Page 2 of 21
PA28.1 | Testicular Tumors — SDL Guide (Part 2)
Non-Seminomatous GCTs — Embryonal Carcinoma and Yolk Sac Tumor
Embryonal Carcinoma
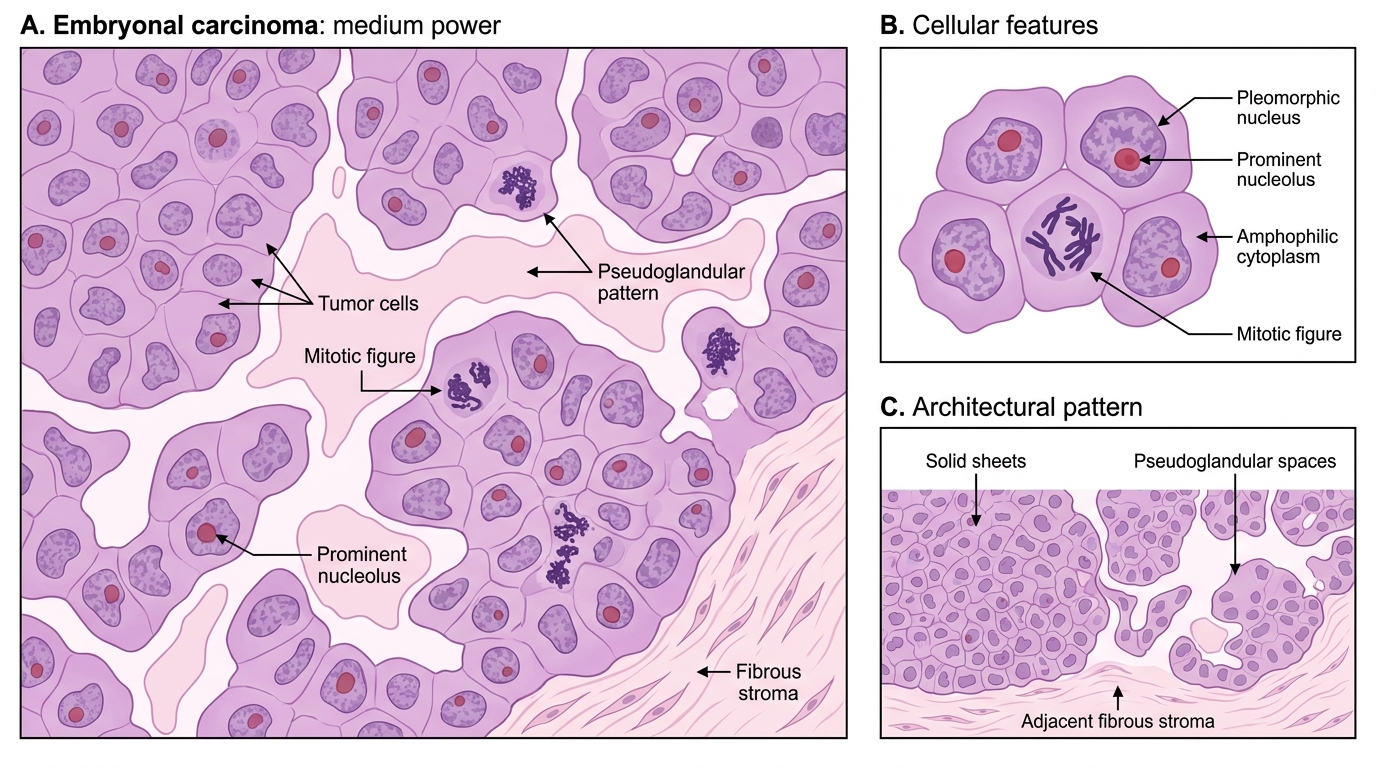
Embryonal carcinoma is the most aggressive and undifferentiated NSGCT, histologically resembling cells of the early embryo (inner cell mass).
Gross: Small, poorly circumscribed, variegated cut surface with prominent hemorrhage and necrosis — contrasting with the homogeneous seminoma.
Microscopic: Large pleomorphic cells arranged in solid sheets, acini (gland-like spaces), or papillae. Cells have amphophilic (dark) cytoplasm, indistinct borders, large irregular nuclei with prominent nucleoli, and numerous mitoses. The "messy" architecture distinguishes it from the orderly seminoma.
Markers: AFP ± elevated; β-hCG ± elevated (STGCs may be present); OCT3/4 positive.
Histology of Embryonal Carcinoma
Yolk Sac Tumor (Endodermal Sinus Tumor)
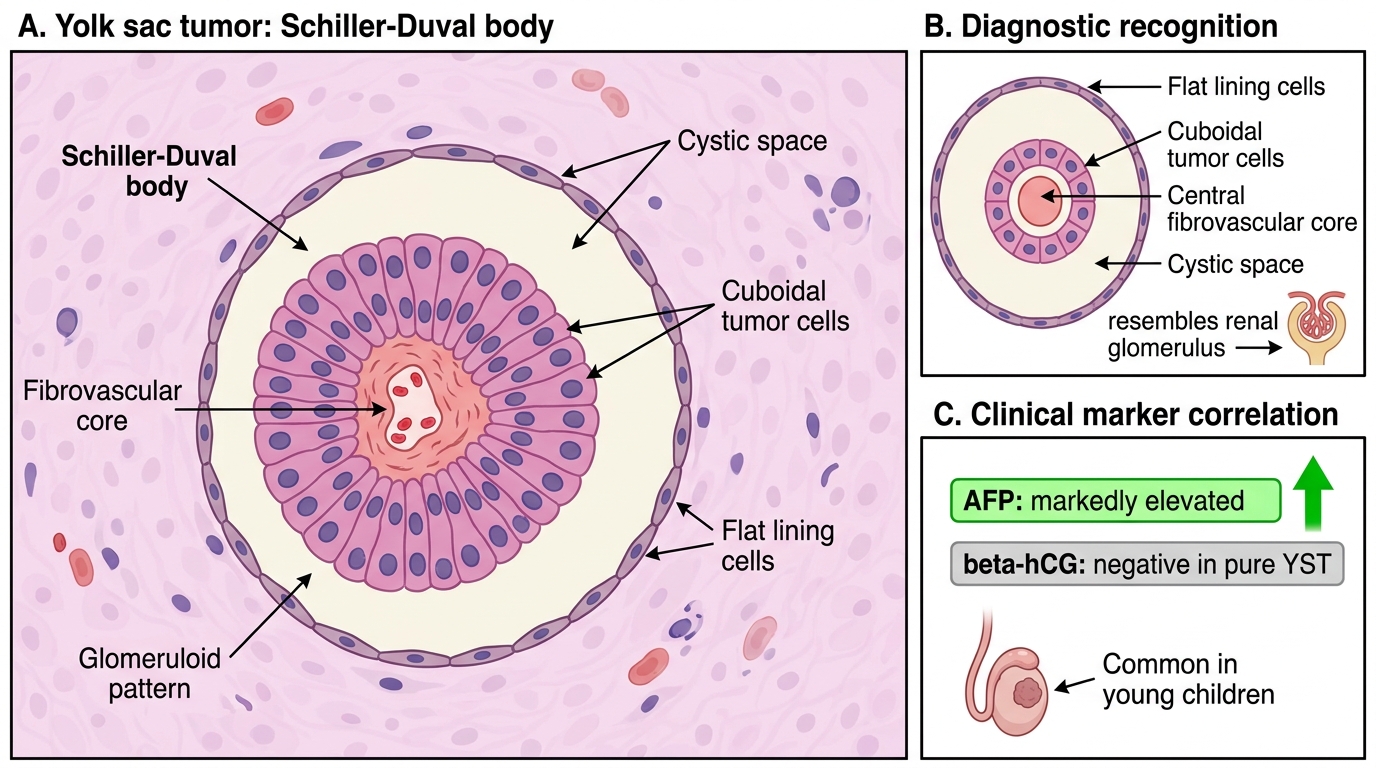
Yolk sac tumor (YST) recapitulates the yolk sac (extraembryonic endoderm) and is the most common testicular GCT in children under 3 years (pure form). In adults, it almost always occurs as a component of a mixed GCT.
Gross: Mucoid, gelatinous cut surface; yellow-white; may show cysts.
Microscopic: Multiple patterns possible, but the Schiller-Duval body is pathognomonic — a central fibrovascular core lined by tumor cells within a cystic space, mimicking the glomeruloid structure of the primitive yolk sac. Cells are cuboidal with vacuolated cytoplasm. Intracellular and extracellular hyaline globules that are AFP-positive on immunohistochemistry are characteristic.
Schiller-Duval Body in Yolk Sac Tumor
Markers: AFP — markedly elevated (the most specific marker for YST); β-hCG — negative in pure YST.
Behaviour (children): Highly curable with surgery ± chemotherapy, even if AFP initially elevated.
SELF-CHECK
A 2-year-old boy is brought with a painless right testicular mass. Orchiectomy shows a tumor with Schiller-Duval bodies and intracytoplasmic hyaline globules. Which serum tumor marker is MOST likely to be markedly elevated?
A. A. β-hCG
B. B. AFP (α-fetoprotein)
C. C. LDH
D. D. Testosterone
Reveal Answer
Answer: B. B. AFP (α-fetoprotein)
Yolk sac tumor (endodermal sinus tumor) — the most common testicular tumor in young children — produces AFP as it recapitulates yolk sac (hepatoid) differentiation. Schiller-Duval bodies are the pathognomonic histological feature. AFP is markedly elevated; β-hCG is not a feature of pure YST. LDH is non-specific and reflects bulk, not a specific marker for YST. Testosterone elevation is a feature of Leydig cell tumors.
Choriocarcinoma and Teratoma
Choriocarcinoma
Choriocarcinoma recapitulates placental trophoblast and is the most aggressive testicular GCT. Pure choriocarcinoma is rare (~0.3% of GCTs) but choriocarcinoma elements are common in mixed GCTs.
Gross: Characteristically small primary tumor with massive systemic metastases — the retroperitoneal nodes may be unaffected while pulmonary, hepatic, and brain metastases are already present. The cut surface shows hemorrhage and necrosis (trophoblast invades vessels).
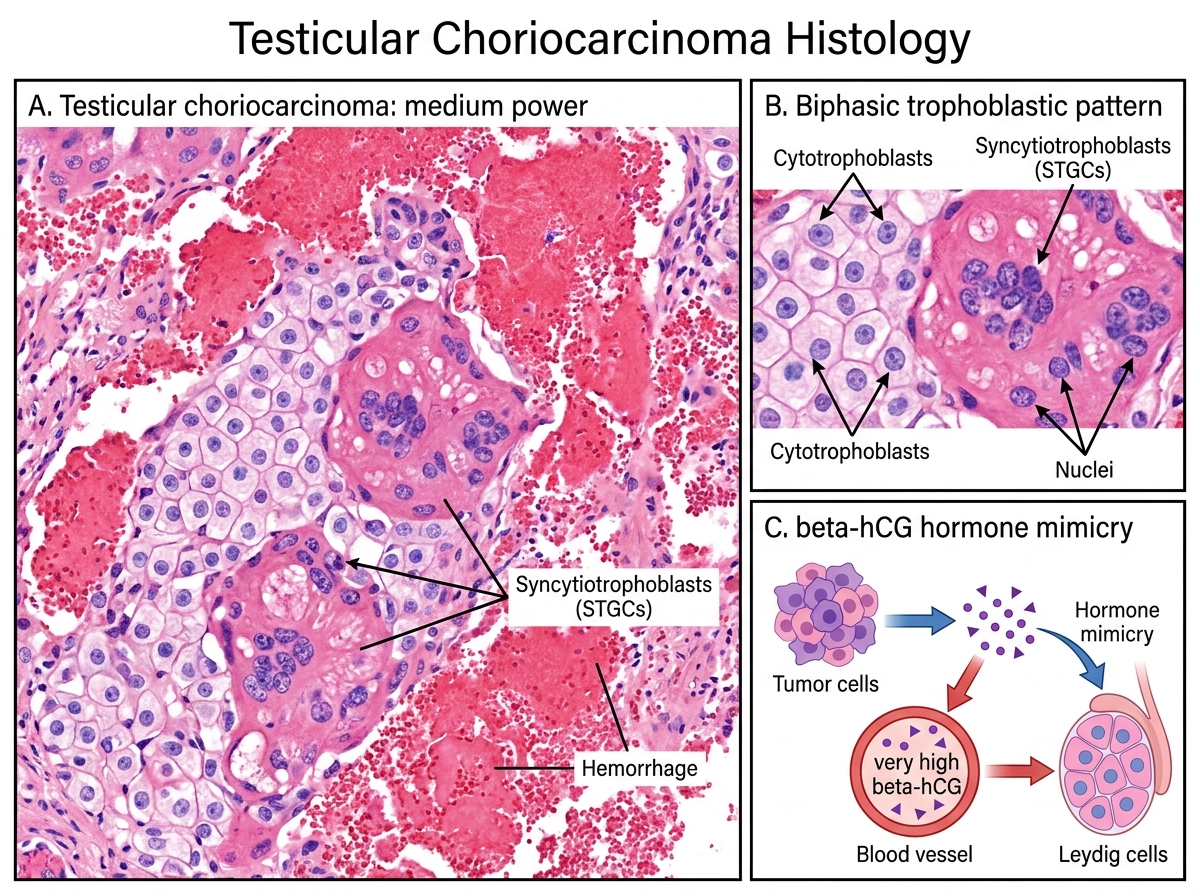
Microscopic: Biphasic pattern — the defining requirement:
- Cytotrophoblasts: Mononuclear cells with clear cytoplasm and distinct cell membranes
- Syncytiotrophoblasts (STGCs): Large multinucleated cells with abundant eosinophilic vacuolated cytoplasm — these produce β-hCG
Both components must be present for the diagnosis; STGCs alone do not make choriocarcinoma.
Markers: β-hCG — markedly elevated (very high levels correlate with prognosis); AFP negative in pure choriocarcinoma.
Behaviour: Hematogenous spread occurs very early (even with microscopic primary) — to lungs, liver, brain. This is why choriocarcinoma presents with distant metastases despite a small primary. Prognosis is worse than other GCT subtypes.
Testicular Choriocarcinoma: Biphasic Histology
Teratoma
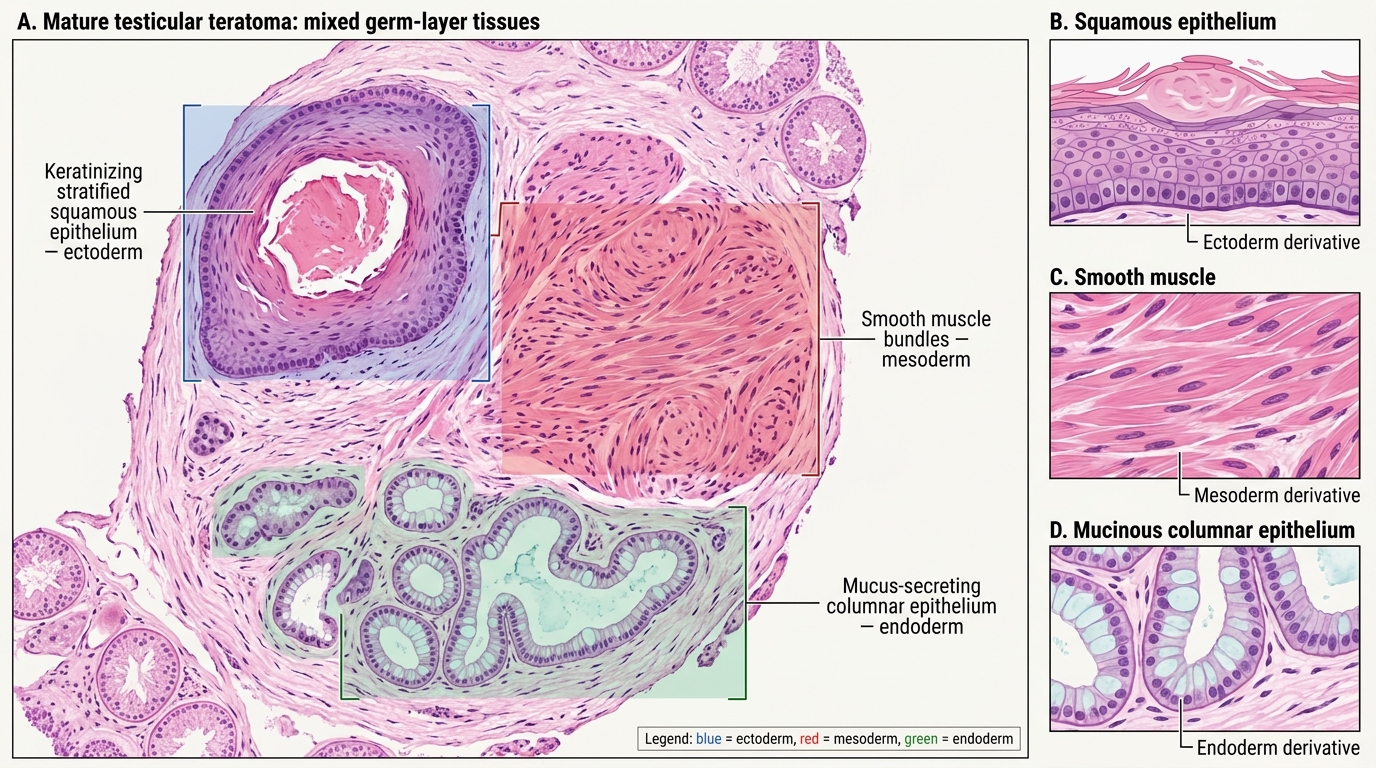
Teratoma contains mature or immature tissues from two or three germ layers (ectoderm, mesoderm, endoderm).
Gross: Heterogeneous — cysts containing mucus, hair, keratin; solid areas of cartilage, bone, neural tissue.
Microscopic: Tissues of varying differentiation — squamous epithelium (ectoderm), smooth muscle, cartilage, bone (mesoderm), intestinal-type mucous glands (endoderm). Mature teratoma in adults is NOT benign (unlike ovarian mature teratoma in females) — it can metastasise. The retained i(12p) alteration distinguishes adult testicular teratoma from the truly benign prepubertal form.
Markers: In a pure teratoma, AFP and β-hCG may be slightly elevated if there are minor components of other lineages; generally not a marker-secreting tumor.
Mature Testicular Teratoma: Three Germ-Layer Derivatives
CLINICAL PEARL
Choriocarcinoma and 'hormone mimicry': Because choriocarcinoma produces very high β-hCG, it can stimulate Leydig cells via cross-reactivity with LH receptors, causing gynecomastia (breast enlargement in males). A young man with a testicular mass + gynecomastia should raise the suspicion for choriocarcinoma or a β-hCG-secreting mixed GCT. Similarly, hyperthyroidism can occur (β-hCG cross-reacts with TSH receptors at very high levels). Don't mistake gynecomastia for a Leydig cell tumor without checking β-hCG first.
Mixed GCTs, Sex Cord-Stromal Tumors, and Lymphoma
Mixed Germ Cell Tumors
Mixed GCTs contain two or more histological components and constitute approximately 50% of all NSGCTs. The most common combination is embryonal carcinoma + teratoma (teratocarcinoma). The clinical behavior is governed by the most aggressive component present.
Key rule: The final tumor marker profile and staging reflect ALL components — a mixed GCT with any choriocarcinoma element will have markedly elevated β-hCG; one with yolk sac tumor will have elevated AFP.
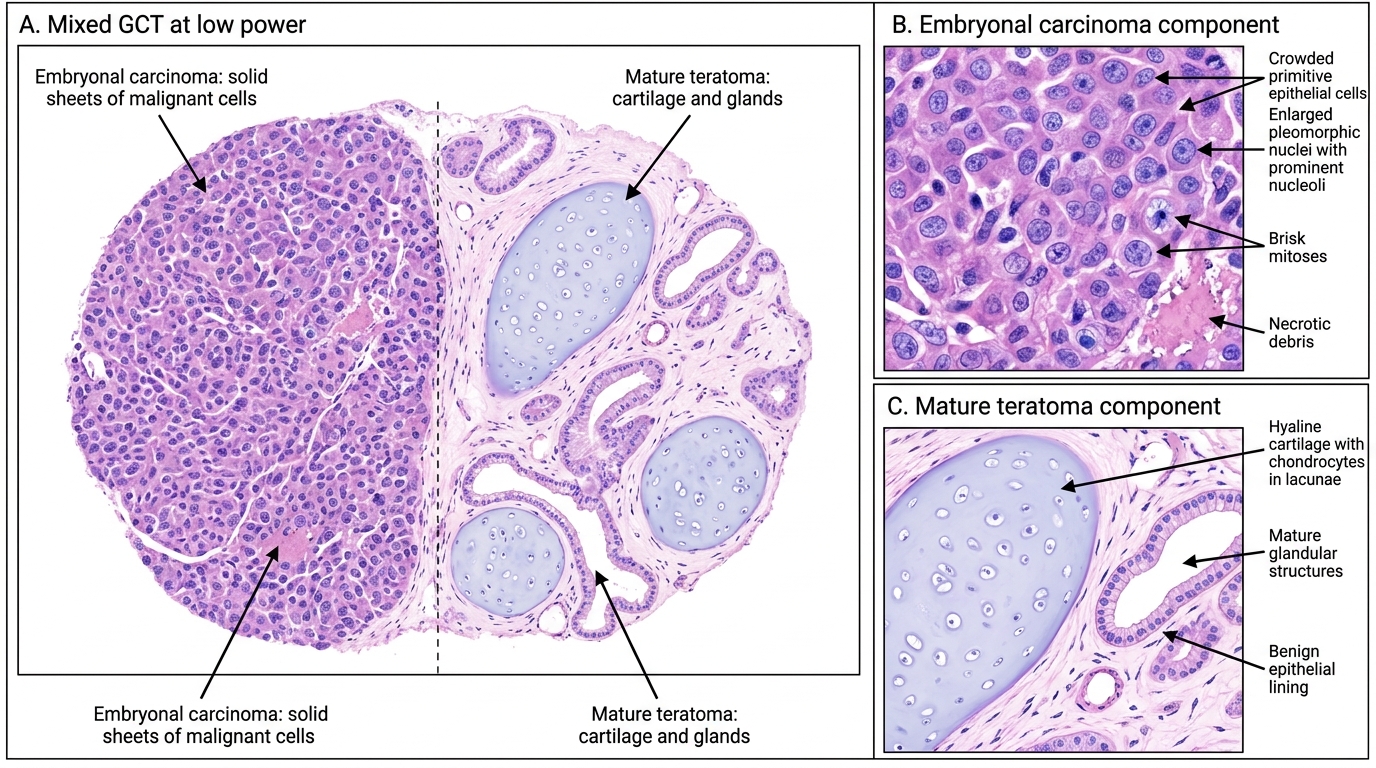
Mixed Germ Cell Tumor: Embryonal Carcinoma and Mature Teratoma
Sex Cord-Stromal Tumors (~5% of testicular tumors)
Leydig cell tumor: Most common sex cord-stromal tumor. The Leydig cell is the testosterone-producing interstitial cell.
- Clinical: Precocious puberty in boys (excess testosterone); gynecomastia in adults (peripheral conversion of excess androgen to estrogen, or direct estrogen production).
- Gross: Well-circumscribed, golden-brown (lipid-rich) nodule.
- Microscopic: Large polygonal cells with abundant eosinophilic granular cytoplasm and round nuclei. Pathognomonic feature: Reinke crystalloids — rectangular eosinophilic rod-shaped cytoplasmic inclusions (seen in ~25–40%).
- Behaviour: ~90% benign. Malignant in ~10% — diagnosed by metastasis, not histology alone.
Sertoli cell tumor: Rare; tubular architecture; may produce estrogen → gynecomastia.
Lymphoma (~5% of testicular tumors)
Testicular lymphoma is the most common testicular tumor in men >60 years. Most are diffuse large B-cell lymphomas (DLBCL). Bilateral involvement occurs in 20–38% of cases (unlike GCTs which are very rarely bilateral). Associated with systemic dissemination; prognosis is poorer than primary nodal DLBCL.