Page 5 of 16
PA34.1-3 | CNS Infections & Tumors — SDL Guide (Part 5)
Meningioma
Meningioma is the most common benign intracranial tumor (and most common intracranial tumor overall, surpassing even GBM in frequency). WHO Grade 1 in 90% of cases.
Origin: Arachnoid cap cells (meningothelial cells) of the arachnoid mater.
Epidemiology: More common in women (2:1) especially in the 40–60-year age group. Association with breast cancer (hormone receptor sharing). Risk factor: ionising radiation, NF2 mutation.
Location: Parasagittal (adjacent to superior sagittal sinus), sphenoid wing, olfactory groove, cerebellopontine angle, spinal cord. They are extra-axial (outside brain parenchyma) — this is key; it means they compress the brain rather than infiltrate it, making complete surgical resection often curative.
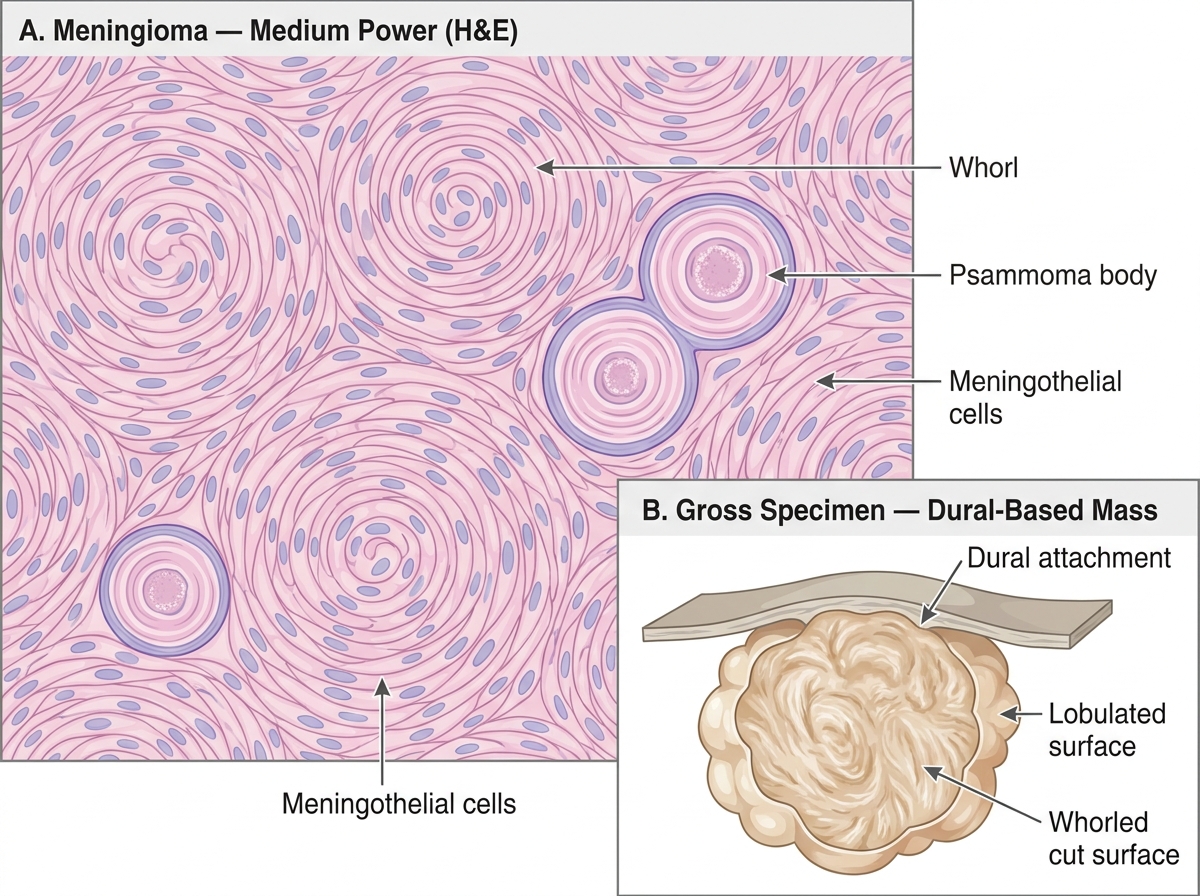
Gross pathology: Well-demarcated, lobulated, firm, grey-white mass attached to the dura. Cut surface: whorled appearance. Sand-like gritty areas (calcification = psammoma bodies).
Microscopy — characteristic features:
• Whorls of meningothelial cells (concentric layers of cells).
• Psammoma bodies — laminated concentric calcified structures (calcified whorls). Presence of psammoma bodies is nearly pathognomonic.
• Syncytial pattern — cells with indistinct cell borders.
• Elongated/spindle cells in fibroblastic variant.
NF2 gene mutation (on chromosome 22q12) — loss of merlin protein — underlying in 40–60% of meningiomas; also responsible for bilateral vestibular schwannomas in NF2 syndrome.
Meningioma: Histology and Gross Pathology
Medulloblastoma and Schwannoma
Medulloblastoma:
- Most common malignant brain tumor in children (peak age 5–9 years). WHO Grade 4. Arises in the cerebellum (midline vermis in children, lateral hemisphere in adults/adolescents).
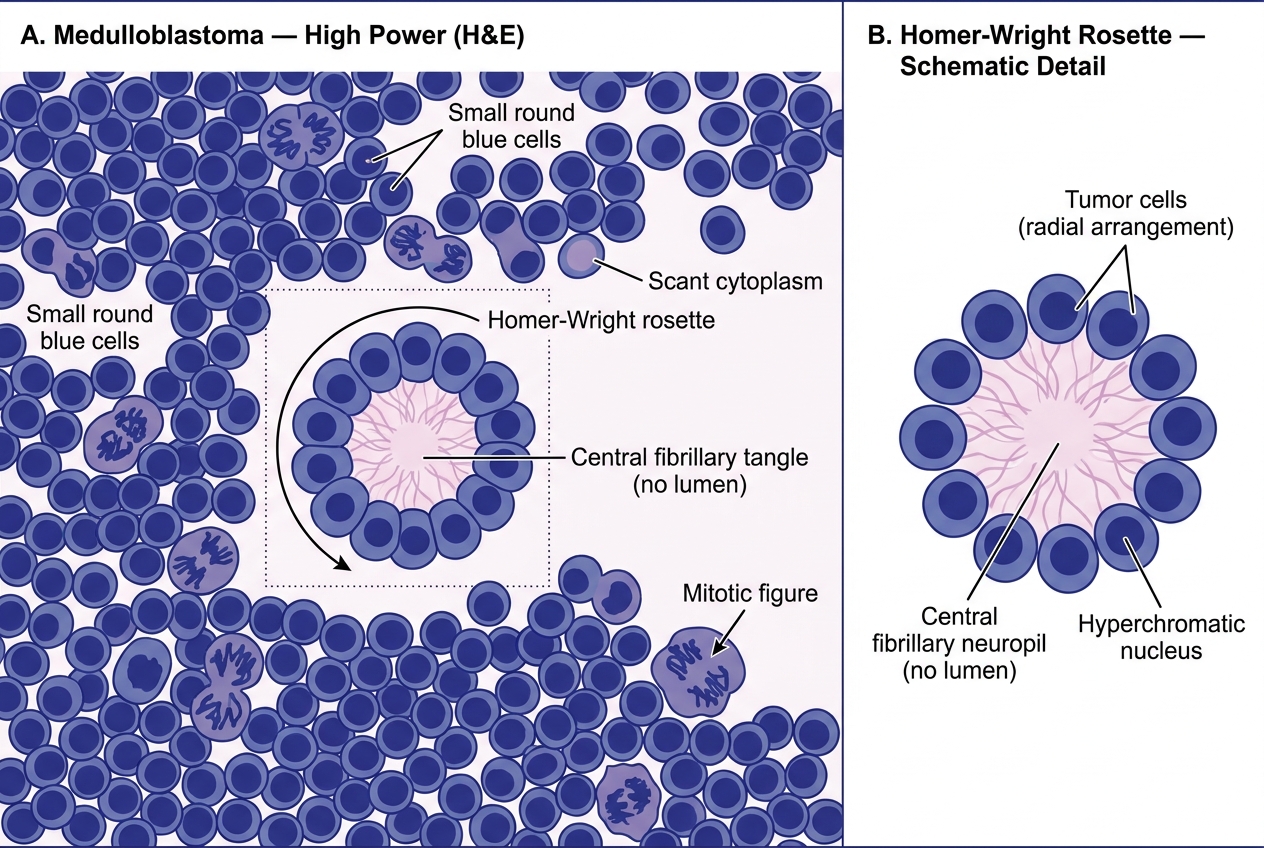
- Histology: Dense sheets of small, round, hyperchromatic blue cells (SRBCT — small round blue cell tumor). Homer-Wright rosettes — tumor cells arranged around a central neuropil fibrillary tangle (not a true lumen). Abundant mitoses; necrosis.
- Molecular subtypes (WHO 2021): WNT-activated (best prognosis), SHH-activated (intermediate), Group 3, Group 4 — determines treatment intensity.
- Spread: Via CSF → drop metastases along spinal cord (must stage with spinal MRI). Also invades 4th ventricle → obstructive hydrocephalus.
- Treatment: surgical resection + craniospinal radiotherapy + chemotherapy. 5-year survival ~70% with current therapy.
Medulloblastoma Histology — High Power with Homer-Wright Rosette
Schwannoma:
- Arises from Schwann cells (myelinating cells of peripheral and cranial nerves). WHO Grade 1.
- Most common location: Vestibular nerve (CN VIII) at the cerebellopontine angle → acoustic neuroma / vestibular schwannoma. Presents: progressive unilateral sensorineural hearing loss, tinnitus, balance disturbance.
- NF2 gene (chromosome 22) — bilateral vestibular schwannomas are pathognomonic of Neurofibromatosis Type 2 (NF2).
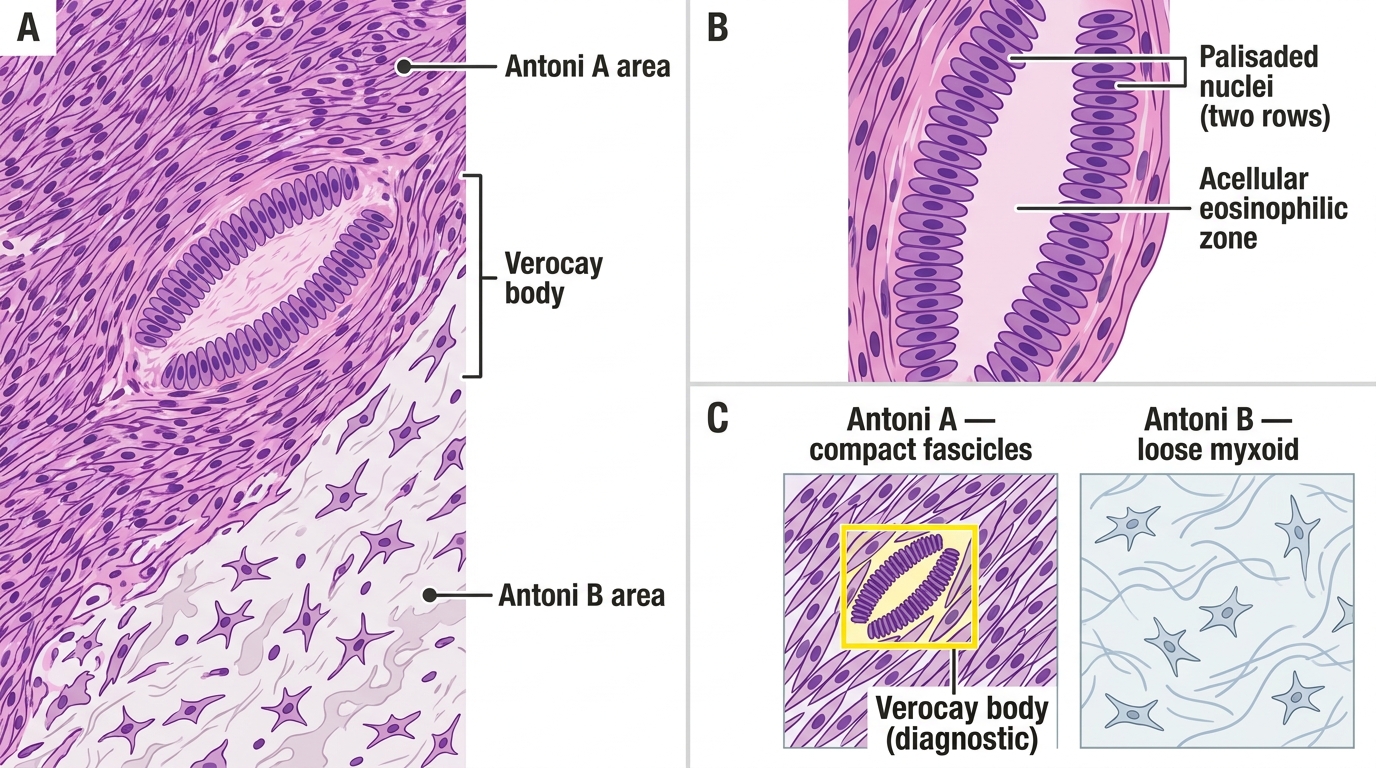
- Microscopy: Alternating Antoni A (hypercellular, spindled cells in palisades — Verocay bodies) and Antoni B (hypocellular, loose/myxoid) areas. Verocay bodies = two rows of palisaded nuclei around eosinophilic material.
- Encapsulated; does NOT infiltrate nerve fibres (compresses them) → surgical cure possible.
Schwannoma Histology: Antoni A and Antoni B Areas with Verocay Body
Raised Intracranial Pressure and Cerebral Herniation
CNS tumors (and severe meningitis) cause raised intracranial pressure (ICP), which produces characteristic clinical features and can cause fatal herniation.
Normal ICP: 5–15 mmHg.
Causes of raised ICP in CNS disease:
• Mass lesion (tumor, haematoma, abscess) — space-occupying effect
• Cerebral oedema — vasogenic (breakdown of BBB) or cytotoxic (cell swelling)
• Hydrocephalus — impaired CSF drainage
• Hyperaemia — increased cerebral blood volume
Clinical features of raised ICP (the Cushing triad for severe elevation):
• Headache — worse in the morning (recumbent position increases ICP during sleep), aggravated by Valsalva, coughing
• Vomiting — projectile, not preceded by nausea (direct medullary stimulation)
• Papilloedema — swelling of optic disc seen on fundoscopy (transmitted pressure along optic sheath)
• Cushing's triad (late, severe): bradycardia + hypertension + irregular respiration
Cerebral herniation syndromes:
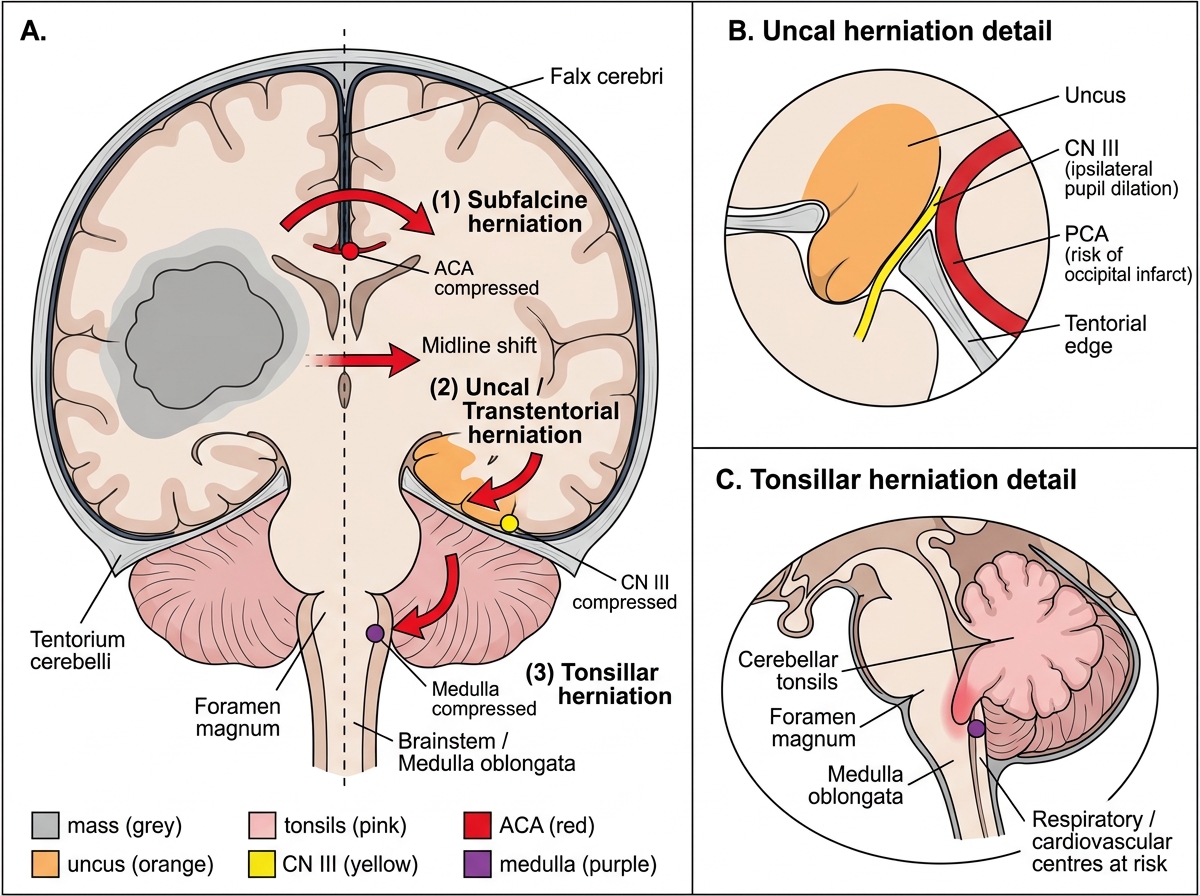
- Transtentorial (uncal) herniation — most common; medial temporal lobe (uncus) herniates through tentorial notch → compresses CN III (ipsilateral fixed, dilated pupil — 'blown pupil') + ipsilateral PCA compression (occipital lobe infarct → contralateral visual loss) + contralateral hemiplegia (cerebral peduncle compression) or ipsilateral hemiplegia (Kernohan's notch — false localising sign).
- Tonsillar herniation — cerebellar tonsils herniate through foramen magnum → medullary compression → respiratory arrest. This is why LP is dangerous with raised ICP.
- Subfalcine herniation — cingulate gyrus herniates under falx cerebri → compresses ACA → contralateral leg weakness.
Cerebral Herniation Syndromes — Coronal Section with Herniation Detail
SELF-CHECK
A 58-year-old man presents with 6 weeks of progressive right-sided weakness and headaches that are worst in the morning. MRI shows a large left frontal mass with surrounding oedema, central necrosis, and ring enhancement. Brain biopsy shows hypercellular atypical astrocytes, pseudopalisading necrosis, and microvascular proliferation. MGMT promoter testing is ordered. What is the diagnosis, and what is the clinical significance of MGMT methylation status?
A. Oligodendroglioma — MGMT methylation predicts 1p/19q codeletion status
B. Glioblastoma (IDH-wild type, WHO Grade 4) — MGMT promoter methylation predicts better response to temozolomide chemotherapy
C. Metastatic carcinoma — MGMT methylation guides targeted biological therapy
D. Ependymoma — MGMT methylation predicts RELA fusion status and prognosis
Reveal Answer
Answer: B. Glioblastoma (IDH-wild type, WHO Grade 4) — MGMT promoter methylation predicts better response to temozolomide chemotherapy
Correct: Glioblastoma. The histological triad (pseudopalisading necrosis + microvascular proliferation + hypercellular pleomorphic astrocytic tumor) is diagnostic of GBM (WHO Grade 4). MGMT encodes a DNA-repair enzyme. When the MGMT promoter is methylated, the gene is silenced → the tumor cannot repair alkylating-agent-induced DNA damage → better response to temozolomide (the standard chemotherapy). MGMT-methylated GBM patients have median survival ~21 months vs ~12 months for unmethylated. This is the primary biomarker tested in clinical practice for treatment planning. Note: ring enhancement on MRI reflects the pseudopalisading necrosis and BBB breakdown at the tumour periphery.