Page 8 of 21
PA28.3-5 | Prostate: BPH, Carcinoma & Prostatitis — SDL Guide (Part 3)
BPH: Clinical Features, Complications, and Diagnosis
Lower Urinary Tract Symptoms (LUTS):
BPH causes LUTS through two mechanisms: (1) static component — mechanical compression of the urethra by enlarged gland; (2) dynamic component — increased α-adrenergic tone in prostatic smooth muscle (this is why α-blockers work acutely).
Obstructive symptoms (voiding):
• Hesitancy (difficulty initiating stream)
• Weak/reduced urinary stream
• Intermittency
• Terminal dribbling
• Incomplete bladder emptying (increased post-void residual)
Irritative symptoms (storage):
• Urgency and urge incontinence
• Frequency (day)
• Nocturia (often the most bothersome symptom)
Symptoms are quantified by the International Prostate Symptom Score (IPSS): 7 questions, score 0–35 (mild ≤7, moderate 8–19, severe ≥20).
Complications of untreated/advanced BPH:
1. Acute urinary retention (AUR) — sudden, painful inability to void; precipitated by cold weather, constipation, alcohol, anticholinergics; requires emergency catheterisation.
2. Chronic urinary retention — large post-void residual → overflow incontinence (painless, dribbling).
3. Recurrent UTI — stagnant residual urine → bacterial colonisation.
4. Bladder calculi — urinary stasis precipitates stone formation.
5. Bladder hypertrophy and trabeculation → diverticula (false diverticula through muscle bundles).
6. Bilateral hydronephrosis and hydro-ureter — back pressure from chronically elevated intravesical pressure → bilateral ureteric obstruction → obstructive uropathy → chronic kidney disease.
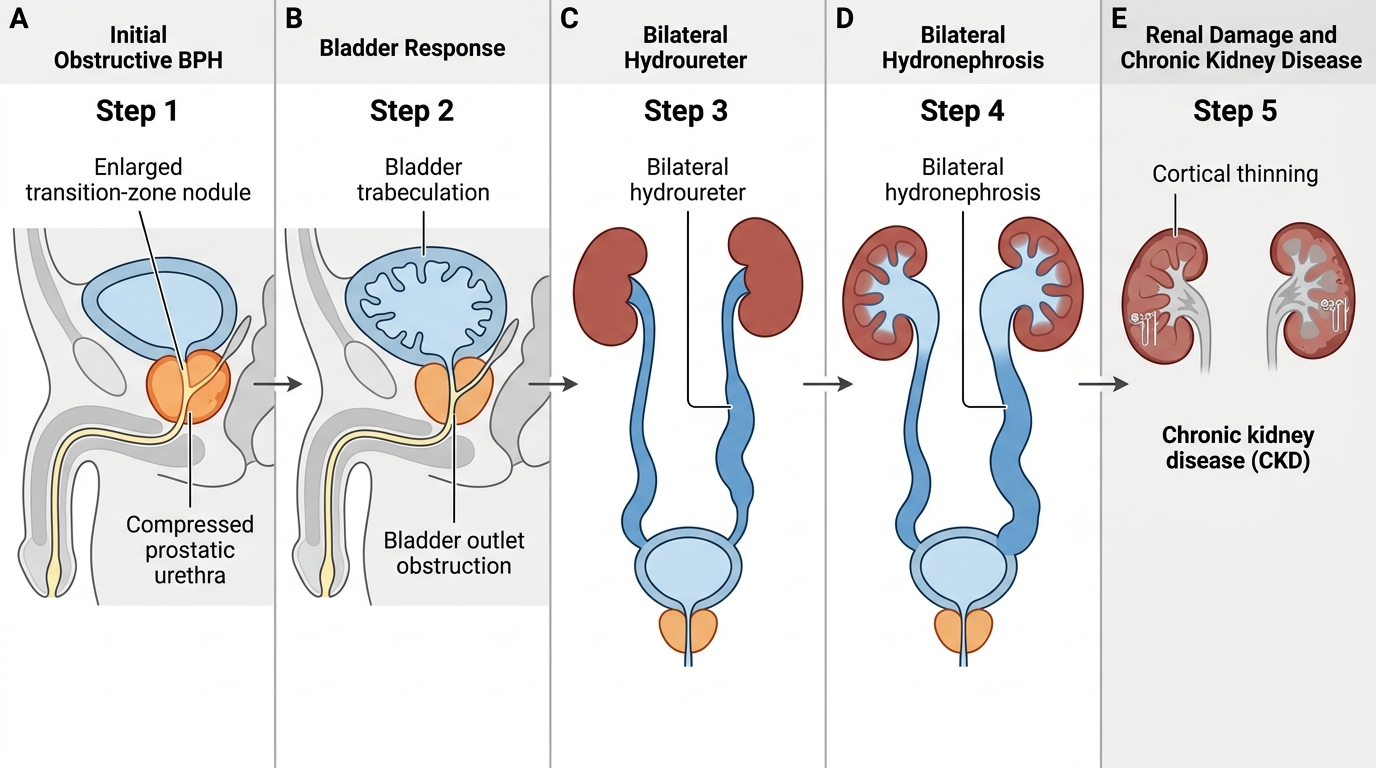
Sequential Complications of Untreated BPH
Investigations:
• DRE: Symmetrically enlarged, smooth, rubbery (elastic) prostate with preserved median sulcus — classical BPH feel. Compare with carcinoma: asymmetric hard nodule, loss of sulcus.
• PSA: Usually ≤10 ng/mL in BPH; ~0.3 ng/mL per gram tissue (PSA density helps); higher levels mandate biopsy to exclude carcinoma.
• Uroflowmetry: Maximum flow rate (Qmax) <10 mL/s suggests obstruction (normal >15).
• Ultrasound (transabdominal/TRUS): Measures prostate volume, post-void residual, upper tract dilation.
• Serum creatinine: Screens for obstructive nephropathy.
Management:
• Watchful waiting: mild symptoms (IPSS ≤7), no complications.
• α-adrenergic blockers (tamsulosin, alfuzosin, silodosin): Relax prostatic smooth muscle → immediate improvement in flow rate; do not shrink gland; first-line for moderate symptoms.
• 5α-reductase inhibitors (finasteride, dutasteride): Block DHT production → shrink gland 20–30% over 3–6 months; most effective in large glands (>40 g); also reduce PSA by ~50% (remember to double observed PSA when monitoring on finasteride).
• Combination therapy: α-blocker + 5α-reductase inhibitor superior to either alone for large glands.
• Surgical — TURP (Transurethral Resection of the Prostate): Gold standard surgical procedure; resectoscope removes transition-zone chips under endoscopic vision; pathology on chips may occasionally reveal incidental carcinoma (Stage T1a/T1b).
SELF-CHECK
A 65-year-old man on finasteride 5 mg/day for two years has his PSA measured: it returns at 3.5 ng/mL. What is the most appropriate next step in his PSA interpretation?
A. Reassure him — PSA <4 ng/mL is normal
B. Double the observed PSA to estimate the true value (effective PSA ~7.0 ng/mL) and consider biopsy
C. Stop finasteride for 3 months and retest
D. Order MRI prostate — PSA is unreliable on finasteride
Reveal Answer
Answer: B. Double the observed PSA to estimate the true value (effective PSA ~7.0 ng/mL) and consider biopsy
Finasteride (5α-reductase inhibitor) suppresses PSA by approximately 50% by reducing DHT-driven PSA secretion. Therefore, the observed PSA must be multiplied by 2 to estimate the 'true' level. An adjusted PSA of ~7.0 ng/mL warrants further evaluation (biopsy or MRI), as it falls above the 4 ng/mL threshold used in unmedicated men. Ignoring this correction would falsely reassure a clinician about a potentially significant rise. This correction rule is one of the most commonly tested clinical pharmacology/pathology integration points.
CLINICAL PEARL
BPH is hyperplasia, not hypertrophy, and it is NOT premalignant. Many students (and some clinicians) conflate BPH with prostate cancer risk. The two diseases arise in different zones (transition vs peripheral), through entirely different molecular mechanisms (DHT-driven growth imbalance vs oncogenic fusion/mutation), and share no causal link. A man with massive BPH has NO higher risk of peripheral-zone adenocarcinoma than a man with a small prostate. The reason PSA monitoring matters in BPH is not because BPH transforms — it's because carcinoma can coexist and is masked by the elevated PSA baseline.
Prostate Carcinoma: Epidemiology and Pathogenesis
Prostatic adenocarcinoma is the most common carcinoma in men in Western countries and the second most common cause of cancer death in men globally. In India, incidence is lower but rising with urbanisation and increased screening awareness.
Epidemiology:
• Most common in men >65 years; rare before 45.
• Highest incidence: African-American men; lowest: East Asian men (though immigrants from low-risk countries progressively acquire host-country risk → environmental and dietary factors important).
• Risk factors: age, family history (first-degree relative doubles risk; BRCA2 mutations confer high risk), high-fat Western diet, androgens (castrated men do not develop carcinoma).
Molecular pathogenesis:
Three key molecular events characterise the development of prostatic adenocarcinoma:
- Androgen receptor (AR) signalling is central and obligate. Testosterone → DHT → AR activation drives transcription of proliferation genes. This explains why androgen deprivation therapy is the cornerstone of systemic treatment.
- TMPRSS2-ETS gene fusion — most common somatic alteration in prostate cancer (~50% of cases). TMPRSS2 (transmembrane serine protease 2) is an androgen-regulated gene on chromosome 21q22; fusion with the ERG transcription factor (or other ETS family members) places ERG under androgen control → oncogenic transcription factor driven by the very hormone required for normal growth → explains why androgen axis remains druggable even in advanced disease.
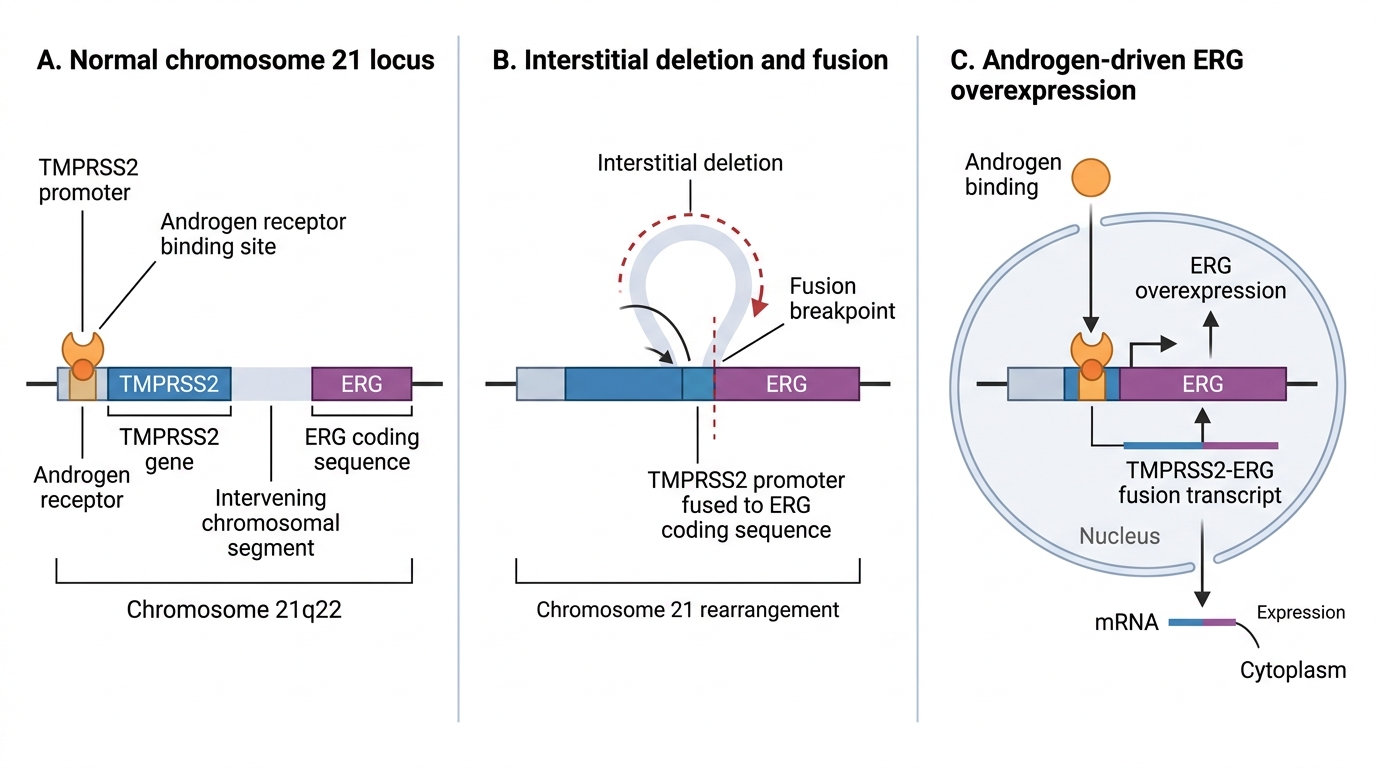
TMPRSS2-ERG Fusion in Prostate Cancer
- Epigenetic silencing of tumour suppressor genes — most notably GSTP1 (glutathione S-transferase P1) promoter hypermethylation (present in >90% of prostate cancers and high-grade PIN lesions; a potential early detection marker). Loss of NKX3.1 (homeobox tumour suppressor) and PTEN (phosphatase and tensin homolog) phosphatase are also important.
Prostatic intraepithelial neoplasia (PIN):
High-grade PIN (HGPIN) is the recognised precursor lesion — architecturally intact (basal layer present) but cytologically malignant (nuclear enlargement, prominent nucleoli). Presence of HGPIN on biopsy mandates repeat biopsy. Low-grade PIN has no clinical significance.
Prostate Carcinoma: Gross and Microscopic Morphology
Gross appearance:
Most (70%) arise in the peripheral zone → posterior and posterolateral capsule. On cross-section: ill-defined, firm, grey-white gritty areas contrasting with the yellow-tan normal prostatic tissue. Unlike BPH, carcinoma lacks the nodular pattern — it infiltrates diffusely and may be grossly undetectable in early stages, discoverable only by histology.
Histological pattern — acinar adenocarcinoma (most common):
The hallmark is small, crowded, irregular glands infiltrating between normal larger glands and stroma.
Key microscopic features (learn all five — exam standard):
- Small, crowded, back-to-back glands — haphazardly arranged, without fibromuscular stroma between them (contrast with BPH: large glands with intervening stroma).
- Single-layer epithelium — absent basal cell layer — only secretory columnar cells; no basal cells identifiable on H&E or on immunohistochemistry for high-molecular-weight cytokeratin (34βE12) or p63. This is the most important distinguishing feature from BPH and HGPIN.
- Prominent nucleoli — large, conspicuous, eosinophilic nucleoli in vesicular nuclei (sometimes described as 'cherry-red'); a reliable cytological marker of malignancy in prostate.
- Perineural invasion — malignant glands tracking along and around nerve sheaths within the prostate; a diagnostic criterion for carcinoma (benign glands do NOT invade nerves); also a route of extra-capsular spread.
- Intraluminal features — pink amorphous crystalloids and blue mucinous secretions (acidic mucin) in lumina; not specific but supportive.
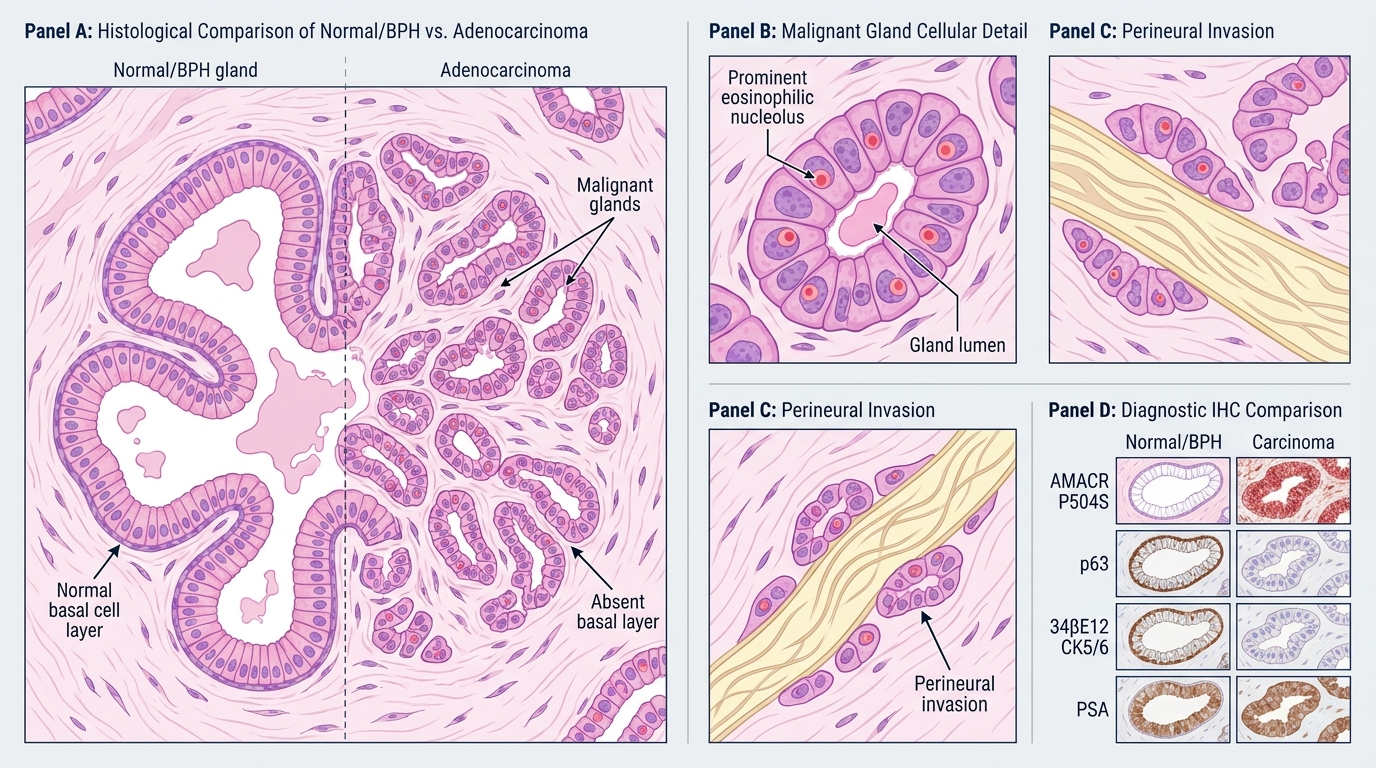
High-Power Histology of Prostatic Adenocarcinoma
Immunohistochemistry (IHC) panel for diagnosis:
| Marker | Normal/BPH | Carcinoma | Comment |
|---|---|---|---|
| AMACR (α-methylacyl-CoA racemase / P504S) | Negative | Positive | Most useful positive marker |
| p63 | Positive (basal cells) | Negative | Basal cell marker |
| 34βE12 (CK5/6) | Positive (basal cells) | Negative | Basal cell marker |
| PSA | Positive | Positive | Confirms prostatic origin, not specific for malignancy |