Page 3 of 16
PA34.1-3 | CNS Infections & Tumors — SDL Guide (Part 3)
Tubercular Meningitis — Histology and Sequelae
Microscopy (histology) of TBM:
• Granuloma — the hallmark histological lesion: central caseous necrosis surrounded by radially arranged epithelioid macrophages (modified histiocytes), Langhans giant cells (horseshoe/peripheral arrangement of nuclei), and outer rim of lymphocytes and plasma cells.
• Acid-fast bacilli (AFB) may be seen with Ziehl–Neelsen (ZN) stain — though yield is low in tissue sections (more reliable in CSF culture/PCR).
• Fibrinous exudate and lymphocytes in subarachnoid space.
• Endarteritis of basal vessels → fibrinoid necrosis → infarcts.
Sequelae and complications:
• Hydrocephalus (most common complication; can be communicating or obstructive from aqueductal stenosis)
• Cranial nerve palsies — CN III, IV, VI, VII, VIII from basal exudate compressing nerves
• Cerebral infarctions — particularly basal ganglia
• Spinal arachnoiditis → cord compression, paraplegia
• SIADH (syndrome of inappropriate ADH secretion) → hyponatraemia
• Paradoxical reaction on anti-TB therapy (IRIS — immune reconstitution inflammatory syndrome)
CSF AFB smear positive in only 10–40%; culture (gold standard) takes 4–8 weeks; PCR and adenosine deaminase (ADA) levels are useful adjuncts in Indian practice.
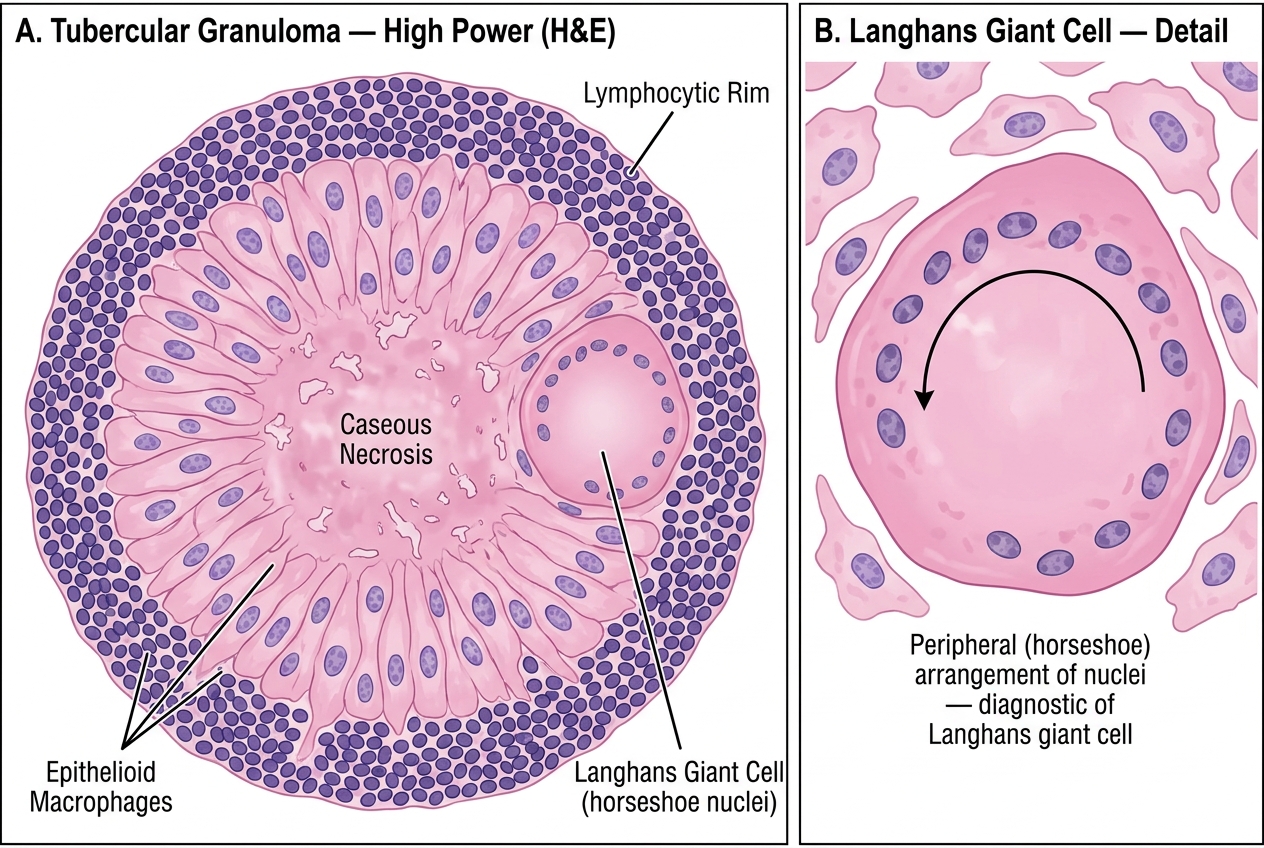
Histology of Tubercular Granuloma (High Power) — Langhans Giant Cell and Concentric Zones
Fungal Meningitis — Cryptococcal Meningitis
Cryptococcal meningitis is the most important fungal CNS infection and a leading opportunistic infection in HIV/AIDS (CD4 count <100 cells/µL) and other immunocompromised states (organ transplant, lymphoma, high-dose steroids).
Organism: Cryptococcus neoformans — an encapsulated yeast found in soil, bird droppings (especially pigeon). The polysaccharide capsule is its key virulence factor — it inhibits phagocytosis, impairs T-cell responses, and is the target of diagnostic tests (India ink, cryptococcal antigen/CrAg).
Pathogenesis:
• Inhalation → pulmonary infection → haematogenous spread → CNS.
• CNS disease particularly severe because cryptococcal capsule resists immune clearance in a space with limited immune surveillance.
• Soap-bubble lesions (gelatinous pseudocysts) in basal ganglia and grey matter — fungi expand locally with minimal inflammation (in immunosuppressed hosts).
Gross pathology: Brain surface may show minimal exudate (unlike pyogenic). Cut section reveals characteristic 'soap-bubble' or gelatinous pseudocysts in basal ganglia and cerebral cortex — filled with clusters of encapsulated yeasts, minimal host reaction.
Microscopy:
• India ink preparation of CSF — pathognomonic: dark background with clear halo of mucoid capsule around budding yeast cells. Single narrow-based budding distinguishes from Candida (which shows germ tubes/pseudohyphae).
• Mucicarmine stain — stains capsule red/magenta.
• Minimal inflammatory reaction in immunocompromised host.
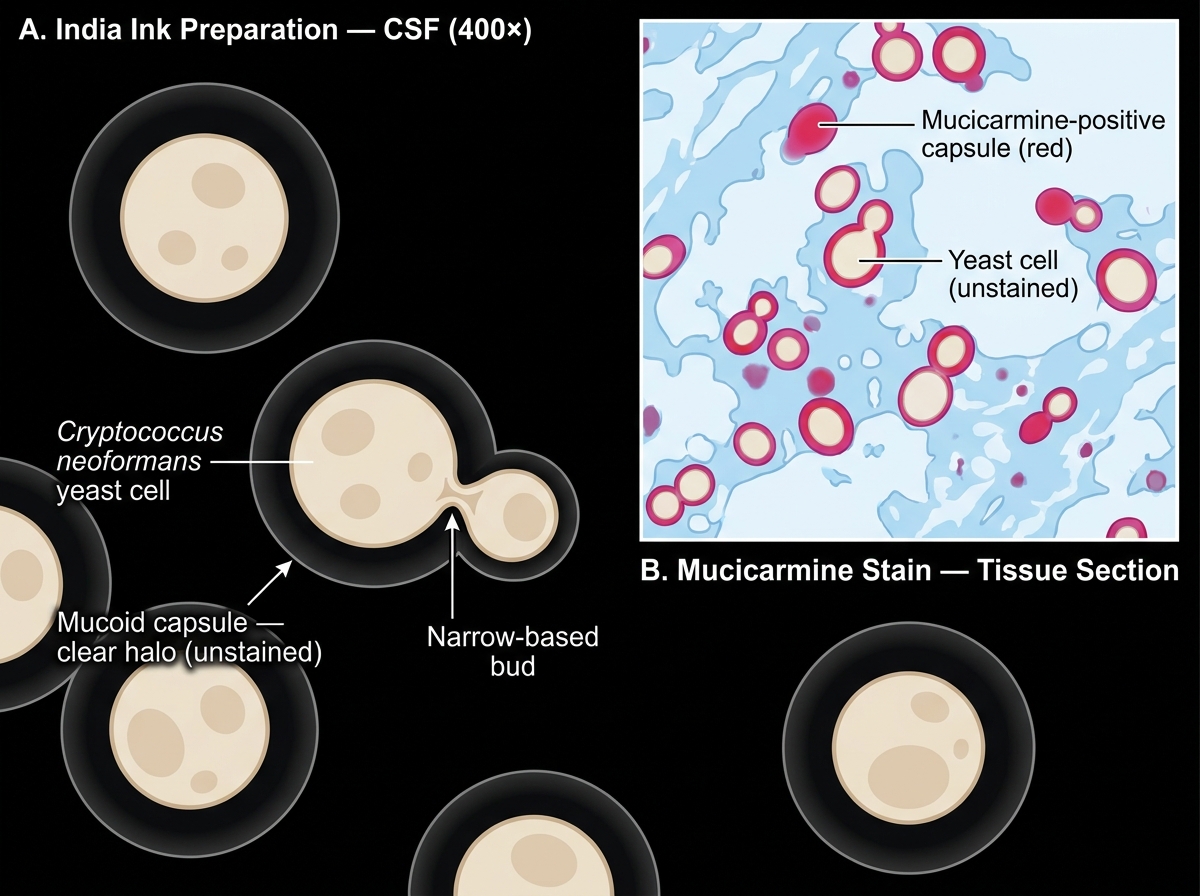
Cryptococcus neoformans — India Ink CSF Preparation and Mucicarmine Tissue Stain
CSF Interpretation Framework — The Essential Comparison Table
This is the single most examined topic in meningitis pathology. Learn the table; understand the logic behind each parameter.
Logic of each parameter:
• Appearance: turbidity reflects cell count; xanthochromia (yellow) = prior haemorrhage or very high protein; pellicle/cobweb clot on standing = TBM (fibrin threads).
• Opening pressure: raised whenever inflammation is present (pyogenic > tubercular > viral; fungal can be very high).
• Cell count and predominant cell type: The key discriminator — neutrophils = bacteria (including early TB, before granuloma forms); lymphocytes = viral, TB, fungal, partially treated bacterial.
• Protein: elevated in all meningitis; very high in bacterial/TB (breakdown of BBB + exudate protein).
• Glucose: LOW in bacterial/TB/fungal (organisms + neutrophils/macrophages consume glucose); NORMAL in viral (viruses don't metabolise glucose in CSF; lymphocytes do not significantly consume glucose). Always compare with simultaneous blood glucose (CSF glucose <50% of blood glucose = hypoglycorrhachia = pathological).
• Gram stain: positive in ~80% of untreated bacterial meningitis.
| Parameter | Normal | Bacterial (Pyogenic) | Viral (Aseptic) | Tubercular | Fungal (Crypto) |
|---|---|---|---|---|---|
| Appearance | Crystal clear | Turbid/purulent, cloudy | Clear / mildly turbid | Clear / turbid; cobweb clot | Clear / slightly turbid |
| Opening pressure | 6–20 cm H₂O | Markedly raised | Normal/mildly raised | Moderately raised | Raised (often very high) |
| Total cells/µL | 0–5 | 1,000–10,000+ | 10–500 | 100–500 | 10–200 |
| Predominant cell | Lymphocytes | Neutrophils (>80%) | Lymphocytes (>80%) | Lymphocytes (mixed early) | Lymphocytes |
| Protein (mg/dL) | 15–45 | Very high (>100, up to 500) | Mildly raised (50–100) | High (100–500) | Mildly–moderately raised |
| Glucose (mg/dL) | 50–80 (⅔ of blood) | Very low (<40) | Normal (>50% of blood) | Low (<45) | Low |
| Glucose ratio | >0.6 | <0.4 (often <0.2) | >0.6 | <0.5 | Low |
| Special tests | — | Gram stain+; culture; CRP | PCR for virus | ZN/AFB smear; ADA; PCR | India ink; CrAg; culture |
Memory hook: "Bacteria eat all the glucose and call all the neutrophils. Viruses are polite — they raise cells a little, never touch the glucose, and call only lymphocytes." TB is in between — lymphocytes, but it does consume glucose.
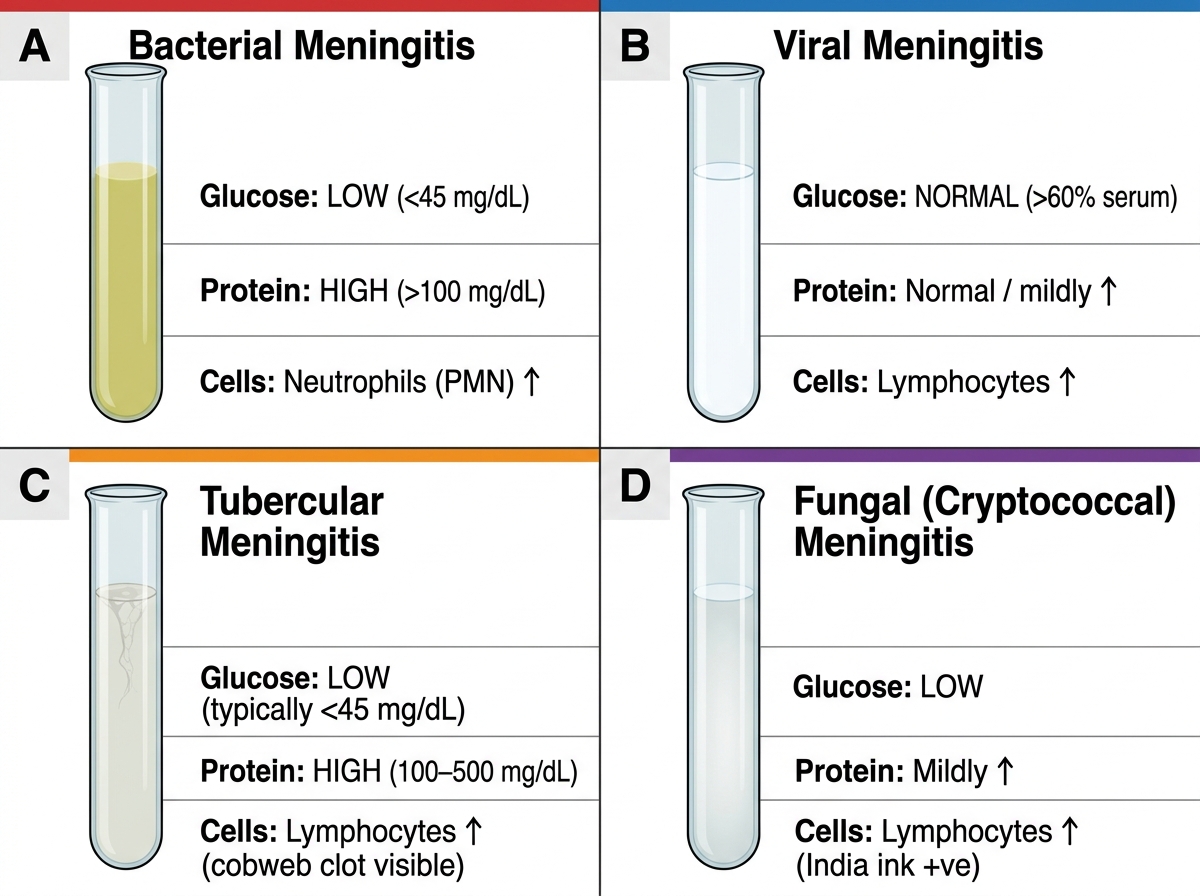
CSF Tube Appearance and Key Values in the Four Types of Meningitis
SELF-CHECK
A 45-year-old HIV-positive man (CD4 = 65 cells/µL) presents with 3 weeks of progressive headache, nausea, and blurred vision. LP shows: opening pressure 35 cm H₂O, clear CSF, WBC 40 cells/µL (95% lymphocytes), protein 80 mg/dL, glucose 32 mg/dL (blood glucose 90 mg/dL). India ink preparation is positive. Which organism is most likely, and what is the key virulence factor that explains the lymphocytic (rather than neutrophilic) response?
A. Neisseria meningitidis — endotoxin (LPS) is the virulence factor
B. Cryptococcus neoformans — polysaccharide capsule inhibits phagocytosis and impairs T-cell activation
C. Mycobacterium tuberculosis — cord factor (trehalose dimycolate) causes granuloma formation
D. Streptococcus pneumoniae — polysaccharide capsule causes opsonisation resistance
Reveal Answer
Answer: B. Cryptococcus neoformans — polysaccharide capsule inhibits phagocytosis and impairs T-cell activation
Correct: Cryptococcus neoformans. The clinical context (HIV, low CD4, subacute course, very high opening pressure, clear CSF, lymphocytic pleocytosis, low glucose, positive India ink) is classic for cryptococcal meningitis. The mucoid polysaccharide capsule is the key virulence factor — it inhibits neutrophil phagocytosis, impairs complement activation, and blunts T-cell-mediated immunity, resulting in lymphocytic (not neutrophilic) pleocytosis. In severely immunocompromised patients, even this lymphocytic response may be minimal ('pauci-cellular' CSF), worsening prognosis. Treatment: amphotericin B + flucytosine induction, then fluconazole maintenance.
SELF-CHECK
A 3-year-old child presents with sudden high fever, bulging fontanelle, and irritability for 24 hours. LP: WBC 8,500/µL (88% neutrophils), protein 320 mg/dL, glucose 10 mg/dL (blood glucose 85 mg/dL). Gram stain shows Gram-negative coccobacilli. Which organism is most likely, AND which complication explains why this age group needs prophylaxis of close contacts?
A. Streptococcus pneumoniae (Gram-positive diplococci) — subdural empyema risk
B. Haemophilus influenzae type b (Gram-negative coccobacilli) — risk of secondary cases among household contacts; rifampicin prophylaxis indicated
C. Neisseria meningitidis (Gram-negative diplococci) — Waterhouse–Friderichsen syndrome risk
D. Listeria monocytogenes (Gram-positive rod) — motor neuron complication in neonates
Reveal Answer
Answer: B. Haemophilus influenzae type b (Gram-negative coccobacilli) — risk of secondary cases among household contacts; rifampicin prophylaxis indicated
Correct: Haemophilus influenzae type b (Hib). In the pre-Hib vaccine era, this was the leading cause of meningitis in children 1 month to 5 years. Gram-negative coccobacilli is the morphological clue. The WBC and glucose profile confirm acute pyogenic meningitis. Hib can spread among unvaccinated household contacts of young children — rifampicin prophylaxis (4 days) is given to household contacts with children under 4 years old. Note: Hib vaccination (PCV) has dramatically reduced incidence in immunised populations. In India, the Universal Immunisation Programme now includes Hib vaccine.