Page 9 of 21
PA28.3-5 | Prostate: BPH, Carcinoma & Prostatitis — SDL Guide (Part 4)
Gleason Grading and ISUP Grade Groups
The Gleason grading system is the most important prognostic tool in prostate pathology. It is based entirely on glandular architecture (not cytological features), assessing the degree of glandular differentiation and infiltration pattern.
Gleason patterns (1–5):
| Pattern | Architecture | Differentiation |
|---|---|---|
| 1 | Round, uniform, separate glands, packed but not infiltrating | Well differentiated |
| 2 | Loosely packed, slightly variable glands | Well differentiated |
| 3 | Discrete, individual infiltrating glands of variable size | Moderately differentiated — most common pattern |
| 4 | Fused, cribriform, or poorly formed glands | Poorly differentiated — key threshold |
| 5 | No gland formation — solid sheets, cords, single cells, comedonecrosis | Anaplastic |
Note: Patterns 1 and 2 are no longer assigned on needle biopsy by modern standards (2014 ISUP revision) — minimum reported is Pattern 3.
Gleason Score: Primary pattern (most prevalent) + Secondary pattern (second most prevalent) = Score (range 6–10 clinically used). E.g., 3+4=7 (most is pattern 3, some is pattern 4).
ISUP Grade Groups (2016 — 5 groups replacing the confusing 6–10 scale):
| ISUP Grade Group | Gleason Score | Prognosis |
|---|---|---|
| 1 | 3+3=6 | Excellent — many managed conservatively |
| 2 | 3+4=7 | Good |
| 3 | 4+3=7 | Intermediate — more pattern 4 = worse |
| 4 | 4+4=8; 3+5=8; 5+3=8 | Poor |
| 5 | 9–10 | Very poor |
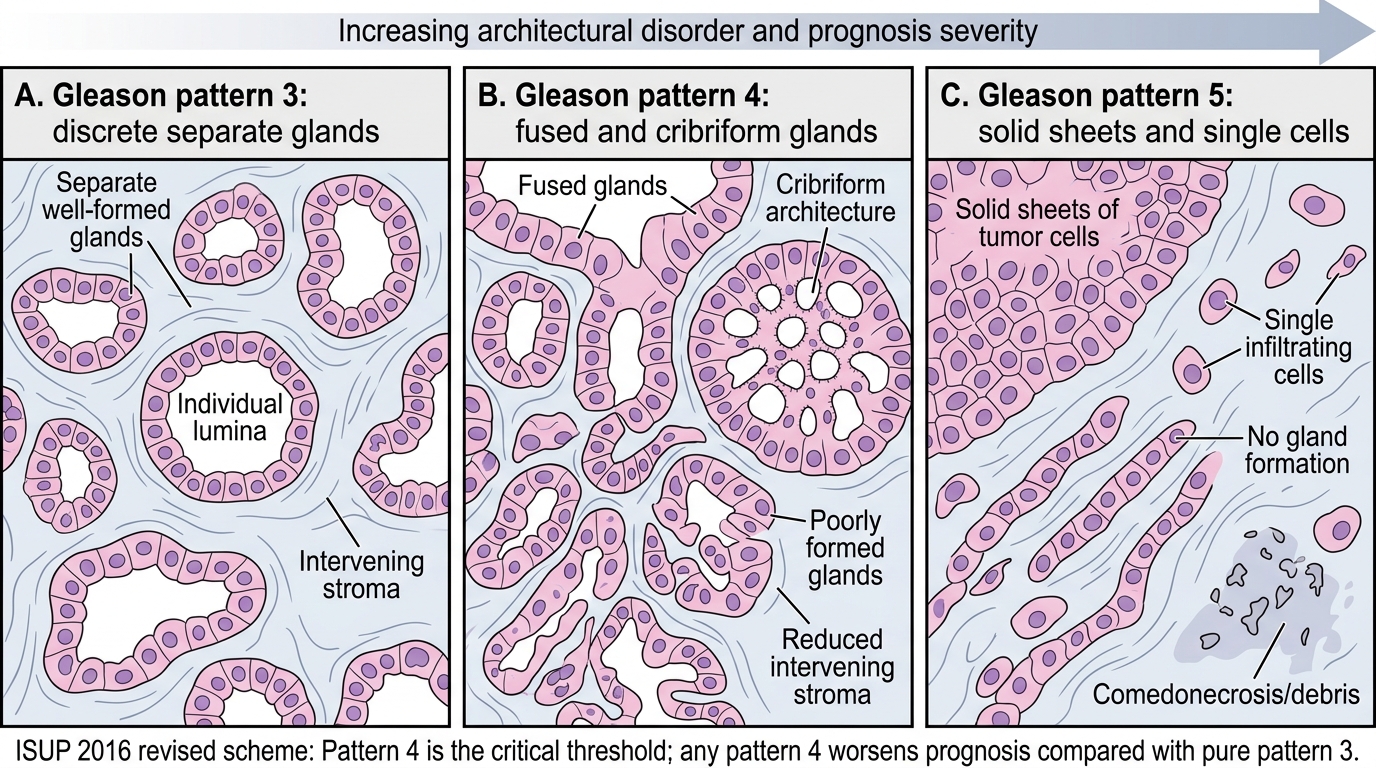
Gleason Patterns 3, 4, and 5 in Prostate Carcinoma
Clinical significance of the 3 vs 4 threshold:
Gleason pattern 4 is the critical inflection point — its presence (even as the minority pattern in a 3+4=7) significantly worsens prognosis compared to 3+3=6. This is why 3+4 (Grade Group 2) and 4+3 (Grade Group 3) are assigned different ISUP groups despite the same summed score.
Prostate Carcinoma: Staging and Routes of Spread
TNM/AJCC Staging (simplified):
| Stage | Definition |
|---|---|
| T1 | Clinically inapparent (not palpable) — T1a: ≤5% of TURP chips; T1b: >5%; T1c: needle biopsy (PSA-detected) |
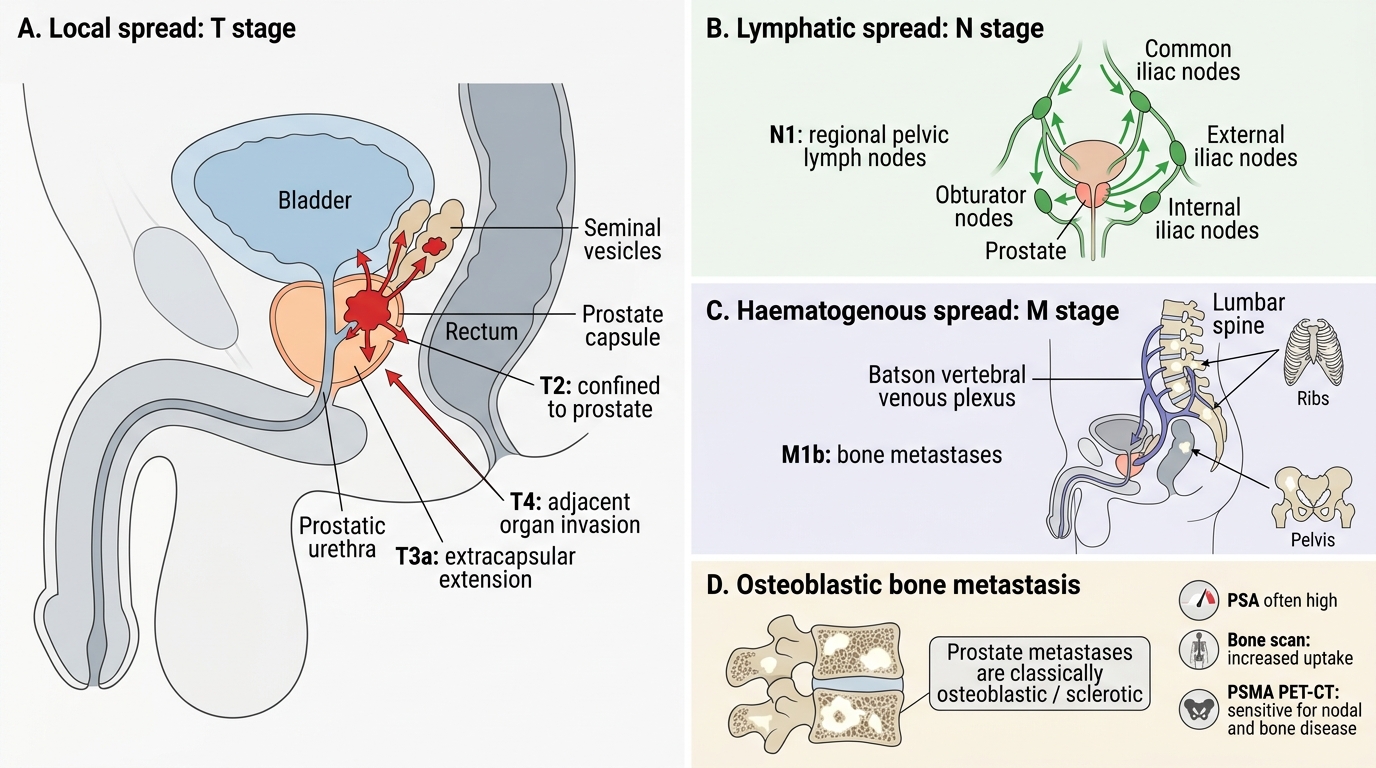
| T2 | Tumour confined within the prostate capsule |
| T3 | Extracapsular extension (T3a) or seminal vesicle invasion (T3b) |
| T4 | Invades adjacent structures: bladder neck, external sphincter, rectum, levator ani |
| N1 | Regional lymph node metastasis (obturator, internal iliac) |
| M1 | Distant metastasis — most commonly bone |
Routes of spread:
1. Direct extension (local spread):
• Extends through the prostatic capsule (extracapsular extension) — most commonly to the neurovascular bundles (posterolateral, explaining nerve-sparing surgery challenges and perineural invasion).
• Seminal vesicle invasion → upstages to T3b, worsens prognosis.
• Bladder base and trigone involvement → urinary symptoms.
• Rectal involvement (less common — Denonvilliers' fascia is a natural barrier).
- Lymphatic spread: Obturator lymph nodes → internal and external iliac nodes → para-aortic nodes. Lymph node metastasis indicates systemic disease.
3. Haematogenous spread — OSTEOBLASTIC BONE METASTASES:
The most distinctive feature of prostate cancer spread. Metastases to bone are predominantly osteoblastic (sclerotic) — tumour cells secrete endothelin-1 and other factors that stimulate osteoblasts → new bone formation → dense/sclerotic lesions on X-ray and bone scan (contrast with most other carcinoma metastases, which are osteolytic). Sites: vertebral column (lumbar > thoracic), pelvis, proximal femur, ribs, skull. The Batson vertebral venous plexus (valveless, communicates directly with pelvic veins) is the preferred route to the vertebral column. Bone pain (especially back/hip pain in an elderly man) + elevated PSA should immediately raise suspicion.
Routes of Spread in Prostate Cancer
- Distant haematogenous spread: Lung, liver (less common than bone).
Staging investigations:
• PSA: High PSA (>20 ng/mL) correlates with extracapsular extension or metastasis.
• Multiparametric MRI prostate (mpMRI): Best imaging for local staging — T2, DWI, DCE sequences; detects extracapsular extension, seminal vesicle invasion; PI-RADS score guides biopsy.
• Bone scan (Tc-99m): Detects osteoblastic metastases — indicated when PSA >20, Gleason score ≥8, or T3/T4 disease.
• PSMA PET-CT: Increasingly replacing bone scan — more sensitive for nodal and bone disease; detects recurrence earlier.
SELF-CHECK
A 72-year-old man presents with severe low back pain for 3 months. PSA is 85 ng/mL. Bone scan shows multiple areas of increased uptake in the lumbar spine, pelvis, and ribs. Plain X-ray of the lumbar spine shows dense, sclerotic vertebral lesions. Biopsy of a vertebra confirms metastatic adenocarcinoma. What is the most likely PRIMARY site?
A. Lung — squamous cell carcinoma metastases can be osteoblastic
B. Kidney — renal cell carcinoma commonly metastasises to bone
C. Prostate — osteoblastic bone metastases with elevated PSA are characteristic
D. Breast — breast cancer is the most common cause of osteoblastic metastases
Reveal Answer
Answer: C. Prostate — osteoblastic bone metastases with elevated PSA are characteristic
Osteoblastic (sclerotic) bone metastases + markedly elevated PSA in an elderly man is the classic presentation of metastatic prostate adenocarcinoma. Prostate cancer secretes endothelin-1 and other factors that stimulate osteoblasts, producing dense sclerotic lesions — the opposite of the osteolytic punched-out lesions seen in myeloma, renal cell carcinoma, and most other carcinomas. Breast cancer can also produce osteoblastic metastases, but PSA elevation points specifically to prostatic origin. Lung squamous cell carcinoma is almost always osteolytic.
PSA Screening, Diagnosis, Treatment, and Prognosis
PSA (Prostate-Specific Antigen):
PSA is a serine protease (encoded by KLK3 gene) secreted by prostatic epithelium — its normal function is to liquefy seminal coagulum. Serum PSA is elevated whenever the epithelial-stromal barrier is disrupted.
Reference ranges (approximate):
• <4 ng/mL — traditionally 'normal' (but ~15% of cancers are PSA <4)
• 4–10 ng/mL — 'grey zone' (25% probability of cancer)
• >10 ng/mL — high suspicion (>50% probability of cancer)
• PSA density (PSA/prostate volume) >0.15 ng/mL/cc favours cancer
• PSA velocity (rise >0.75 ng/mL/year) — suspicious even within grey zone
• Free:total PSA ratio — lower free PSA fraction (<25%) suggests carcinoma (BPH elevates both total and free PSA proportionately)
Screening controversy: Widespread PSA screening reduces cancer-specific mortality (~20% in ERSPC trial) but causes significant overdiagnosis (many indolent tumours that would never cause symptoms are detected and treated) → shared decision-making approach now recommended (USPSTF); most guidelines recommend starting discussion at age 50–55 for average-risk men.
Diagnosis: TRUS-guided needle biopsy (12-core systematic) or MRI-targeted biopsy (for PI-RADS 3–5 lesions). Minimum 10–12 cores from the peripheral zone bilaterally.
Treatment principles:
| Stage | Options |
|---|---|
| Localised (T1-T2, low grade) | Active surveillance; radical prostatectomy; external beam radiotherapy ± brachytherapy |
| Locally advanced (T3-T4) | Radiotherapy + ADT (androgen deprivation therapy) |
| Metastatic | Androgen deprivation therapy (ADT) — surgical (bilateral orchidectomy) or medical (LHRH agonists/antagonists: leuprolide, goserelin, degarelix) |
| Castration-resistant | Enzalutamide/abiraterone (next-gen AR axis inhibitors); docetaxel chemotherapy; PARP inhibitors (if BRCA2 mutation) |
Androgen deprivation therapy (ADT) works because prostate cancer cells are androgen-dependent — removing androgens causes apoptosis and tumour regression. Eventually, cancer cells mutate to become castration-resistant (AR amplification, mutations, splice variants like AR-V7) — a clinically important endpoint.
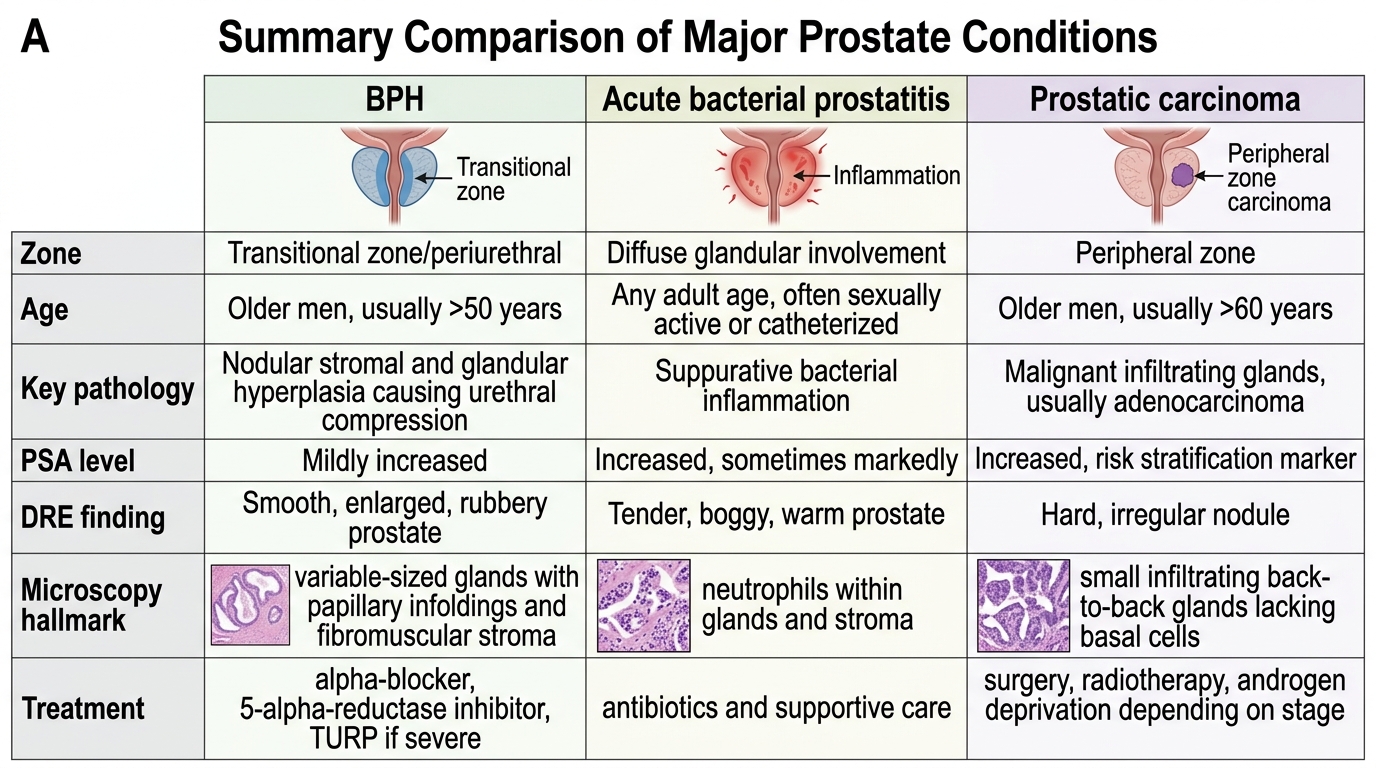
Comparison of BPH, Acute Prostatitis, and Prostatic Carcinoma
Prognosis:
• ISUP Grade Group 1 (Gleason 3+3=6) with PSA <10 and T1c: 10-year cancer-specific survival >95%.
• Metastatic castration-sensitive: median survival ~3–5 years with modern combination therapy.
• Castration-resistant: median survival ~18–36 months depending on treatment era.
> Key prognostic triad: PSA level + Gleason grade + clinical stage — used together to risk-stratify every newly diagnosed prostate cancer patient.
CLINICAL PEARL
Osteoblastic metastases cause a 'superscan' on bone scan. When prostate cancer metastases are extensive, the bone scan may show such diffuse, intense uptake throughout the axial and appendicular skeleton that the kidneys (normally visible) are not seen — the image looks like only bone, hence 'superscan.' Paradoxically, it can be mistaken for a technically inadequate scan. Recognising a superscan in the context of an elevated PSA is a critical clinical and exam skill. Serum alkaline phosphatase (ALP) is also markedly elevated because osteoblasts produce ALP — a cheap and useful surrogate for bone turnover in monitoring treatment response.
SELF-CHECK
A pathologist receives a needle biopsy from the right peripheral zone of a 67-year-old man. H&E shows small infiltrating glands with a single cell layer, absent basal cells, and prominent eosinophilic nucleoli. Immunohistochemistry for AMACR (P504S) is strongly positive; p63 and 34βE12 are both negative. What is the diagnosis?
A. High-grade prostatic intraepithelial neoplasia (HGPIN)
B. Benign prostatic hyperplasia
C. Prostatic adenocarcinoma
D. Granulomatous prostatitis
Reveal Answer
Answer: C. Prostatic adenocarcinoma
The combination of (1) small infiltrating glands, (2) absent basal cell layer on H&E, (3) positive AMACR (a positive marker for malignancy in prostate), and (4) negative p63/34βE12 (basal cell markers — confirming absence of basal layer) is the classic IHC profile of prostatic adenocarcinoma. HGPIN retains an intact (though patchy) basal layer and basal cell markers remain positive; it can be AMACR-weakly positive but glandular architecture is preserved. BPH has intact two-layer epithelium with basal cells positive for p63/34βE12 and AMACR negative.