Page 7 of 21
PA28.3-5 | Prostate: BPH, Carcinoma & Prostatitis — SDL Guide (Part 2)
Chronic Pelvic Pain Syndrome and Granulomatous Prostatitis
Chronic Pelvic Pain Syndrome (CPPS — NIH Category III)
The commonest and most diagnostically challenging form of prostatitis. By definition, cultures are negative.
Pathogenesis: Multifactorial — proposed mechanisms include sterile autoimmune inflammation (molecular mimicry with bacterial antigens), pelvic floor muscle spasm and myofascial trigger points, neurogenic inflammation (substance P, mast cell activation), and psychosocial amplification.
Subtypes:
• IIIa (inflammatory CPPS): WBCs >10/hpf in EPS or post-massage urine — histology shows lymphocytic infiltrate; likely represents residual immune activation.
• IIIb (non-inflammatory CPPS): No excess WBCs — pelvic floor dysfunction predominates.
Clinical features: Pelvic pain for ≥3 of the past 6 months; variable dysuria, frequency; ejaculatory pain; normal or near-normal PSA; DRE often normal or mildly tender. Diagnosis is one of exclusion.
Treatment: Alpha-blockers (relax bladder neck and prostate smooth muscle), NSAIDs, 5α-reductase inhibitors, pelvic floor physiotherapy, psychosocial support.
Granulomatous Prostatitis
Types and causes:
1. Infectious granulomatous prostatitis — Mycobacterium tuberculosis (most important in India; part of urogenital TB); also Histoplasma, Blastomyces in endemic areas.
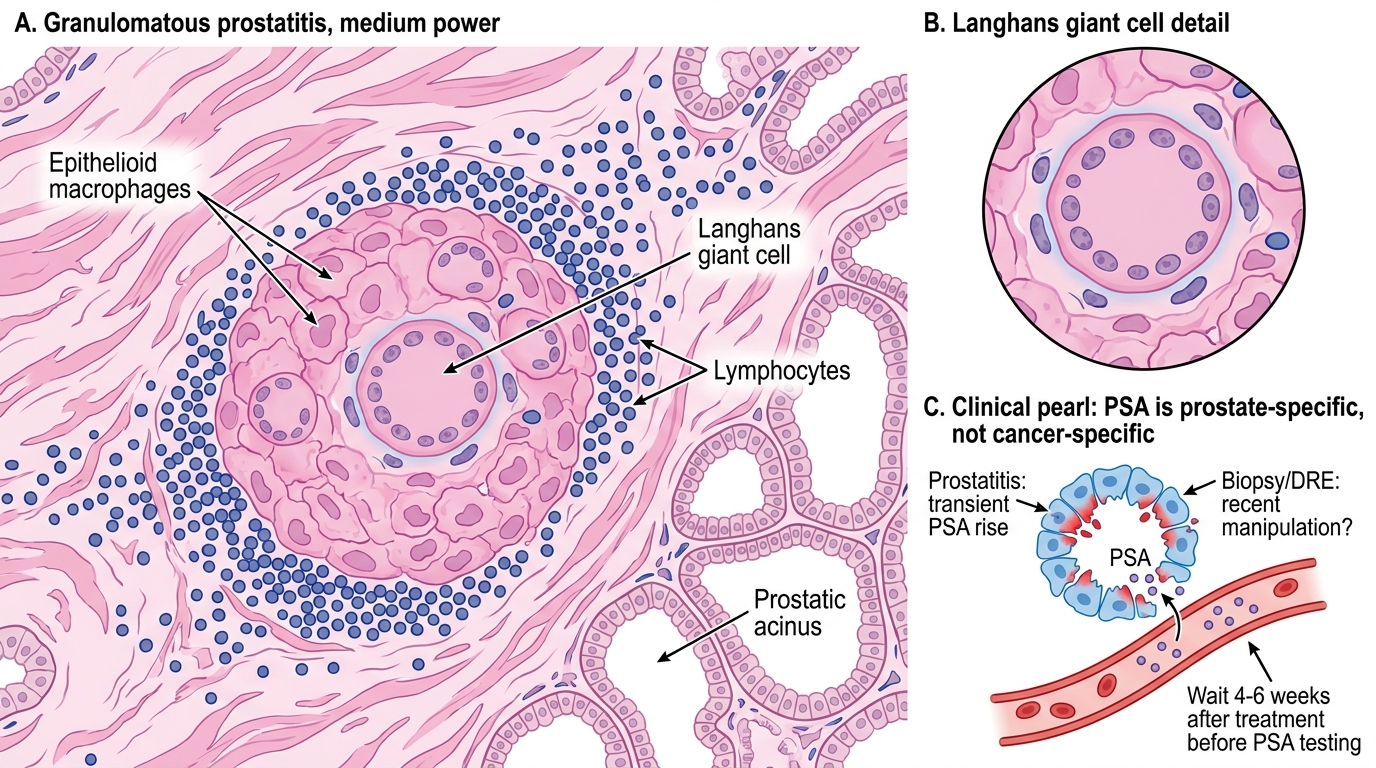
2. Non-specific granulomatous prostatitis — most common type; thought to be a reaction to extravasated prostatic secretions; caseous-free epithelioid granulomas mixed with lipid-laden macrophages.
3. BCG-induced granulomatous prostatitis — iatrogenic, after intravesical BCG therapy for bladder cancer; non-caseating granulomas throughout prostate.
Pathology: Epithelioid macrophages ± Langhans giant cells, lymphocytes; in TB — caseating granulomas with Ziehl-Neelsen-positive bacilli.
Clinical trap: Granulomatous prostatitis can produce a hard, irregular prostate on DRE and elevated PSA — mimicking carcinoma. Biopsy is diagnostic.
Granulomatous Prostatitis: Histology and PSA Pearl
CLINICAL PEARL
PSA is prostate-specific, NOT cancer-specific. Any disruption of the prostate epithelial architecture releases PSA into the circulation — acute prostatitis can push PSA to >100 ng/mL, BPH causes a moderate steady rise (roughly 0.3 ng/mL per gram of tissue), and prostate biopsy causes a sharp spike lasting up to 3 weeks. Always ask: 'When was the DRE? Any recent biopsy? Any UTI or prostatitis?' before interpreting a PSA result. The clinical rule: never order PSA during active prostatitis — wait at least 4–6 weeks after treatment before testing.
Benign Prostatic Hyperplasia: Hormonal Pathogenesis
Benign prostatic hyperplasia (BPH) is a non-neoplastic, non-inflammatory enlargement of the prostate due to nodular hyperplasia of glandular epithelium and fibromuscular stroma in the transition zone.
Epidemiology: Virtually universal with advancing age — histological BPH in ~20% at age 40, ~70% by age 60, >90% by age 80. Symptomatic disease affects ~50% of men over 60. Requires: (1) functioning testes (eunuchs do not develop BPH) and (2) advancing age.
Hormonal pathogenesis — the DHT hypothesis:
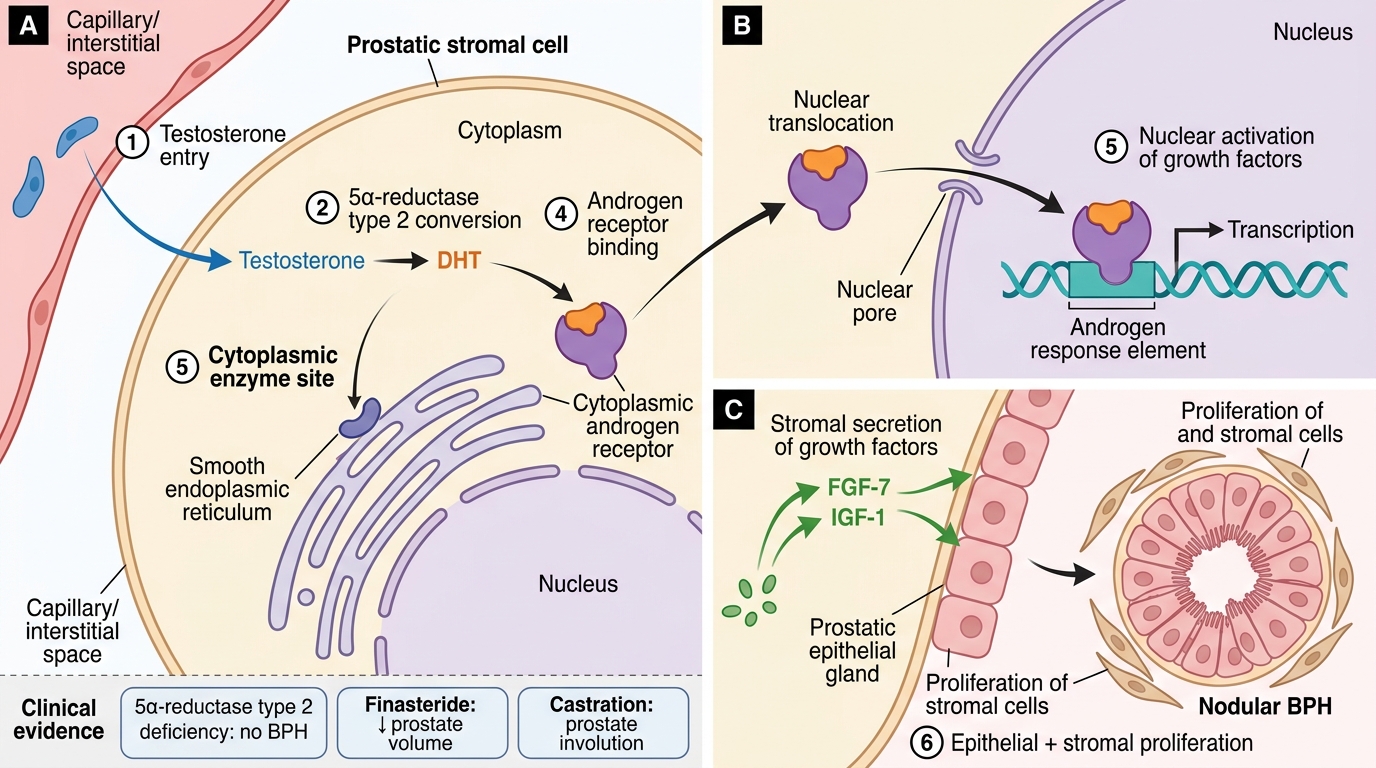
- Testosterone (from Leydig cells) enters prostatic stromal cells and is converted to dihydrotestosterone (DHT) by 5α-reductase type 2 (expressed in prostatic stroma).
- DHT binds the androgen receptor with ~5× greater affinity than testosterone and dissociates more slowly → more potent and sustained nuclear signal.
- DHT activates growth factor signalling (IGF-1, FGF-7/KGF, EGF) → promotes epithelial and stromal cell proliferation AND inhibits apoptosis → net tissue accumulation.
- Disequilibrium between proliferation and apoptosis, rather than de-novo oncogenesis, is the mechanism → BPH is hyperplasia, not neoplasia.
DHT-Driven Pathogenesis of BPH
Supporting evidence for DHT hypothesis:
• Men with 5α-reductase type 2 deficiency (pseudohermaphroditism) have absent prostatic tissue and never develop BPH.
• Finasteride (5α-reductase type 2 inhibitor) reduces prostate volume by 20–30% and relieves LUTS — direct therapeutic proof of the DHT mechanism.
• Castration causes prostate involution.
BPH: Morphology — Gross and Microscopic
Gross appearance:
The enlarged prostate in BPH typically weighs 20–100+ grams (normal ~20 g). The transition zone expands concentrically, producing a pale grey, firm, multinodular mass that compresses the peripheral zone and distorts the urethra into a narrow slit or crescentic channel. The cut surface shows well-defined nodules with a honeycomb-like appearance due to cystically dilated glands oozing milky fluid. The outer (surgical) capsule is formed by compressed peripheral zone tissue — important for TURP (the surgeon resects within this capsule).
Microscopic components — two main types of nodules:
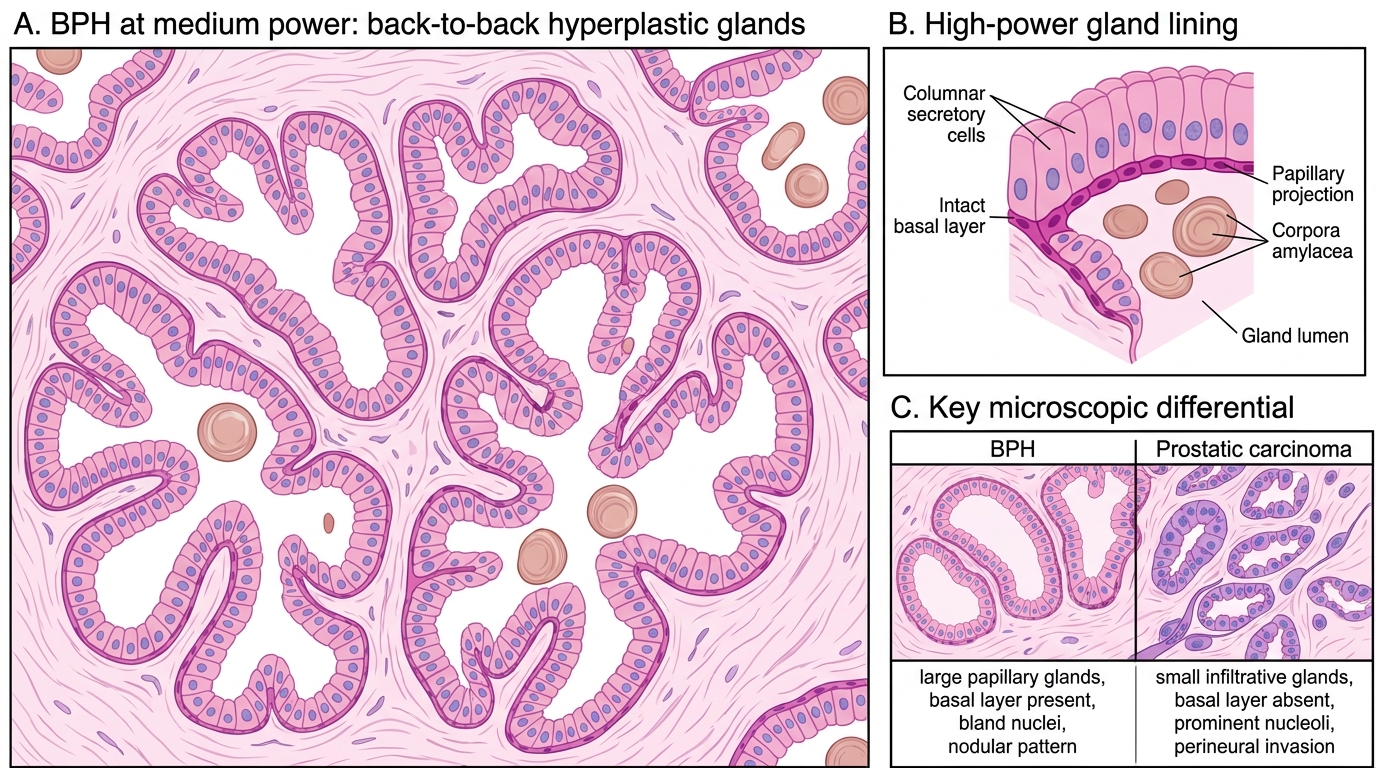
1. Glandular (epithelial) nodules — composed of hyperplastic, back-to-back glands lined by two layers:
• Inner layer: tall columnar secretory cells (pale cytoplasm) often forming papillary projections into the lumen.
• Outer layer: flattened basal cells (small, dark nuclei) — this intact basal cell layer is the key microscopic feature that distinguishes BPH from carcinoma.
• Lumina contain corpora amylacea (pink, laminated concentric structures from condensed secretions — normal finding, increases with age).
- Stromal nodules — predominantly composed of smooth muscle and fibrous tissue with sparse glands; feel firmer and are less responsive to 5α-reductase inhibitors (which primarily shrink glandular tissue).
Histology of Benign Prostatic Hyperplasia
Key microscopic differential (BPH vs Carcinoma):
| Feature | BPH | Carcinoma |
|---|---|---|
| Gland architecture | Large, papillary, back-to-back | Small, crowded, infiltrative |
| Basal cell layer | Present (two cell layers) | Absent |
| Nuclei | Bland, uniform | Enlarged, prominent nucleoli |
| Pattern | Nodular, zonal | Haphazard infiltration |
| Perineural invasion | Absent | Present |