Page 2 of 16
PA34.1-3 | CNS Infections & Tumors — SDL Guide (Part 2)
Complications of Pyogenic Meningitis
Complications explain why bacterial meningitis carries a mortality of 20–30% even with treatment, and why 30–50% of survivors have permanent neurological deficits:
Acute complications:
• Cerebral oedema → raised ICP → herniation
• Septicaemia/septic shock → multi-organ failure
• Waterhouse–Friderichsen syndrome (meningococcal) — adrenal haemorrhage, DIC, purpura fulminans
• Subdural empyema — pus collection between dura and arachnoid
• Venous sinus thrombosis — sagittal or cavernous sinus
Subacute/chronic complications:
• Communicating hydrocephalus — fibrinous exudate blocks arachnoid villi → impaired CSF absorption (most common long-term complication)
• Cerebral infarction — vasculitis of leptomeningeal vessels → ischaemia
• Cranial nerve palsies — CN III, VI (oculomotor, abducens — involvement causes diplopia/strabismus), CN VIII (vestibulocochlear → sensorineural hearing loss — most common neurological sequela in children)
• Epilepsy — cortical irritation and scarring
• Intellectual disability — especially if untreated/delayed in neonates
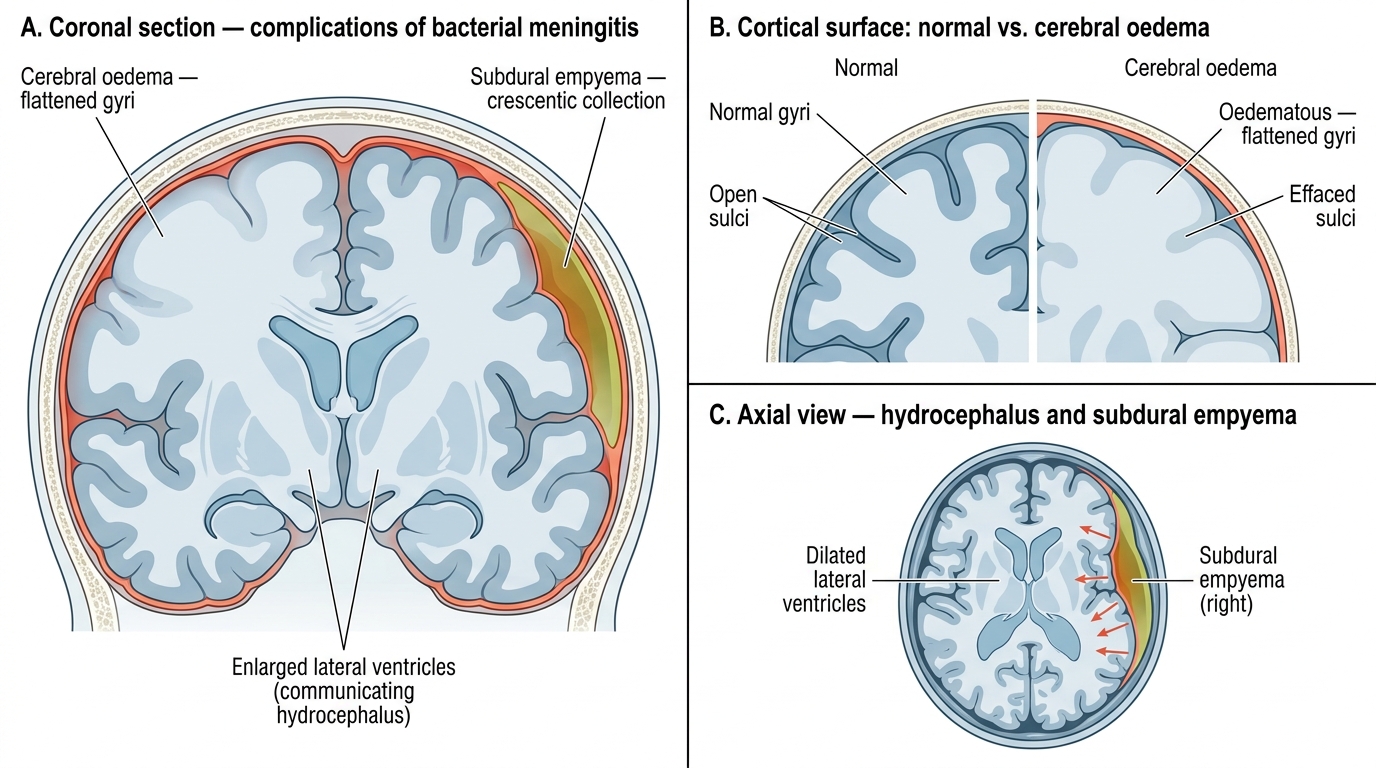
Complications of Bacterial Meningitis — Brain Cross-Section
CLINICAL PEARL
Kernig's and Brudzinski's signs are both tests for meningeal irritation caused by inflammation of the spinal meninges: Kernig's — the patient cannot fully extend the knee with the hip flexed to 90° (pain/resistance); Brudzinski's — passive neck flexion causes involuntary hip and knee flexion. Both are positive in bacterial meningitis. The pathological basis is chemical irritation of nerve roots passing through the inflamed subarachnoid space. Clinical pearl: In immunocompromised patients (HIV, elderly), meningeal signs may be absent even with severe bacterial meningitis — always LP if clinically suspected. Also: do a CT head BEFORE LP if there is papilloedema, focal neuro deficit, or altered sensorium, to rule out space-occupying lesion (risk of herniation with LP if raised ICP).
Viral (Aseptic) Meningitis
Aseptic meningitis refers to meningitis with a lymphocytic CSF pleocytosis where routine bacterial cultures are negative. The term 'aseptic' is historical — most cases are viral.
Common causes:
• Enteroviruses (Coxsackievirus, Echovirus) — most common cause of viral meningitis overall; typically summer/autumn; often affects children
• Herpes simplex virus type 2 (HSV-2) — especially in genital herpes; causes recurrent benign lymphocytic meningitis (Mollaret's meningitis)
• Mumps virus — pre-vaccine era; benign; CN VIII involvement
• HIV — acute seroconversion illness (primary HIV meningitis)
• Arboviruses — Japanese encephalitis (important in India), West Nile virus
Pathogenesis: Viruses reach CNS via haematogenous or neuronal route → infect meningeal cells and ependyma → lymphocyte and monocyte recruitment (not neutrophils, because viral antigens stimulate adaptive immunity, not innate neutrophil response).
Gross pathology: Brain may appear grossly normal or mildly hyperaemic. No thick exudate (unlike bacterial).
Microscopy: Lymphocytic infiltration of leptomeninges. Perivascular lymphocytic cuffing. Microglial nodules in encephalitis.
Course: Usually self-limiting in 7–10 days. No specific treatment (except acyclovir for HSV encephalitis, which is a more severe form). Complete recovery in most cases.
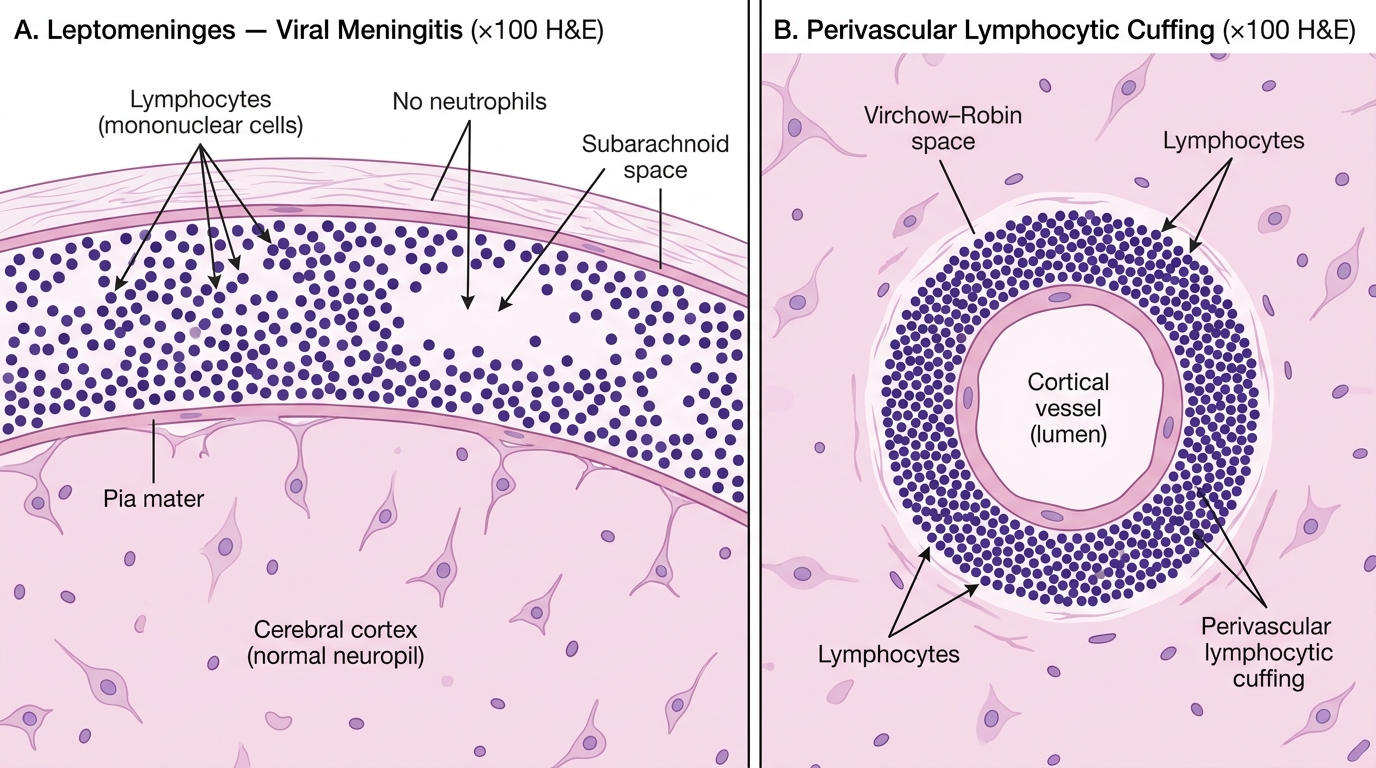
Viral Meningitis — Leptomeningeal Lymphocytic Infiltrate and Perivascular Cuffing (H&E, ×100)
Tubercular Meningitis — Pathogenesis and Gross Pathology
Tubercular meningitis (TBM) is the most important form of chronic granulomatous meningitis and the leading cause of meningitis mortality in India and high-burden countries. It requires urgent diagnosis as untreated disease kills within weeks.
Pathogenesis:
- Primary pulmonary TB (or reactivation) → haematogenous dissemination → subpial/subependymal tuberculoma forms in brain or meninges (Rich focus).
- Rich focus ruptures → tuberculoprotein released into subarachnoid space → intense inflammatory reaction.
- Exudate predominantly at the base of the brain (basal exudate) — this is the hallmark distribution of TBM.
- Granuloma formation: central caseous necrosis surrounded by epithelioid macrophages, Langhans giant cells, and lymphocytes.
Gross pathology:
• Thick gelatinous grey exudate at the base of the brain — involving the sylvian fissures, interpeduncular cistern, and surface of cerebellum.
• Tiny miliary tubercles (1–2 mm) scattered on meninges and parenchyma.
• Hydrocephalus (obstructive or communicating) — very common, from blockage at basal cisterns.
• Arteritis of vessels at base → infarcts (especially basal ganglia via Heubner's artery).
India-specific importance: TBM presents insidiously over 2–8 weeks (fever, headache, weight loss, night sweats), unlike the acute onset of pyogenic meningitis. This subacute presentation in an Indian patient with positive family history or prior TB exposure should always raise suspicion of TBM.
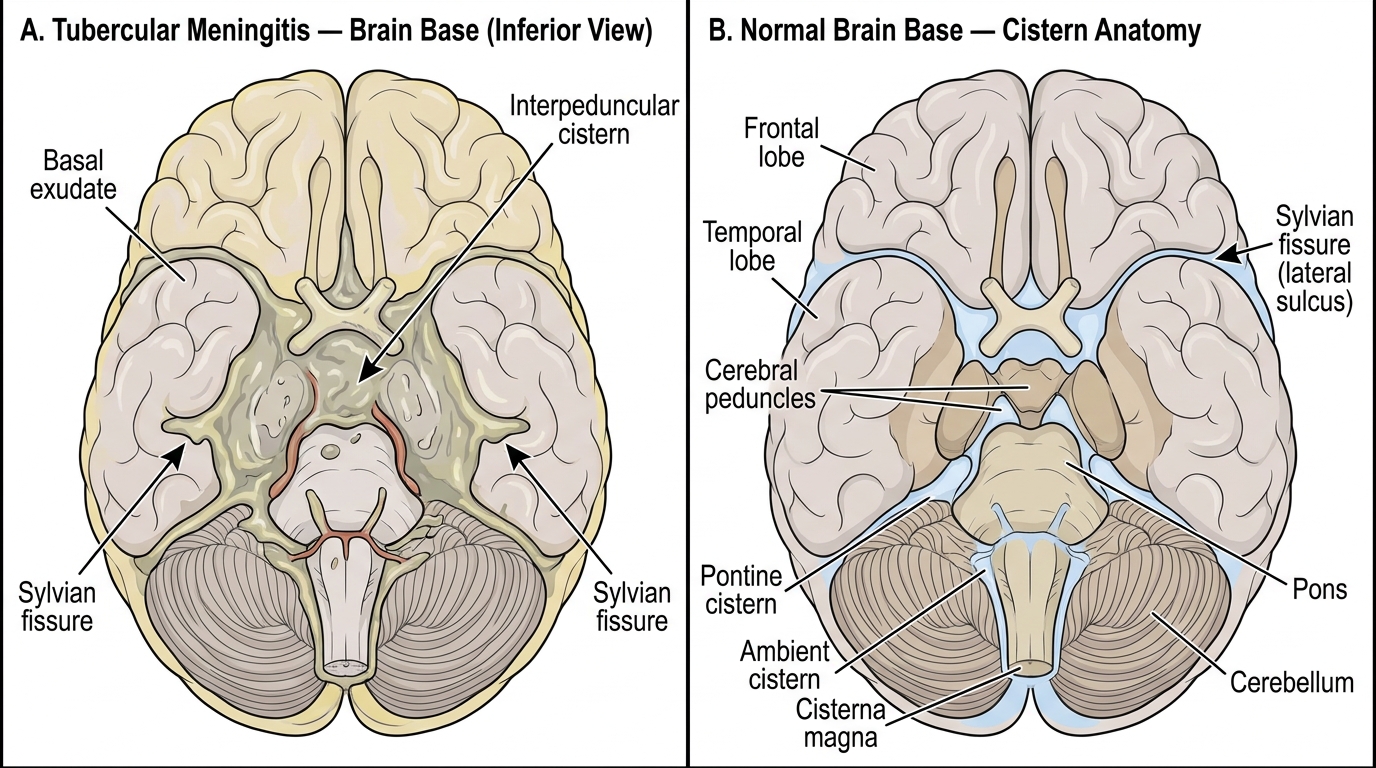
Tubercular Meningitis: Brain Base Gross Pathology