbook of Pathology, 8th ed., Ch. 22 (Male Reproductive System) (textbook)
- Underwood's Pathology, 7th ed., Ch. 19 (Urinary and Male Genital Systems) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 68-year-old retired schoolteacher visits his GP with a six-month history of getting up three times every night to pass urine — small amounts each time — followed by a weak, hesitant stream and a persistent feeling that his bladder never fully empties. His PSA is 5.2 ng/mL. His GP performs a digital rectal examination and feels a smooth, symmetrically enlarged, rubbery prostate. He is reassured: 'It's probably just BPH.'
Six months later he returns. He has had two urinary tract infections. His PSA is now 8.7 ng/mL. A transrectal ultrasound-guided biopsy is performed. The histology report reads: Gleason 4+3=7, ISUP Grade Group 3, perineural invasion present, two of twelve cores positive, right peripheral zone.
Same gland, same patient, two completely different diseases — occurring simultaneously. The prostate is unique in that it harbours three major pathological processes — prostatitis, BPH, and carcinoma — that can mimic, mask, or coexist with each other. Getting them right is one of the most clinically impactful things you will learn in Pathology this year.
WHY THIS MATTERS
- PA28.3 (BPH) is a guaranteed long-answer or structured question in university exams; it is also the number-one urological presentation in general medicine wards.
- PA28.4 (carcinoma) is a high-yield integrated question crossing Pathology, Surgery, and Oncology; PSA interpretation and Gleason grading appear repeatedly in NBE/NExT papers.
- PA28.5 (prostatitis) is shorter but tested as a short note and in differential-diagnosis MCQs; chronic pelvic pain syndrome is one of the most under-recognised clinical entities.
- Clinico-pathological pearls: BPH → central zone (transition zone), never premalignant; carcinoma → peripheral zone, androgen-dependent, osteoblastic metastases to spine/pelvis.
- Year-1 bridge: testosterone → DHT (5α-reductase, Type 2 in prostate); McNeal zones of the prostate (transition, central, peripheral).
RECALL
Before proceeding, briefly recall:
1. McNeal zones of the prostate — which zone surrounds the urethra (transition zone), which zone is palpated on DRE (peripheral zone), and roughly what percentage of the normal gland each occupies.
2. Testosterone → DHT conversion — which enzyme catalyses this, where is it expressed in the prostate, and what is DHT's role in prostatic growth?
3. PSA (prostate-specific antigen) — is it specific for cancer? What is the normal range? What else can raise it?
4. Basic tumour grading concepts — what does it mean to grade a tumour, and why does grade predict prognosis better than size alone in adenocarcinomas?
If any of these feel uncertain, pause and revisit your Year-1 Anatomy and Physiology notes — this module builds directly on all four concepts.
Normal Prostate Anatomy: The Zone Framework
Understanding prostate pathology requires the McNeal zonal anatomy, because each disease preferentially targets a specific zone:
| Zone | Location | % of Gland | Disease |
|---|---|---|---|
| Transition zone | Periurethral, flanks proximal urethra | ~5–10% (normal) | BPH — can expand to 90% of gland |
| Central zone | Surrounds ejaculatory ducts, base | ~20–25% | Rarely involved in disease |
| Peripheral zone | Posterior and posterolateral, palpable on DRE | ~70–75% | Carcinoma (~70%); Prostatitis |
| Anterior fibromuscular stroma | Anterior surface | — | Smooth muscle, no glands |
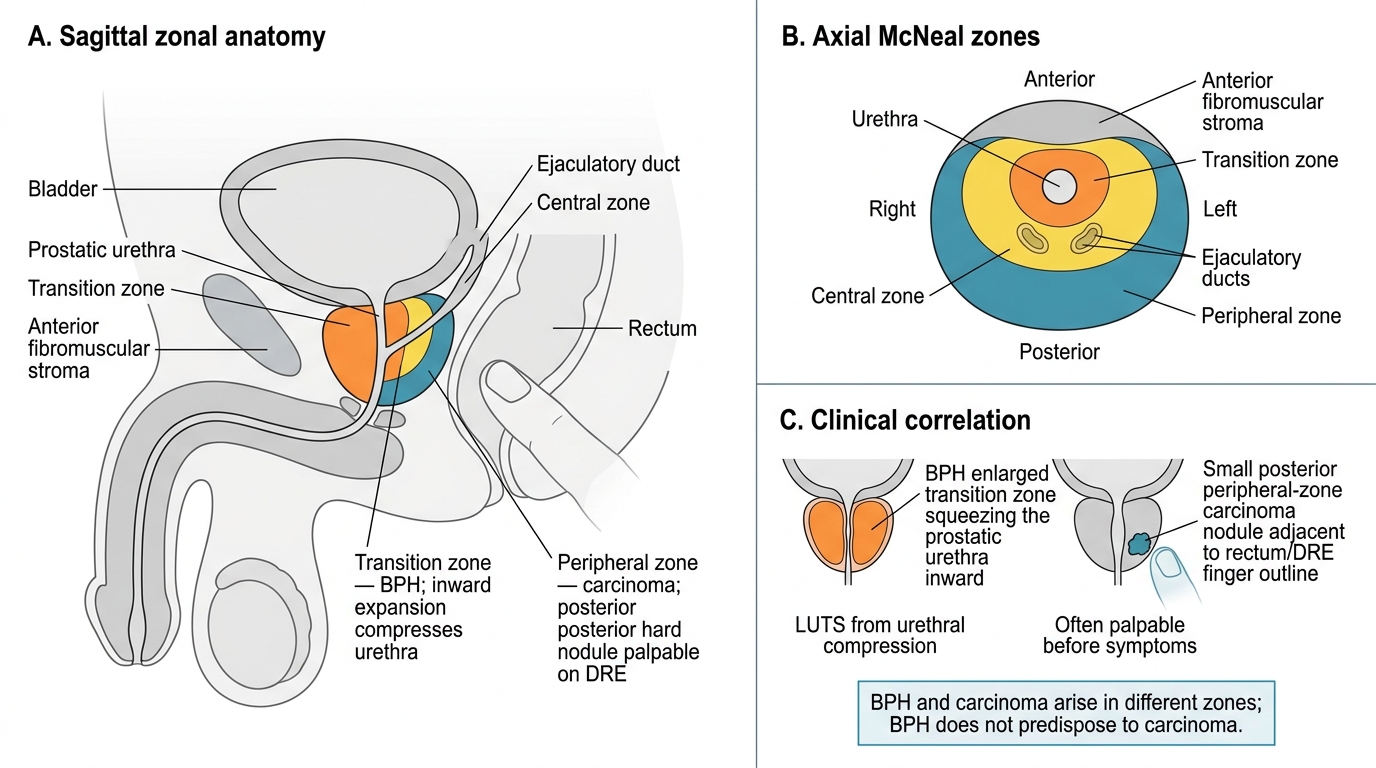
McNeal Zones of the Prostate and Disease Correlation
Clinical correlation: BPH expands inward and compresses the urethra (hence LUTS); carcinoma arises posteriorly and is palpable on DRE as a hard nodule before it becomes symptomatic. This anatomical separation explains why BPH does not predispose to carcinoma — they are independent diseases arising in different zones with different molecular mechanisms.
Prostatitis: Classification and Overview
Prostatitis encompasses four clinical syndromes classified by the National Institutes of Health (NIH) into Categories I–IV:
| NIH Category | Name | WBC in EPS | Culture | Key Feature |
|---|---|---|---|---|
| I | Acute bacterial prostatitis | +++ | Positive | Systemic sepsis possible |
| II | Chronic bacterial prostatitis | + | Positive | Recurrent UTI, same organism |
| III | Chronic pelvic pain syndrome (CPPS) | IIIa: +; IIIb: − | Negative | Commonest form (~90–95%) |
| IV | Asymptomatic inflammatory prostatitis | + | Variable | Incidental biopsy finding |
EPS = expressed prostatic secretions
The majority of clinical prostatitis (90–95%) is Category III (CPPS), which has no proven bacterial cause and is thought to involve neurogenic inflammation, pelvic floor dysfunction, and immune dysregulation.
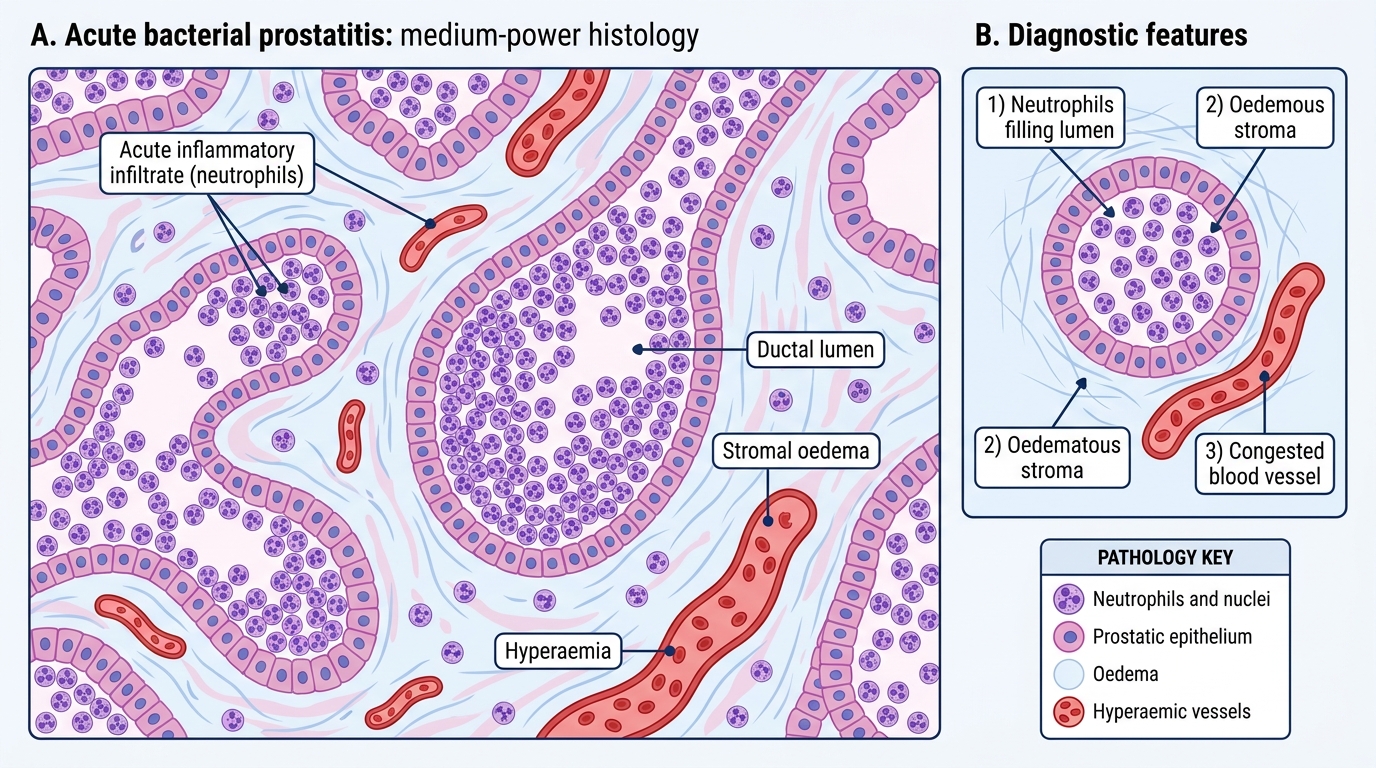
Acute Bacterial Prostatitis: Histology
Acute and Chronic Bacterial Prostatitis
Acute Bacterial Prostatitis (NIH Category I)
Aetiology: Most commonly caused by gram-negative enteric organisms — Escherichia coli (most frequent), Klebsiella, Proteus, Pseudomonas. Organisms reach the prostate via ascending urethral infection (most common), reflux of infected urine, haematogenous spread, or iatrogenic (post-TRUS biopsy).
Pathology: Acute suppurative inflammation — ducts and acini packed with neutrophils, stromal oedema, hyperaemia. Microabscesses may form; coalescence produces a prostatic abscess (requires surgical drainage).
Clinical features: Sudden onset fever, chills, rigors; severe perineal/low back pain; exquisitely tender, boggy prostate on DRE (do NOT vigorously massage — risk of bacteraemia); dysuria, frequency, acute urinary retention. PSA is markedly elevated (can exceed 100 ng/mL — do not order or interpret PSA in acute prostatitis).
Treatment: IV fluoroquinolones or aminoglycosides; total duration 4–6 weeks (long course because the blood-prostate barrier limits antibiotic penetration in chronic disease).
Chronic Bacterial Prostatitis (NIH Category II)
Aetiology: Same organisms as acute; persistence due to bacterial biofilm formation in prostatic calculi or poor antibiotic penetration.
Pathology: Lymphocytes, plasma cells, macrophages, and occasional neutrophils within and around acini and in periductal stroma. Chronic inflammation → fibrosis.
Clinical features: The hallmark is recurrent UTI with the same organism in an otherwise well man; perineal discomfort, post-ejaculatory pain; DRE may be mildly tender or normal; PSA mildly elevated.
Diagnosis: Meares-Stamey 4-glass test (or simpler 2-glass pre/post-massage test) — bacterial counts significantly higher in expressed prostatic secretions (EPS) than in the initial urethral voided urine localises infection to the prostate.