Page 3 of 21
PA28.1 | Testicular Tumors — SDL Guide (Part 3)
Tumor Markers — AFP, β-hCG, and LDH
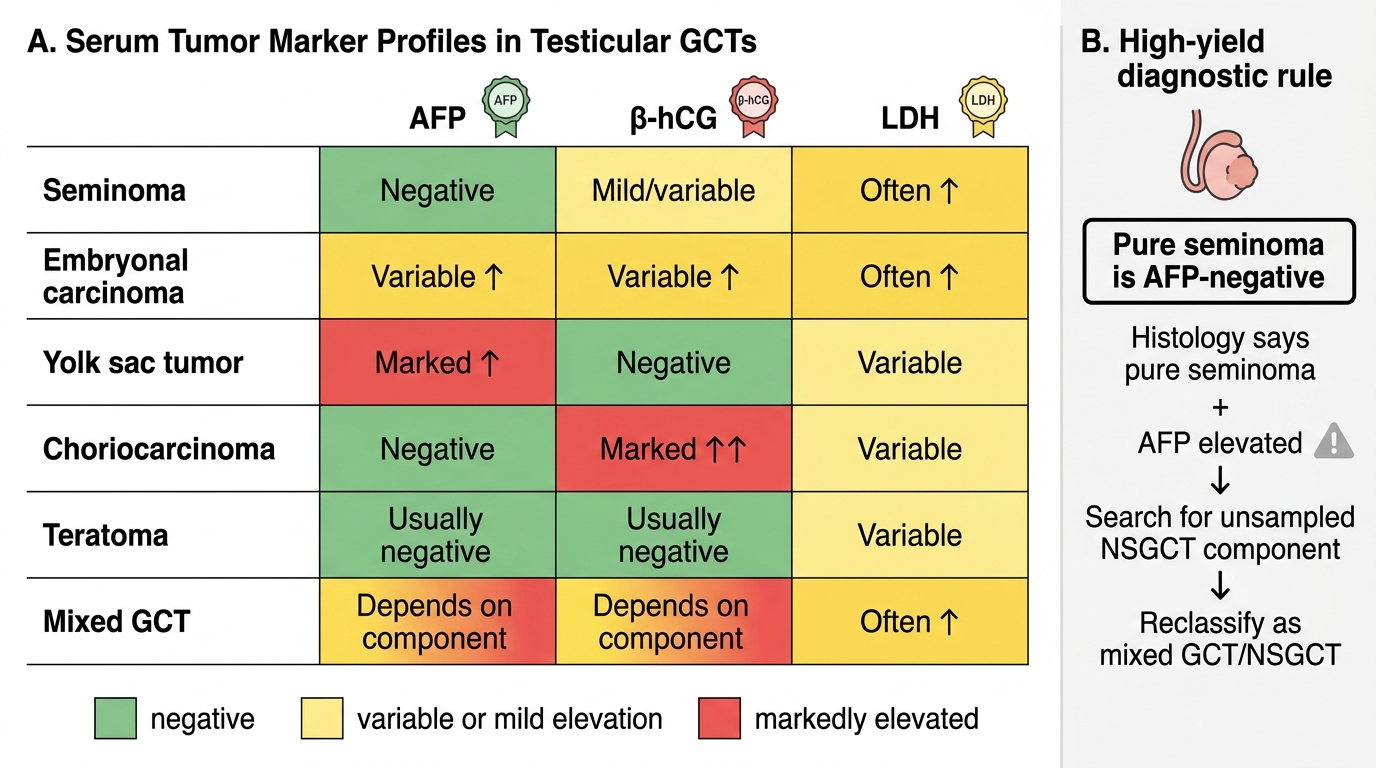
Serum tumor markers are central to diagnosis, staging, prognosis, and monitoring response to treatment in testicular GCTs. The three standard markers are:
| Marker | Produced by | Elevated in | NOT elevated in |
|---|---|---|---|
| AFP | Yolk sac endodermal cells; embryonal hepatoid cells | YST, Embryonal carcinoma (variable), Mixed GCT (if YST component) | Pure seminoma (NEVER), Choriocarcinoma (pure) |
| β-hCG | Syncytiotrophoblasts | Choriocarcinoma (markedly), Mixed GCT (if chorio component), Seminoma with STGCs (mildly, <1000 IU/L) | YST (pure) |
| LDH | Non-specific; correlates with tumor bulk and cell turnover | Any large or metastatic GCT (used in prognostic staging) | Not tumor-type specific |
Critical examination rules:
1. AFP is NEVER elevated in pure seminoma. Elevated AFP forces reclassification to NSGCT.
2. β-hCG can be mildly elevated in seminoma (due to STGCs) but remains below the level seen in choriocarcinoma.
3. AFP is physiologically elevated in normal infants up to 1 year of age — do not interpret a raised AFP as pathological in a neonate; use age-adjusted nomograms.
4. After orchiectomy, tumor markers should fall with appropriate half-lives (AFP t½ = 5–7 days; β-hCG t½ = 24–36 hours). Failure to fall appropriately indicates residual or metastatic disease.
Prognostic classification (IGCCCG): Good/Intermediate/Poor prognosis is determined by primary site, metastatic sites, and post-orchiectomy marker levels — LDH, AFP, β-hCG all feed into this risk score.
Tumor Marker Profiles in Testicular Germ Cell Tumors
SELF-CHECK
A 30-year-old man undergoes right radical orchiectomy for a testicular mass. Histology shows pure seminoma with no other components. Post-operatively, serum AFP is 320 IU/mL (normal <10). What is the MOST appropriate interpretation?
A. A. AFP elevation is expected in seminoma due to stromal reaction
B. B. This confirms Stage III seminoma requiring immediate chemotherapy
C. C. AFP elevation suggests an unsampled NSGCT component; the tumor should be reclassified
D. D. The AFP elevation is likely due to liver metastases
Reveal Answer
Answer: C. C. AFP elevation suggests an unsampled NSGCT component; the tumor should be reclassified
Pure seminoma is ALWAYS AFP-negative. An elevated post-orchiectomy AFP in a 'histologically pure' seminoma means the pathologist has missed a non-seminomatous component (yolk sac tumor, embryonal carcinoma). The tumor must be reclassified as a mixed GCT/NSGCT — this changes management from radiotherapy to cisplatin-based chemotherapy. The clinical rule is: AFP drives the diagnosis, not the histology alone.
Clinical Presentation and Staging
Clinical Presentation
The classic presentation is a painless, firm, intratesticular mass in a man aged 15–40 years. Key features:
- Painless — in contrast to epididymo-orchitis (which is painful and febrile). Acute pain occurs in ~10% (intratumoral hemorrhage, particularly in choriocarcinoma).
- Unilateral in >97% (bilateral GCTs in <2%).
- The mass does not transilluminate (solid tumor; hydrocele — which does — may coexist).
- Gynaecomastia may be present if the tumor secretes β-hCG or estrogen.
- Back pain/flank pain — suggests bulky para-aortic lymphadenopathy.
- Respiratory symptoms — lung metastases.
- Headache/neurological symptoms — rare but indicates brain metastases (poor prognosis).
Differential diagnosis of scrotal mass:
- Epididymo-orchitis (painful, tender, fever, raised WBC)
- Varicocele ('bag of worms', increases with Valsalva)
- Hydrocele (transilluminates)
- Spermatocele (above testis, transilluminates)
- Testicular GCT (solid, hard, non-tender)
Investigation
- Scrotal ultrasound: First-line — characterises the mass as intra- or extra-testicular and assesses vascularity.
- Serum tumor markers (AFP, β-hCG, LDH) — drawn BEFORE orchiectomy.
- CT chest, abdomen, pelvis — staging.
- Radical inguinal orchiectomy (NOT scrotal approach) — definitive diagnosis and initial treatment. Scrotal incision is contraindicated (disrupts lymphatic drainage to inguinal nodes and changes management).
Staging (TNM/Royal Marsden System)
| Stage | Description |
|---|---|
| I | Confined to testis (T1–T4 depending on vascular/lymphatic invasion or local extension) |
| II | Retroperitoneal (para-aortic) lymph node involvement |
| III | Mediastinal nodes, supraclavicular nodes, or visceral metastases (lung, liver, brain) |
Spread and Staging of Testicular Germ Cell Tumor
Spread, Prognosis, and Treatment Principles
Routes of Spread
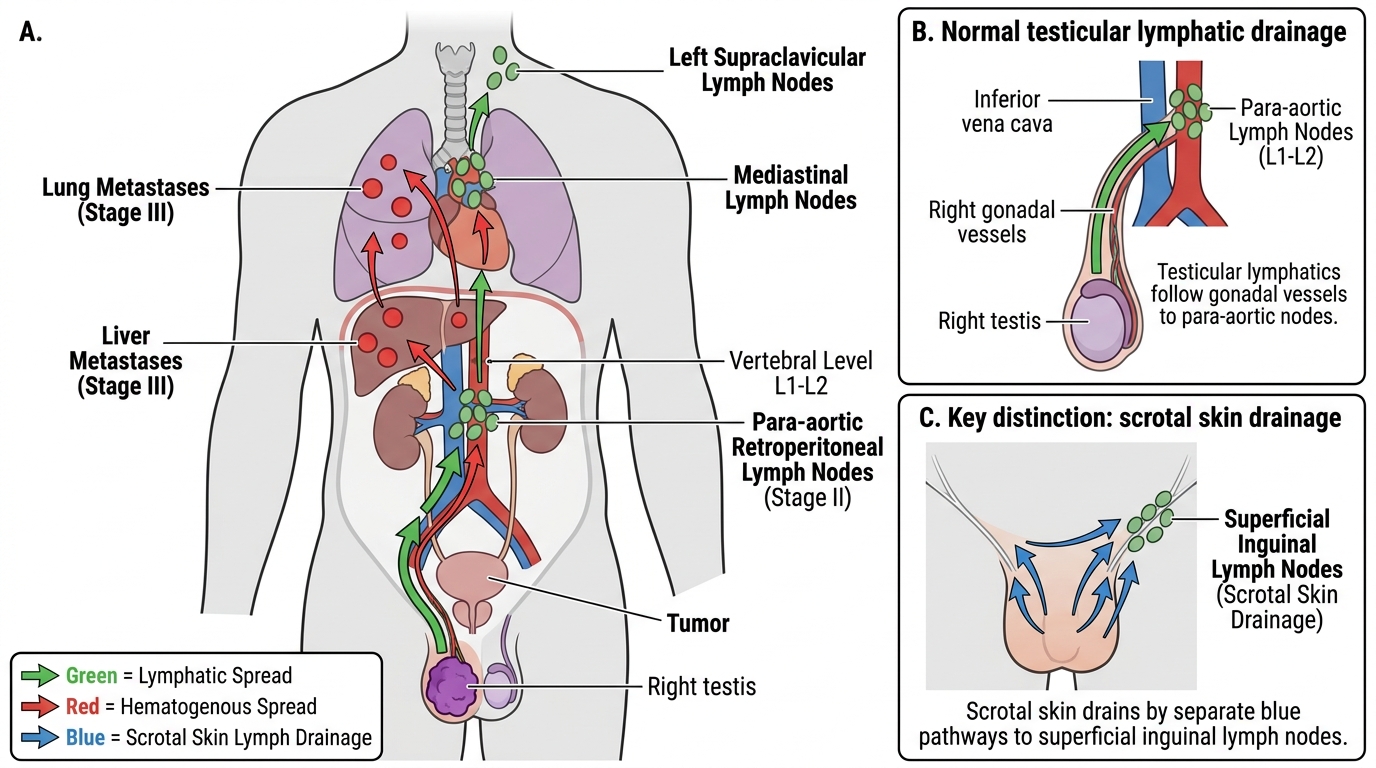
1. Local extension: Through the tunica albuginea into the epididymis, spermatic cord, or scrotal skin (changes stage).
2. Lymphatic spread (most common initial route in seminoma and most NSGCTs):
- Follows the testicular lymphatics along the gonadal vessels → para-aortic (retroperitoneal) nodes at L1–L2
- Then cephalad to mediastinal and supraclavicular nodes
3. Hematogenous spread:
- Choriocarcinoma: Hematogenous spread is the PRIMARY and EARLY route — lungs, liver, brain, even before nodal spread.
- Other NSGCTs: Hematogenous spread typically follows lymphatic spread — lungs are the most common site.
- Seminoma: Late hematogenous spread.
Prognosis
Testicular GCTs have excellent overall prognosis:
- Stage I seminoma: ~99% 5-year survival with orchiectomy ± surveillance/radiotherapy.
- Stage I NSGCT: ~95–98% with orchiectomy ± retroperitoneal lymph node dissection (RPLND).
- Metastatic GCT (Stage III): Good prognosis group ~92% 5-year survival; poor prognosis group ~50%.
- Adverse factors: Non-pulmonary visceral metastases (liver, brain, bone), markedly elevated AFP or β-hCG, mediastinal primary.
Treatment Principles
| Tumor Type | Stage I | Advanced Disease |
|---|---|---|
| Seminoma | Orchiectomy + surveillance or single-agent carboplatin or radiotherapy (para-aortic strip) | BEP chemotherapy (Bleomycin + Etoposide + cisPlatin); highly radiosensitive |
| NSGCT | Orchiectomy + RPLND or surveillance | BEP × 3–4 cycles; residual masses resected (may contain mature teratoma — 'growing teratoma syndrome') |
Spermatocytic tumor: Orchiectomy alone is curative.
Sex cord-stromal tumors: Orchiectomy; most benign.
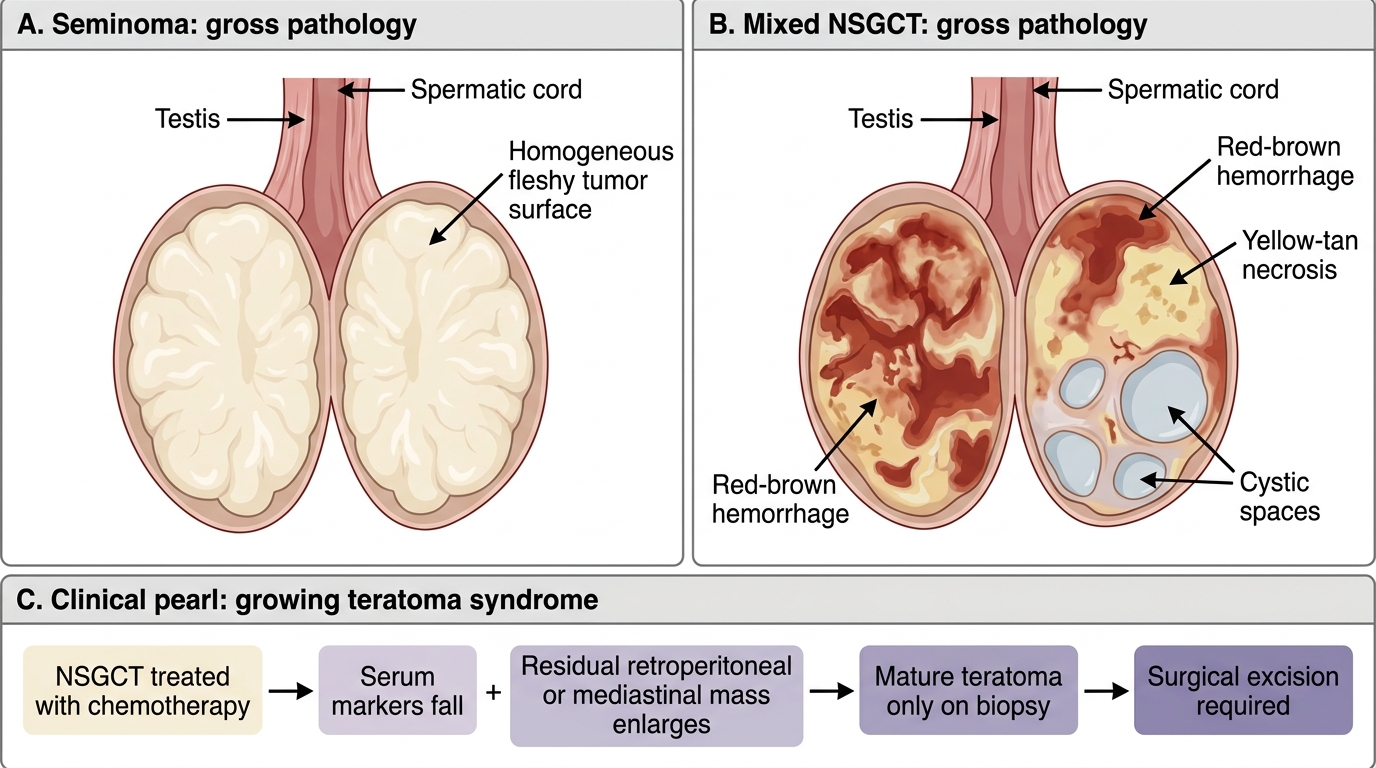
Gross Comparison of Seminoma and Mixed NSGCT
CLINICAL PEARL
'Growing teratoma syndrome': A rare but important phenomenon in NSGCTs. During or after chemotherapy, a residual mass in the retroperitoneum or mediastinum may actually enlarge — yet serum markers are falling. Paradoxically, this represents chemotherapy-induced differentiation: the viable embryonal carcinoma component has been killed, but the teratomatous component, which is chemo-resistant, is growing. These masses must be resected surgically because they can compress vital structures. Biopsy shows only mature teratoma. This is why all residual post-chemo masses in NSGCT are surgically excised.