Page 1 of 16
PA34.1-3 | CNS Infections & Tumors — SDL Guide
Learning Objectives
- Describe the etiology, types, and pathogenesis of meningitis, including distinguishing features of pyogenic, viral, tubercular, and fungal forms (PA34.1)
- Interpret CSF findings to identify the likely causative organism/category of meningitis from a given clinical scenario (PA34.3)
- Classify primary CNS tumors and describe the etiology, genetics, pathogenesis, gross/microscopic pathology, clinical presentation, and complications of major tumor types (PA34.2)
- Explain the mechanisms and consequences of raised intracranial pressure and cerebral herniation
INSTRUCTIONS
Two of the most rewarding topics in systemic pathology meet here: infections of the meninges and tumors of the brain. Both can be life-threatening; both are diagnosis-driven by very specific findings — the CSF report on one hand, the MRI and histopathology on the other. This module walks you through the pathological logic that connects an organism's virulence to the type of inflammatory exudate it produces, and a tumor's cell of origin to its genetics and behavior. Master the CSF interpretation table: it appears in almost every MBBS Professional examination. Engage actively — use the micro-quizzes to test yourself on clinical vignettes before the real exam does.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch. 28 — The Central Nervous System (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old college student is brought to the emergency room at 2 AM — sudden severe headache ('worst of my life'), neck so stiff his chin won't touch his chest, fever of 39.8 °C. His roommate says it started less than 12 hours ago. While you call neurology, the nurse draws blood cultures and you order a lumbar puncture. The CSF drips out under high pressure, cloudy like dishwater. You look at the report: WBC 12,000 cells/µL (90% neutrophils), protein 280 mg/dL, glucose 15 mg/dL (blood glucose 90 mg/dL). In the next 30 seconds, you have to decide: which organism, what empirical antibiotic, and how urgent is ICU transfer? Everything hinges on reading that CSF report. By the end of this module, you will read it faster than the resident.
WHY THIS MATTERS
CNS infections and tumors appear in every system of clinical medicine you will study. The neurologist, neurosurgeon, intensivist, paediatrician, and infectious disease specialist all need to interpret CSF and understand tumour pathology. In India, tubercular meningitis is still a leading cause of chronic meningitis and a major cause of preventable disability; the ability to distinguish it from pyogenic meningitis from a single CSF report saves lives and avoids incorrect treatment. CNS tumors — including glioblastoma (median survival 15 months even with treatment) — require accurate pathological diagnosis including molecular markers that now guide chemotherapy. For your Professional examinations, PA34.1–34.3 carry guaranteed short-answer and clinical-vignette marks. Understanding the pathogenesis — not just memorising facts — is what allows you to answer an unfamiliar scenario correctly.
RECALL
From your first-year anatomy and physiology, you know: the brain is enclosed in three layers — dura mater, arachnoid mater, and pia mater (collectively the meninges). Cerebrospinal fluid (CSF) fills the subarachnoid space and the ventricular system, produced by the choroid plexus and absorbed by arachnoid granulations. Normal CSF is crystal clear, has 0–5 lymphocytes/µL, protein 15–45 mg/dL, and glucose 50–80 mg/dL (about two-thirds of blood glucose). From microbiology, you know that Streptococcus pneumoniae and Neisseria meningitidis are leading causes of bacterial meningitis. From biochemistry, the blood–brain barrier restricts entry of large molecules and immune cells into the CNS. Now we build on this — exploring what happens when pathogens breach that barrier, and what happens when brain cells themselves go rogue.
Meningitis — Classification and Pathogenetic Routes
Meningitis is inflammation of the meninges (the leptomeninges — arachnoid + pia — are primarily involved). It is classified by the dominant cell type in CSF, which directly reflects the nature of the infecting organism:
- Purulent (pyogenic/bacterial) — neutrophilic exudate; CSF looks cloudy/turbid
- Aseptic (viral/lymphocytic) — lymphocytic exudate; CSF clear or mildly turbid
- Chronic (granulomatous) — tubercular or fungal; lymphocytic/mixed; often basal predominance
How do organisms reach the meninges? Three main routes:
- Haematogenous (bacteraemia/viraemia) — most common. Organism seeds meninges from blood (e.g., N. meningitidis from nasopharynx → blood → meninges).
- Direct extension — from adjacent focus: sinusitis (frontal → frontal lobe), otitis media, mastoiditis, skull fracture with CSF leak, dental abscess.
- Retrograde neuronal transport — viral (e.g., HSV, rabies virus travel along axons to CNS).
Once organisms breach the blood–brain barrier and enter the subarachnoid space, the inflammatory cascade is amplified because the CNS lacks normal lymphatic drainage and has limited local immune surveillance — a space where even a small infection can generate devastating pressure.
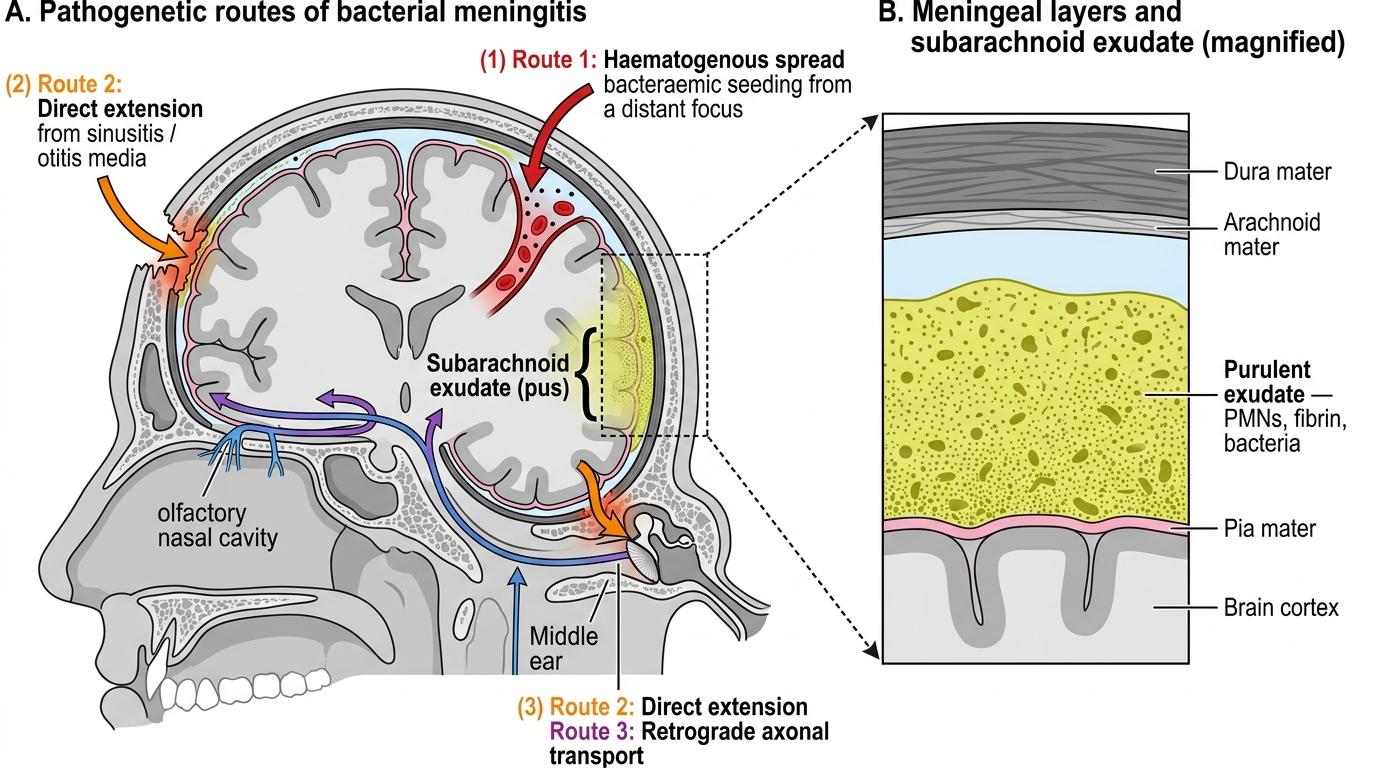
Meningeal Anatomy and Pathogenetic Routes of Bacterial Meningitis
Acute Pyogenic (Bacterial) Meningitis — Pathogens by Age Group
The causative organism varies strongly with patient age — one of the most frequently examined facts in pathology:
| Age Group | Leading Organisms |
|---|---|
| Neonates (0–4 weeks) | E. coli (K1 capsule), Group B Streptococcus (S. agalactiae), Listeria monocytogenes |
| Infants/toddlers (1 month–2 years) | Haemophilus influenzae type b (Hib), Streptococcus pneumoniae, N. meningitidis |
| Children & young adults (5–30 years) | Neisseria meningitidis (commonest in this group; epidemics in hostels, colleges) |
| Adults (>30 years) | Streptococcus pneumoniae (most common overall in adults; also in elderly) |
| Elderly & immunocompromised | L. monocytogenes, Gram-negative rods |
Key virulence feature: Bacteria that cause meningitis share one structural trait — a polysaccharide capsule that resists phagocytosis (e.g., S. pneumoniae, H. influenzae, N. meningitidis, E. coli K1). This allows bacteraemia and seeding of meninges.
Pneumococcal meningitis is the most lethal form with highest mortality and neurological sequelae. Meningococcal meningitis can present with petechial/purpuric rash and fulminant Waterhouse–Friderichsen syndrome (bilateral adrenal haemorrhage → adrenal failure).
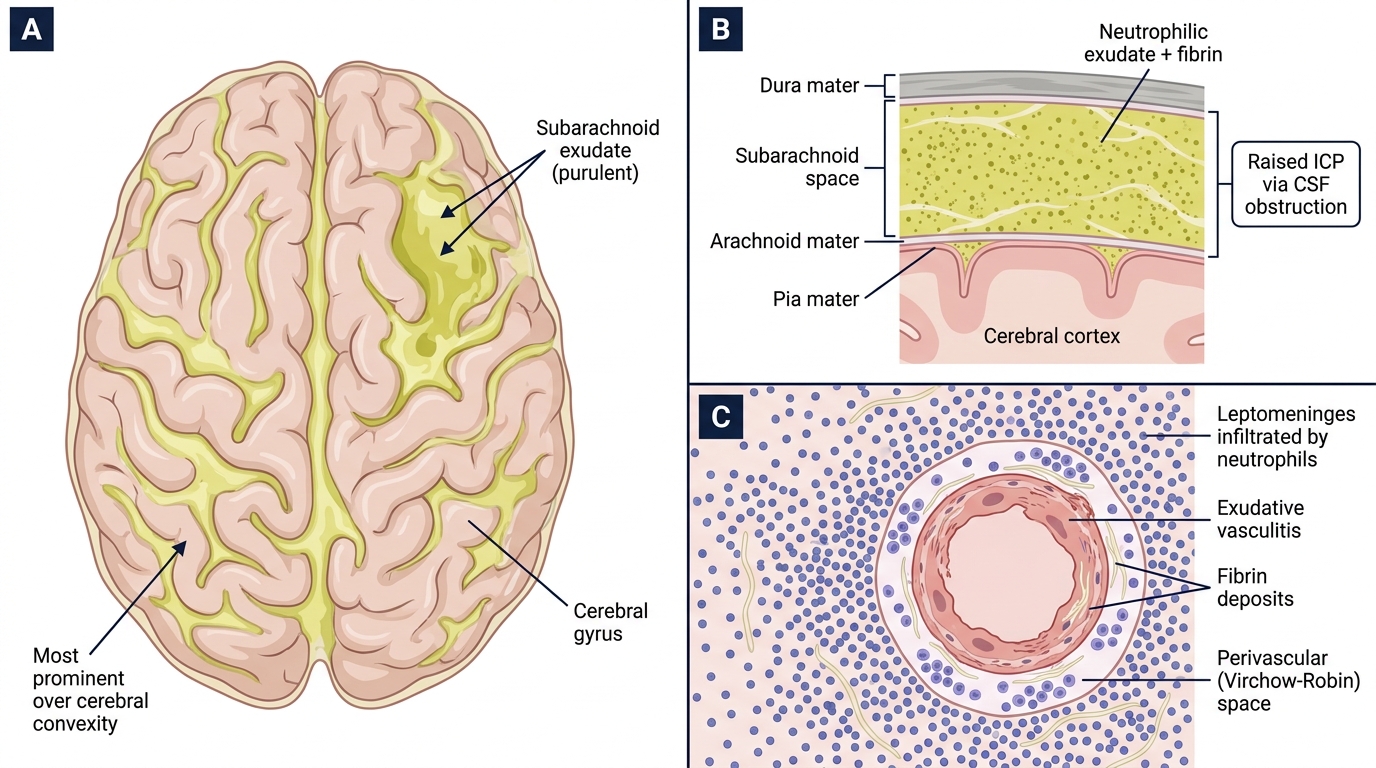
Acute Bacterial (Pyogenic) Meningitis — Gross Pathology, Meningeal Cross-section, and Histology
Pathogenesis and Microscopy of Acute Pyogenic Meningitis
Pathogenesis sequence:
- Bacteria colonise nasopharynx → bacteraemia → penetrate choroid plexus or inflamed cerebrovascular endothelium → enter subarachnoid space.
- Bacterial products (LPS, peptidoglycan, teichoic acid) activate pattern-recognition receptors (TLRs) on resident microglia and meningeal macrophages → pro-inflammatory cytokine storm (IL-1β, TNF-α, IL-6).
- Cytokines → increased blood–brain barrier permeability, neutrophil influx → purulent exudate in subarachnoid space.
- Exudate obstructs CSF flow → communicating hydrocephalus and raised ICP.
- Vasculitis of meningeal and cortical vessels → infarction.
- Toxins + inflammation → direct neuronal injury.
Gross pathology: The brain surface is covered by a thick, creamy-yellow to green purulent exudate, most prominent over the cerebral convexities and at the base of the brain. In H. influenzae and pneumococcal meningitis, the exudate is particularly thick at the base.
Microscopy (histology): Leptomeninges infiltrated by massive neutrophilic exudate with fibrin. Polymorphs in perivascular Virchow–Robin spaces. Cortical vessels show exudative vasculitis. In early stages: vascular engorgement and oedema.
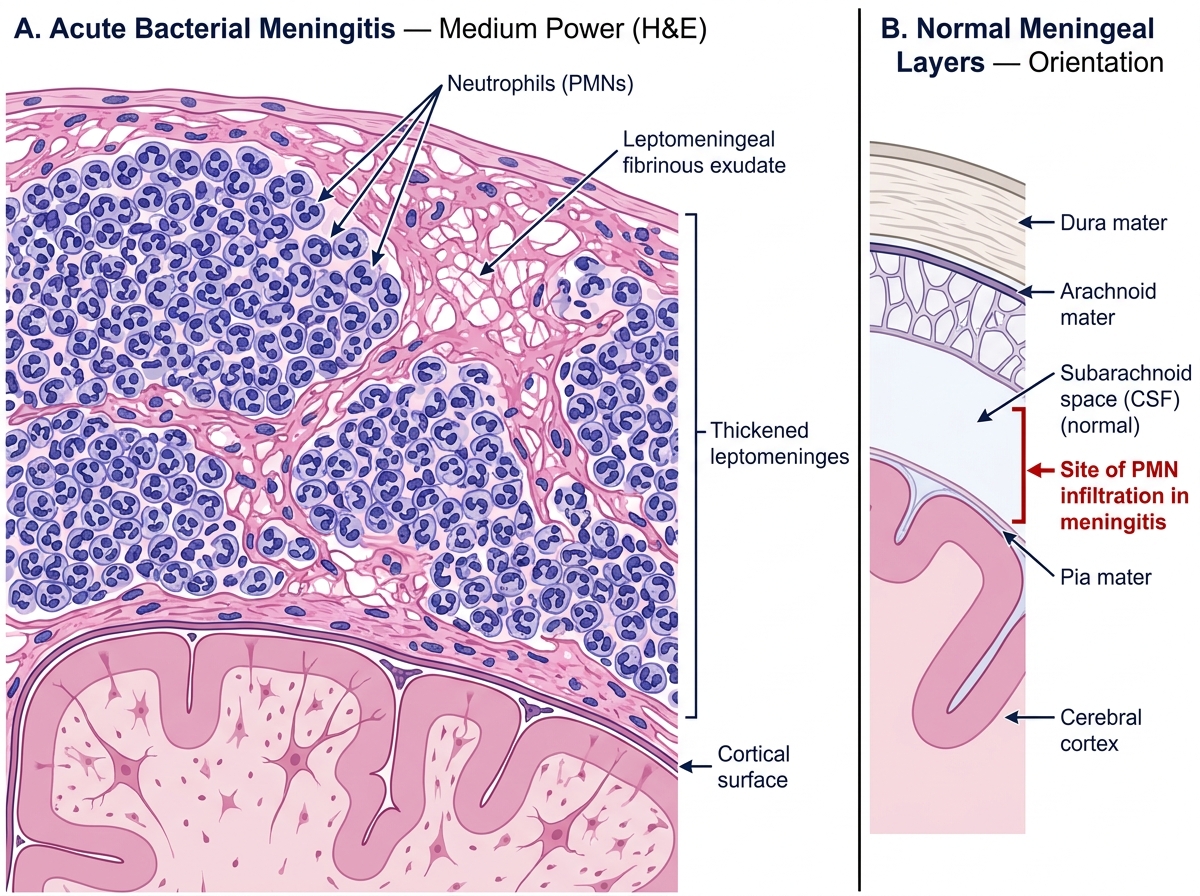
Histology of Acute Bacterial Meningitis — Medium Power (H&E)