Page 4 of 16
PA34.1-3 | CNS Infections & Tumors — SDL Guide (Part 4)
CNS Tumors — Classification Principles
Primary CNS tumors arise from brain parenchyma, meninges, or cranial nerve sheaths. Secondary (metastatic) tumors arise elsewhere and spread to the CNS.
Critical fact: In adults, metastatic tumors are more common than primary tumors. The most common sources of brain metastases are:
1. Lung (most common overall — especially small cell carcinoma and adenocarcinoma)
2. Breast
3. Melanoma (highest propensity to metastasise per primary tumor)
4. Kidney (RCC)
5. Colon
Mnemonic: "Look, Beautiful, My Kidney Colon" — Lung, Breast, Melanoma, Kidney, Colon.
Classification of primary CNS tumors:
I. Glial tumors (Gliomas) — most common primary CNS tumors; arise from glial cells:
• Astrocytomas (from astrocytes) — includes glioblastoma (Grade 4)
• Oligodendroglioma (from oligodendrocytes)
• Ependymoma (from ependymal cells lining ventricles)
II. Non-glial tumors:
• Meningioma — from arachnoid cap cells
• Medulloblastoma — from cerebellar primitive cells (embryonal tumor)
• Schwannoma — from Schwann cells of cranial nerves
• Primary CNS lymphoma — usually B-cell; associated with HIV
• Craniopharyngioma — from Rathke's pouch remnants; suprasellar
WHO grading (Grade 1–4): Based on mitosis, necrosis, vascular proliferation, and molecular markers. Grade 4 = highest malignancy, shortest survival.
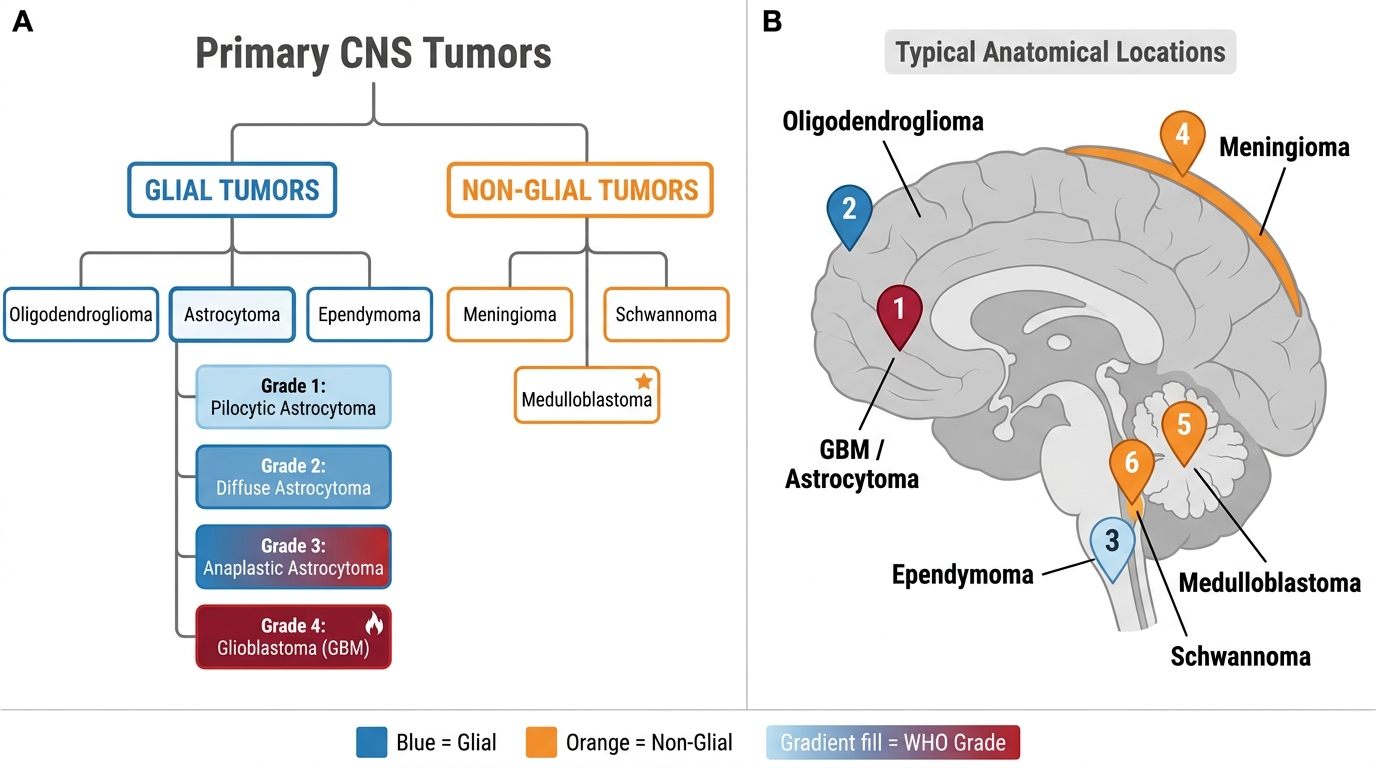
Classification of Primary CNS Tumors and Their Anatomical Locations
Glioblastoma (Astrocytoma Grade 4) — Pathology and Molecular Markers
Glioblastoma (GBM) is the most common and most malignant primary brain tumor in adults. Mean age of onset: 55–65 years. Median survival: 12–15 months despite surgery + radiotherapy + temozolomide.
Molecular markers — essential for exam and clinical management:
- IDH1/IDH2 mutation: Isocitrate dehydrogenase mutation is the most important prognostic marker. IDH-wild type GBM = primary GBM (de novo, worse prognosis, majority of adult GBMs). IDH-mutant GBM = secondary GBM (arises from lower-grade astrocytoma, slightly better prognosis). IDH mutation → 2-hydroxyglutarate accumulation → epigenetic reprogramming → tumorigenesis.
- MGMT promoter methylation: O-6-methylguanine-DNA methyltransferase is a DNA repair enzyme. Methylation of MGMT promoter silences it → tumor cannot repair alkylating-agent damage → better response to temozolomide chemotherapy. ~40% of GBMs are MGMT-methylated — these patients do significantly better.
- EGFR amplification: Common in primary GBM. Epidermal growth factor receptor overexpression drives cell proliferation.
Gross pathology:
• Large irregular mass with central necrosis and haemorrhage (variegated cut surface — grey-white necrotic areas, yellow necrotic core, red haemorrhagic areas — resembling a butterfly across the corpus callosum in butterfly glioma).
• Poorly defined margins — infiltrates surrounding brain widely.
• Satellite lesions may be present.
Microscopy — two pathognomonic features:
1. Pseudopalisading necrosis (serpentine/geographic necrosis) — areas of necrosis rimmed by densely packed tumour cells arranged in a palisade (picket-fence pattern) as cells migrate away from the hypoxic centre.
2. Microvascular proliferation (glomeruloid bodies) — tufted, multilayered, thickened vessel walls resembling renal glomeruli — driven by VEGF released by hypoxic tumor cells.
Additionally: high mitotic rate, nuclear pleomorphism, hypercellularity.
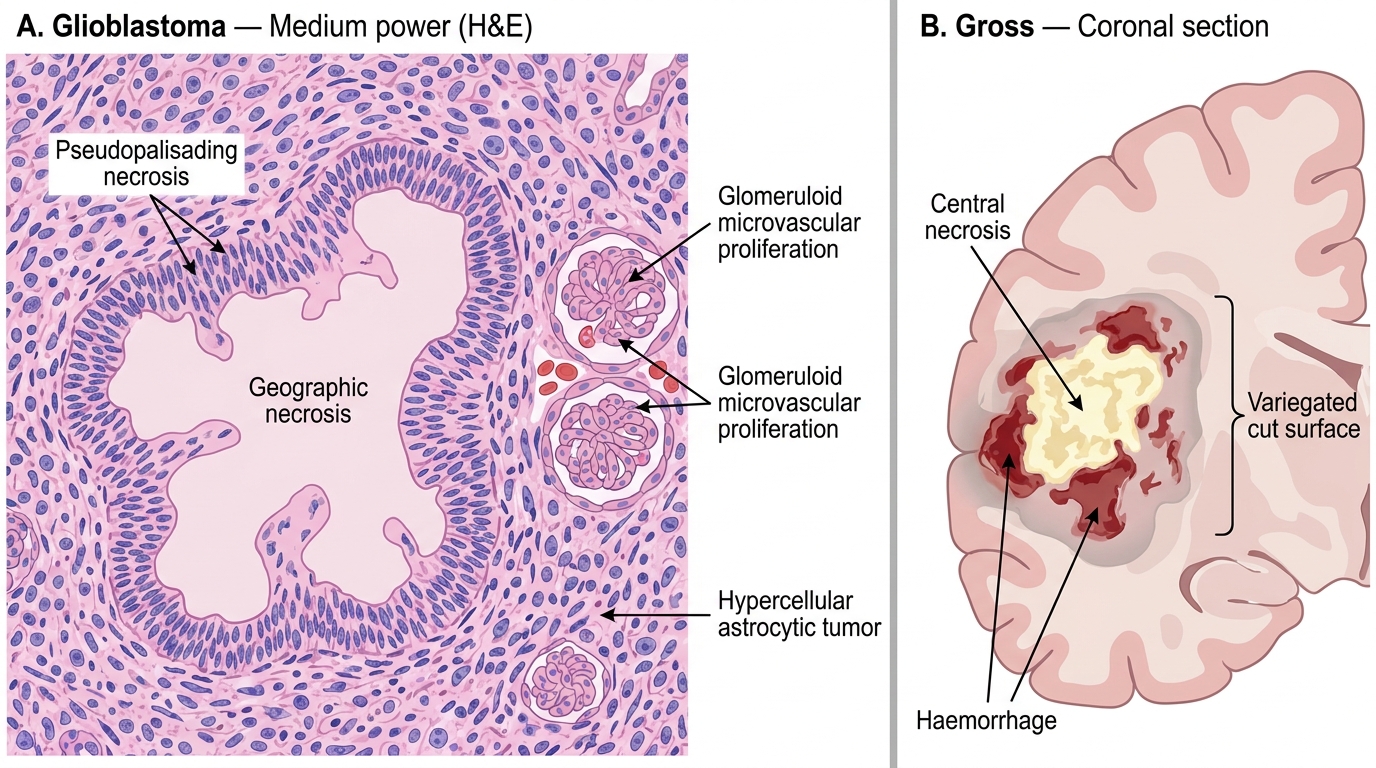
Glioblastoma: Histology and Gross Pathology
Oligodendroglioma and Ependymoma
Oligodendroglioma:
- Arises from oligodendrocytes. Grade 2 (low grade) or Grade 3 (anaplastic). Typically in the frontal lobe in adults (30–40s).
- 1p/19q codeletion — the defining molecular alteration; seen in virtually 100% of true oligodendrogliomas. This codeletion confers better prognosis and sensitivity to procarbazine–CCNU–vincristine (PCV) chemotherapy.
- IDH mutation is also present (IDH-mutant + 1p/19q codeleted = WHO oligodendroglioma).
- Gross: Soft, gelatinous tumour, often with calcification (seen on CT as stippled calcification).
- Microscopy — "fried egg appearance": round uniform nuclei surrounded by abundant clear cytoplasm (due to formalin fixation artefact causing perinuclear halo). No fibrillary processes. Chicken-wire vascular pattern (delicate branching capillaries).
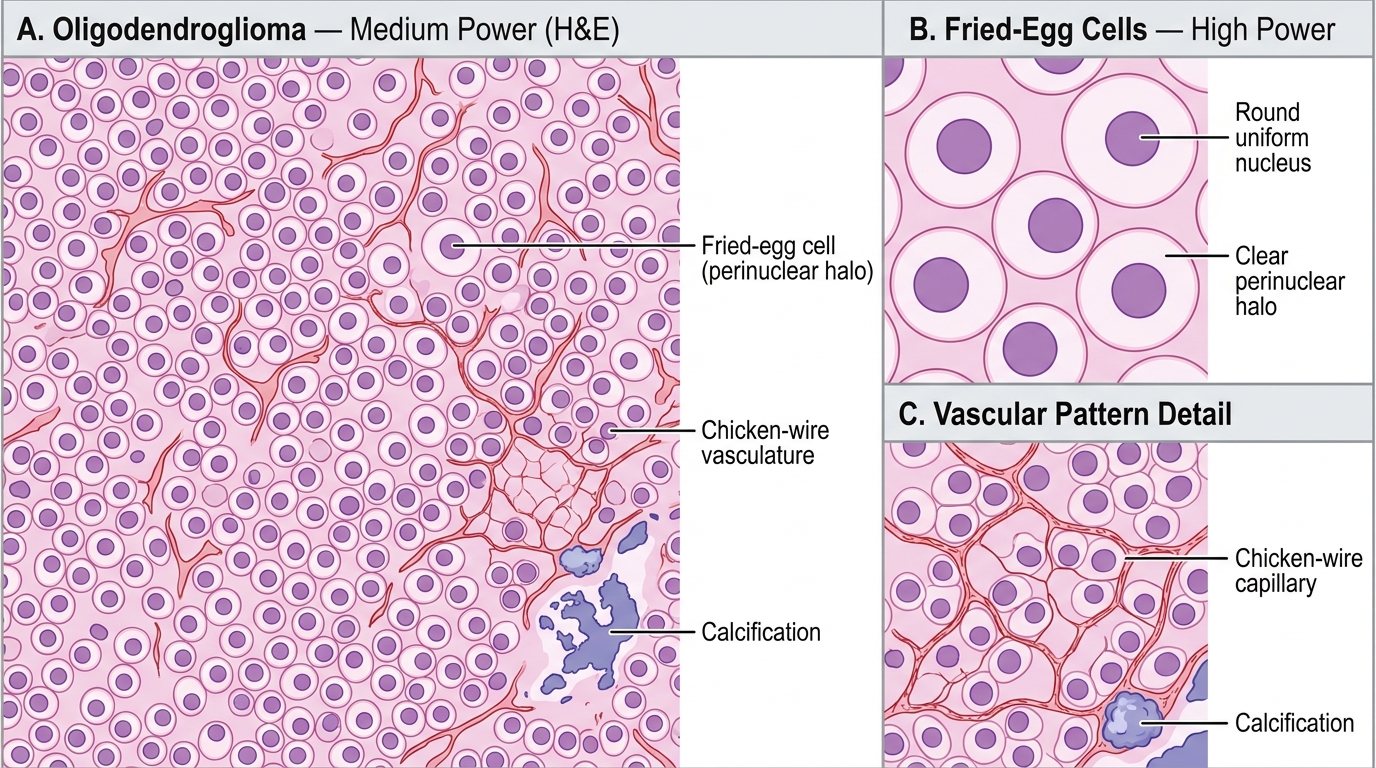
Oligodendroglioma Histology — Fried-Egg Cells, Chicken-Wire Vasculature, and Calcification
Ependymoma:
• Arises from ependymal cells lining ventricles and spinal canal. Peak: children and young adults.
• Location: Intracranial ependymomas — 4th ventricle (children); Spinal ependymomas — filum terminale/conus medullaris (adults, most common spinal cord tumor).
• Microscopy — two characteristic structures:
1. Perivascular pseudorosettes — tumor cells arranged radially around blood vessels with a fibrillary anucleate zone (most common).
2. True ependymal rosettes — columnar cells arranged around a central lumen (less common but pathognomonic).
• RELA fusion — important in Grade 3 supratentorial ependymoma (poor prognosis).
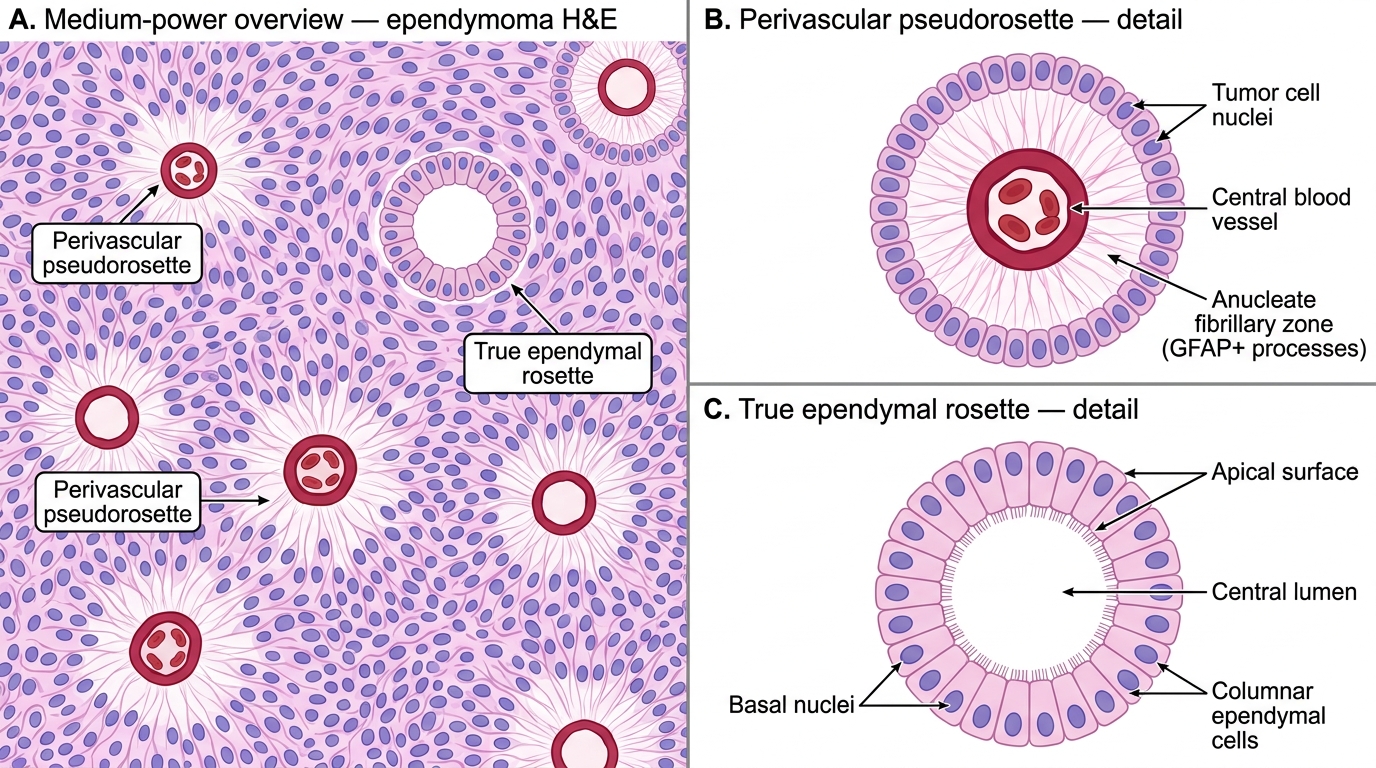
Ependymoma — Perivascular Pseudorosettes and True Ependymal Rosettes (H&E, Medium & High Power)
CLINICAL PEARL
Molecular markers in glioma — 3 you MUST know for exams:
- IDH mutation → present in low-grade gliomas (Grade 2–3) and secondary GBM → BETTER prognosis vs IDH-wild type (which is primary GBM, worse prognosis). Think: IDH-mutant = Improving/better prognosis.
- 1p/19q codeletion → defines oligodendroglioma; associated with better chemosensitivity. Codeletion + IDH mutation = textbook oligodendroglioma.
- MGMT methylation → predicts response to temozolomide in GBM. Ask: is the tumor's DNA-repair enzyme silenced? If yes, chemotherapy works better.
Exam trap: WHO 2021 now requires molecular markers (IDH, 1p/19q) to diagnose glioma types — histology alone is insufficient for classification. A tumor with 'fried-egg' histology but no 1p/19q codeletion is NOT an oligodendroglioma by current WHO criteria.