Page 1 of 21
PA28.1 | Testicular Tumors — SDL Guide
Learning Objectives
- Classify testicular tumors into germ cell tumors (seminoma and non-seminomatous), sex cord-stromal tumors, and lymphoma, and explain the basis of this classification.
- Describe the pathogenesis of germ cell tumors, including the roles of isochromosome 12p and germ cell neoplasia in situ (GCNIS).
- Outline the gross and microscopic morphology of seminoma, embryonal carcinoma, yolk sac tumor, choriocarcinoma, teratoma, and mixed germ cell tumors.
- Correlate each tumor type with its characteristic serum tumor markers (AFP, β-hCG, LDH) and explain why AFP is never elevated in pure seminoma.
- Describe the typical clinical presentation, routes of lymphatic and hematogenous spread, staging system, and principles of management for testicular germ cell tumors.
INSTRUCTIONS
Testicular tumors are among the most common solid malignancies in young men aged 15–35 years, yet they carry some of the best cure rates in oncology when diagnosed and treated appropriately. This SDL integrates histopathology, molecular biology, clinical reasoning, and tumor marker interpretation into a unified framework. As you work through each section, connect the microscopic appearance to the tumor's behaviour — for example, why choriocarcinoma bleeds so readily, or why pure seminoma is AFP-negative. Build your classification tree systematically before memorising individual features, and use the micro-quizzes to test pattern recognition. This module forms the foundation for understanding male genital tract pathology and is directly examinable in clinical and pre-clinical assessments under NMC competency PA28.1.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 21 — Male Genital Tract (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch. 24 — Male Reproductive System (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old medical student notices a painless, hard swelling in his right testis while showering. He dismisses it as a minor injury and delays seeking care for six weeks. When he finally presents to a urologist, his serum β-hCG is markedly elevated and a chest X-ray reveals pulmonary nodules. The urologist tells him that had he come two weeks earlier, the staging would likely have been Stage I — now it is Stage III. The diagnosis: mixed germ cell tumor, predominantly choriocarcinoma. This case encapsulates why recognising a painless testicular mass in a young man as cancer-until-proven-otherwise is one of the most critical clinical reflexes you will develop. Delay is the enemy.
WHY THIS MATTERS
Testicular tumors account for ~1–2% of all male malignancies but are the most common solid cancer in men aged 15–35 years. Despite this, overall survival exceeds 95% for Stage I disease and 70–80% even for metastatic disease — a triumph of cisplatin-based chemotherapy (BEP regimen). For the clinician, the challenge is early recognition: the differential diagnosis of a scrotal swelling includes epididymo-orchitis, hydrocele, and varicocele, but a solid, painless intratesticular mass demands urgent investigation. Pathologists play a central role in diagnosing tumor type from the orchiectomy specimen, which directly guides oncological management. Understanding the tumor marker profile, histological subtype, and staging is therefore essential to patient care.
RECALL
Before proceeding, activate the following Year-1 knowledge:
- Anatomy: The testis descends retroperitoneally from the lumbar region. Its lymphatic drainage follows the gonadal vessels to the para-aortic (retroperitoneal) lymph nodes at L1–L2 — NOT the inguinal nodes (which drain the scrotum). This explains the typical first site of metastasis in testicular GCTs.
- Histology: The testis contains two main cell populations — germ cells (spermatogonia → mature sperm) within seminiferous tubules, and supporting stromal cells (Sertoli cells inside tubules; Leydig cells in the interstitium). Tumors arise from each of these lineages.
- Biochemistry: α-Fetoprotein (AFP) is a fetal liver protein that also marks yolk sac (hepatoid) differentiation. β-hCG is produced by syncytiotrophoblasts (placental cells). Elevated levels in a non-pregnant male indicate tumor production. LDH (lactate dehydrogenase) is a non-specific marker of tumor bulk and cell turnover.
- Embryology: The testis develops from an undifferentiated gonad near the mesonephric (Wolffian) duct. Failure of normal descent leads to cryptorchidism, the strongest known risk factor for testicular GCT.
Classification of Testicular Tumors
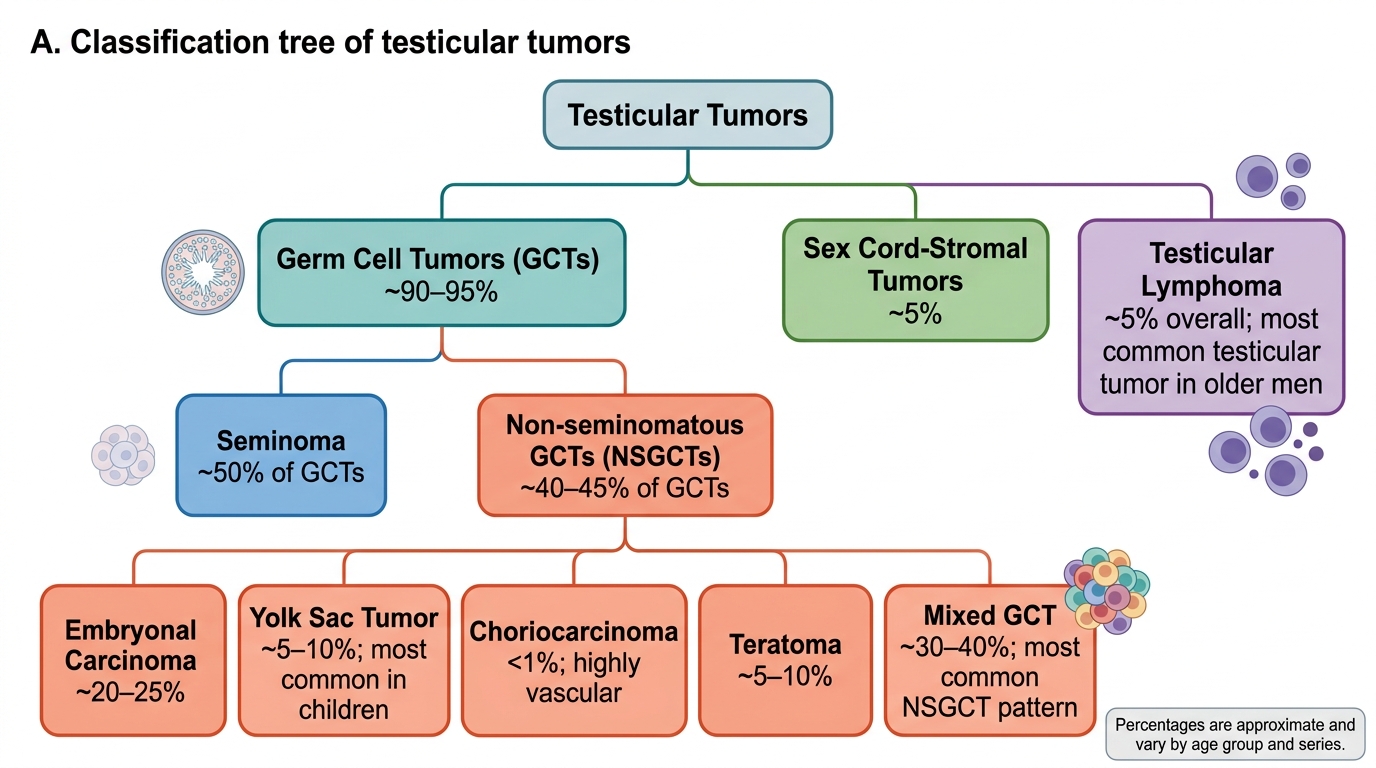
The WHO classification divides testicular tumors into three broad categories based on cell of origin:
| Category | Cell of Origin | Key Examples | Age Group |
|---|---|---|---|
| Germ cell tumors (GCTs) | Pluripotent germ cells | Seminoma, embryonal carcinoma, yolk sac tumor, choriocarcinoma, teratoma, mixed GCT | 15–45 years |
| Sex cord-stromal tumors | Sertoli or Leydig cells | Leydig cell tumor, Sertoli cell tumor | Any age |
| Lymphoma | B lymphocytes | Diffuse large B-cell lymphoma | >60 years |
Germ cell tumors (GCTs) constitute ~95% of testicular neoplasms. They are further divided into:
1. Seminoma (~55% of GCTs) — resembles primitive germ cells; uniform cells; AFP-negative; highly radiosensitive.
2. Non-seminomatous germ cell tumors (NSGCTs) — umbrella term for all other GCTs:
- Embryonal carcinoma — most aggressive; resembles early embryonic cells
- Yolk sac tumor (endodermal sinus tumor) — most common in infants; AFP-positive
- Choriocarcinoma — resembles placental trophoblasts; β-hCG-positive; prone to hemorrhage
- Teratoma — contains elements from two or three germ layers; mature teratoma in adults is NOT benign (unlike in females)
- Mixed GCT — two or more histological patterns; most common NSGCT overall (~50% of NSGCTs)
The critical clinical implication: seminoma vs. NSGCT drives treatment — seminomas are exquisitely radiosensitive, while NSGCTs require cisplatin-based chemotherapy.
Classification of Testicular Tumors
Risk Factors and Pathogenesis
Risk Factors
- Cryptorchidism (undescended testis): 3–5-fold increased GCT risk in the undescended testis and 2-fold in the contralateral normally descended testis. Even after successful orchiopexy before puberty, residual risk persists — suggesting that cryptorchidism is a marker of testicular dysgenesis, not just a mechanical problem.
- Testicular dysgenesis syndrome (TDS): A spectrum including cryptorchidism, hypospadias, impaired spermatogenesis, and GCT, linked to fetal exposure to endocrine disruptors.
- Klinefelter syndrome (47,XXY): Increased risk of mediastinal GCTs and bilateral testicular GCTs.
- Prior contralateral GCT: 2–3% lifetime risk of a second primary in the opposite testis.
- Family history: ~8–10-fold risk in first-degree relatives.
Pathogenesis — the two-hit model
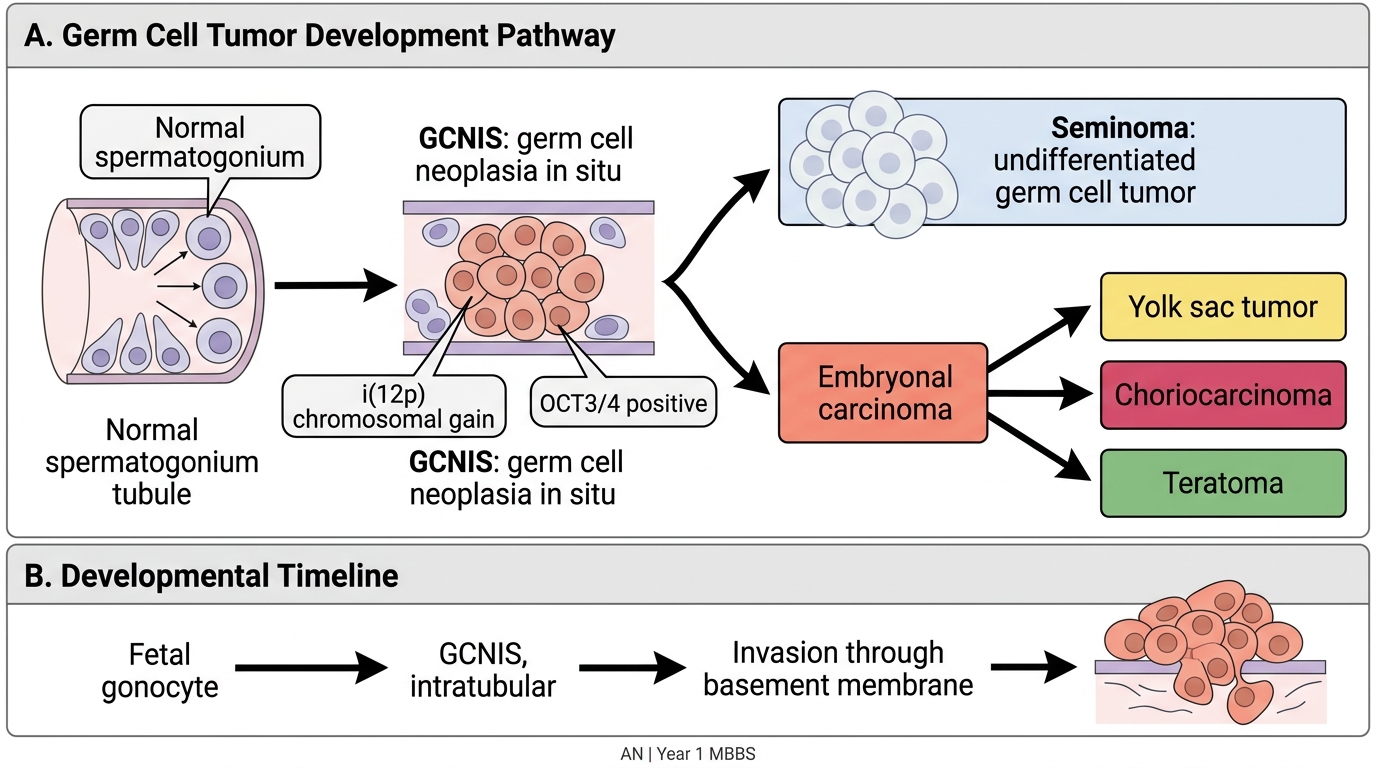
All testicular GCTs (except spermatocytic tumor) are now believed to arise from a common precursor lesion:
Germ cell neoplasia in situ (GCNIS) — formerly called intratubular germ cell neoplasia (IGCN) — consists of atypical large cells with clear cytoplasm resembling embryonic gonocytes, lining the seminiferous tubules without invasion. GCNIS has two key features:
- It expresses OCT3/4 (POU5F1) and PLAP (placental alkaline phosphatase) — markers of embryonic/pluripotent stem cells.
- It invariably harbors isochromosome 12p (i[12p]) — the hallmark genomic alteration of testicular GCTs.
Isochromosome 12p arises from an error during meiosis — the short arm (12p) is duplicated and the long arm (12q) lost, creating a chromosome with two identical 12p arms. The 12p region contains genes (KRAS, CCND2, NANOG, DAD-R) that promote cell survival and pluripotency. This gain-of-function alteration is present in ~80% of GCTs and drives progression from GCNIS to invasive tumor.
The lineage taken by the invasive GCT determines its histological type:
- Undifferentiated → seminoma
- Totipotent (embryonic) → embryonal carcinoma → further differentiation to yolk sac tumor (extraembryonic endoderm), choriocarcinoma (trophoblast), or teratoma (somatic tissues)
Pathogenesis of Testicular Germ Cell Tumors
Seminoma — Morphology and Behaviour
Seminoma is the most common single testicular GCT and the paradigm of a radiosensitive, highly curable tumor.
Gross morphology: Homogeneous, lobulated, creamy-white to grey cut surface without hemorrhage or necrosis (unless very large). The tumor is well-circumscribed and typically replaces most of the testis. The tunica albuginea (fibrous capsule) is intact in most cases.
Microscopic morphology (the hallmark pattern):
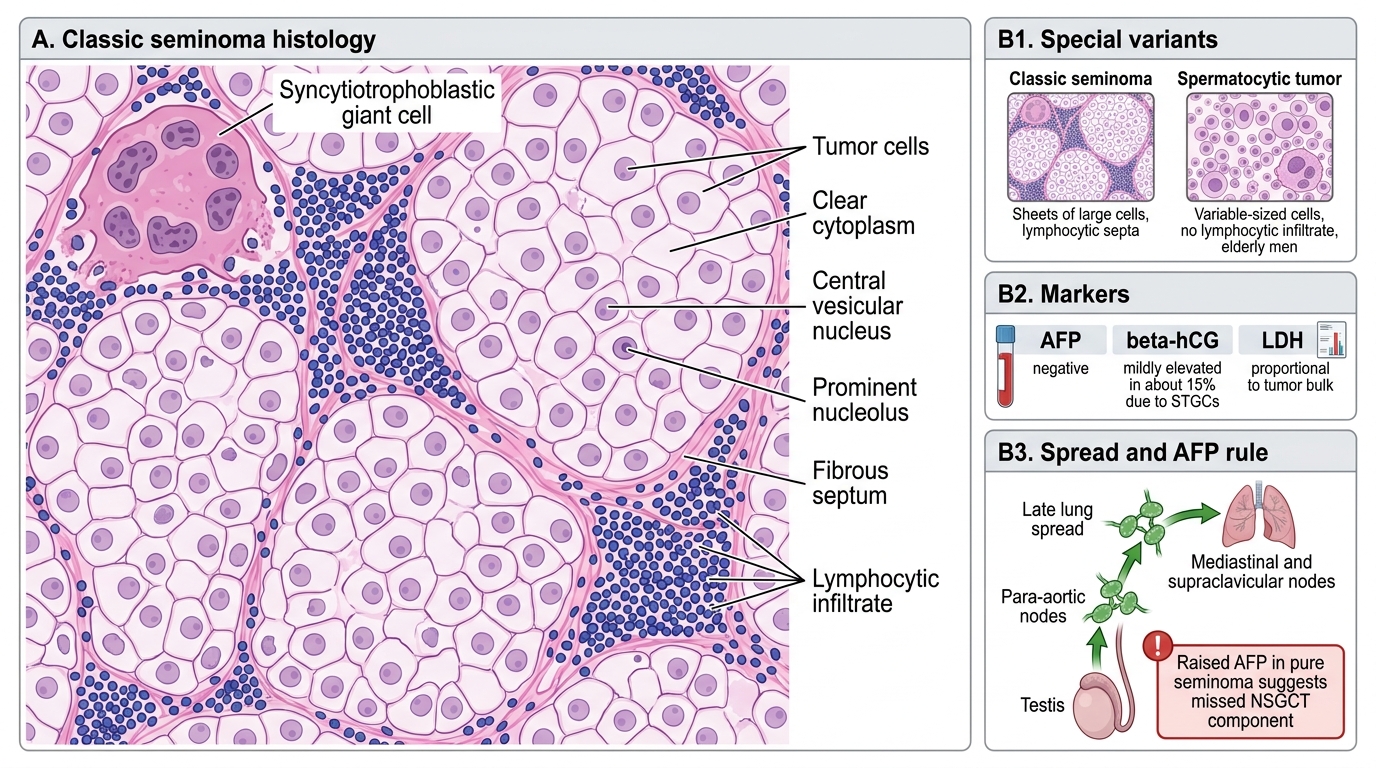
- Sheets and lobules of uniform large round cells — each with abundant clear cytoplasm (glycogen-rich, PAS-positive), a large central nucleus with prominent nucleolus.
- Stroma contains fibrous septa with a characteristic lymphocytic infiltrate — this lymphocytic response is pathognomonic and reflects host immunosurveillance.
- Granulomatous reaction (aggregates of epithelioid histiocytes) in ~20% of cases — can mimic tuberculosis on clinical presentation.
- Syncytiotrophoblastic giant cells (STGCs) in ~15% of classic seminomas — these produce β-hCG, but AFP remains negative (this is critical: pure seminoma is ALWAYS AFP-negative).
Classic Seminoma: Histology, Markers, and Clinical Pearl
Special variants:
- Classic (typical) seminoma: 95% of seminomas; age 30–40 years.
- Spermatocytic tumor (formerly spermatocytic seminoma): elderly men (>50 years); NOT related to GCNIS or i(12p); lacks lymphocytic infiltrate; extremely indolent — rarely metastasises.
Markers: AFP — negative (always); β-hCG — mildly elevated in ~15% (due to STGCs); LDH — elevated proportional to tumor bulk.
Behaviour: Spreads first to para-aortic lymph nodes, then to mediastinal/supraclavicular nodes, and late to lungs. Hematogenous spread is uncommon. Highly sensitive to radiotherapy and cisplatin.
CLINICAL PEARL
AFP rule for seminoma: If a patient has a histologically pure seminoma on orchiectomy AND a raised AFP — the pathologist has missed a yolk sac tumor or embryonal carcinoma component. The AFP drives you to look harder. In practice, a raised AFP after orchiectomy reclassifies the tumor as NSGCT regardless of histology, and management changes accordingly. This is one of the most high-yield exam facts in testicular tumor pathology.