Page 9 of 16
PA35.1 | Retinoblastoma & Neuro-Ophthalmic Morphology — SDL Guide (Part 3)
CNS Morphology Walk-Through — Gliomas and Meningioma
Glioblastoma (GBM) — WHO Grade 4 Astrocytoma:
• Gross: Highly variable — haemorrhage, necrosis, cystic areas give a 'butterfly' appearance when crossing the corpus callosum. Poorly demarcated from normal brain. Cut surface shows variegated yellow necrosis and red haemorrhage.
• Micro: The three diagnostic hallmarks of GBM:
1. Pseudopalisading necrosis — the pathognomonic feature. Elongated hyperchromatic tumor nuclei palisade (align in parallel rows) around zones of necrosis, forming a picket-fence pattern. This represents hypoxia-induced migration of cells away from the necrotic core.
2. Glomeruloid microvascular proliferation — tufts of proliferating endothelial and smooth muscle cells within vessels, forming complex structures resembling renal glomeruli. Driven by VEGF secreted by the hypoxic tumor.
3. Nuclear pleomorphism and mitoses — extreme variation in nuclear size, multinucleated giant cells, numerous mitoses.
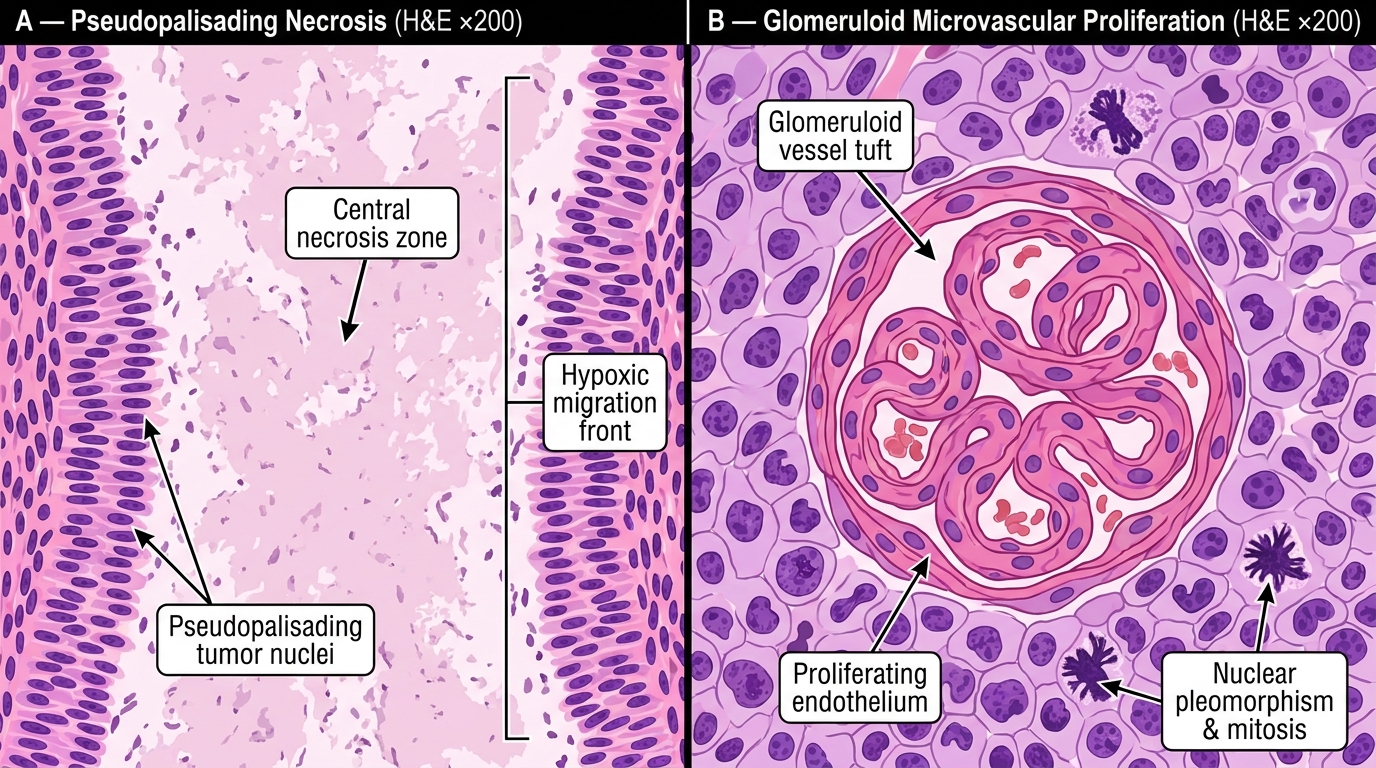
GBM Diagnostic Hallmarks — Pseudopalisading Necrosis and Glomeruloid Microvascular Proliferation (H&E)
Meningioma:
• Origin: Arachnoid cap cells (meningothelial cells) of the leptomeninges. Most common benign intracranial tumor in adults.
• Gross: Well-demarcated, bosselated (nodular surface), rubbery mass attached to dura. Does not invade brain parenchyma (pushes it). Cut surface: grey-white, gritty (from calcification).
• Micro: Multiple patterns, but the two you must know:
1. Whorled pattern — onion-skin concentric arrangements of meningothelial cells, giving the characteristic spiral ('whorl') appearance.
2. Psammoma bodies — calcified concentric lamellations within the whorls (named after psammos = sand). They result from progressive calcification of the whorl centres. Pathognomonic when numerous.
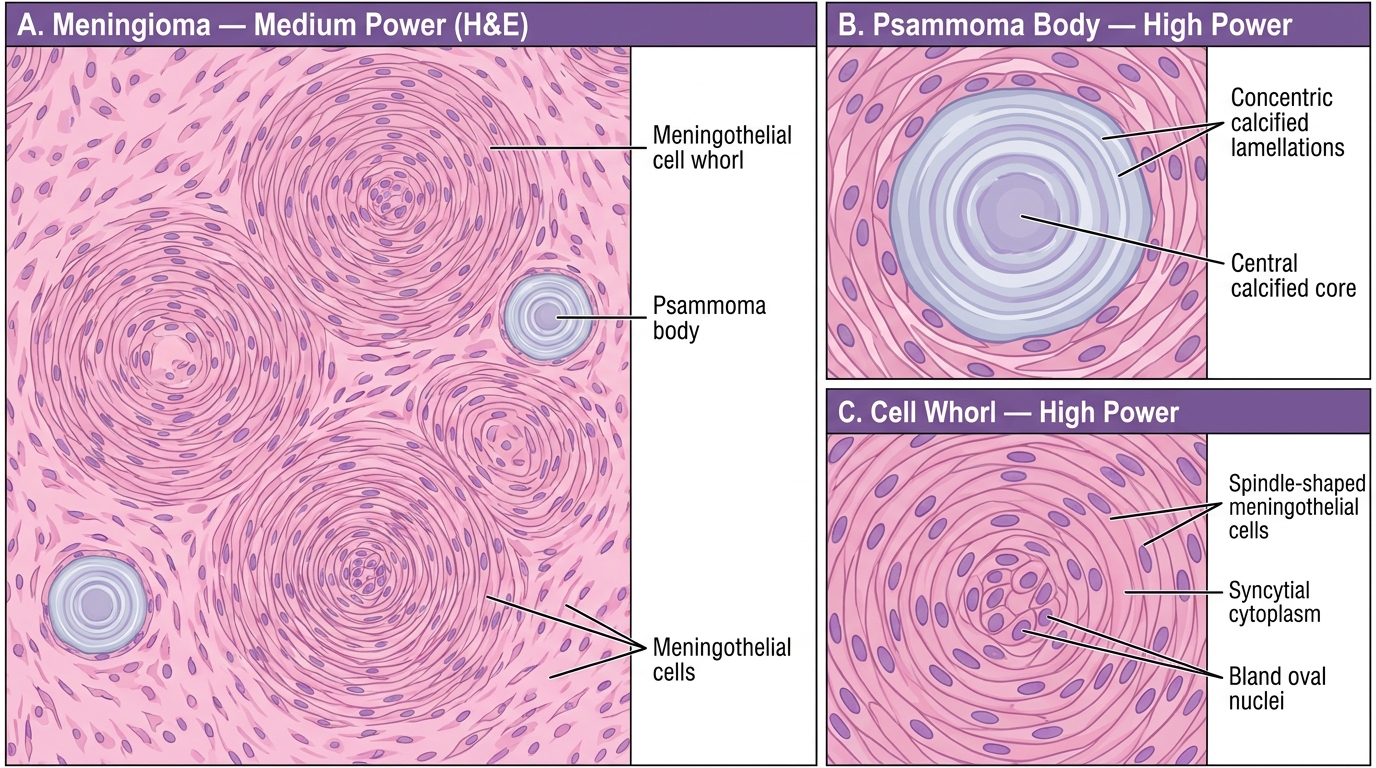
Meningioma Histology — Whorling Pattern and Psammoma Bodies (H&E)
Oligodendroglioma — the 'fried-egg' pattern:
- Origin: Oligodendrocytes
- WHO Grade 2 or 3; IDH-mutant and 1p/19q co-deleted by molecular definition
- Micro: The classic appearance (artefactual from formalin fixation): round nuclei surrounded by a clear halo of cytoplasm — the 'fried-egg' cell or perinuclear halo. Cells are arranged in a regular, monotonous sheet. Delicate 'chicken-wire' vasculature (thin-walled capillaries in a hexagonal/branching pattern) in the background. Calcification common (cortical/perivascular).
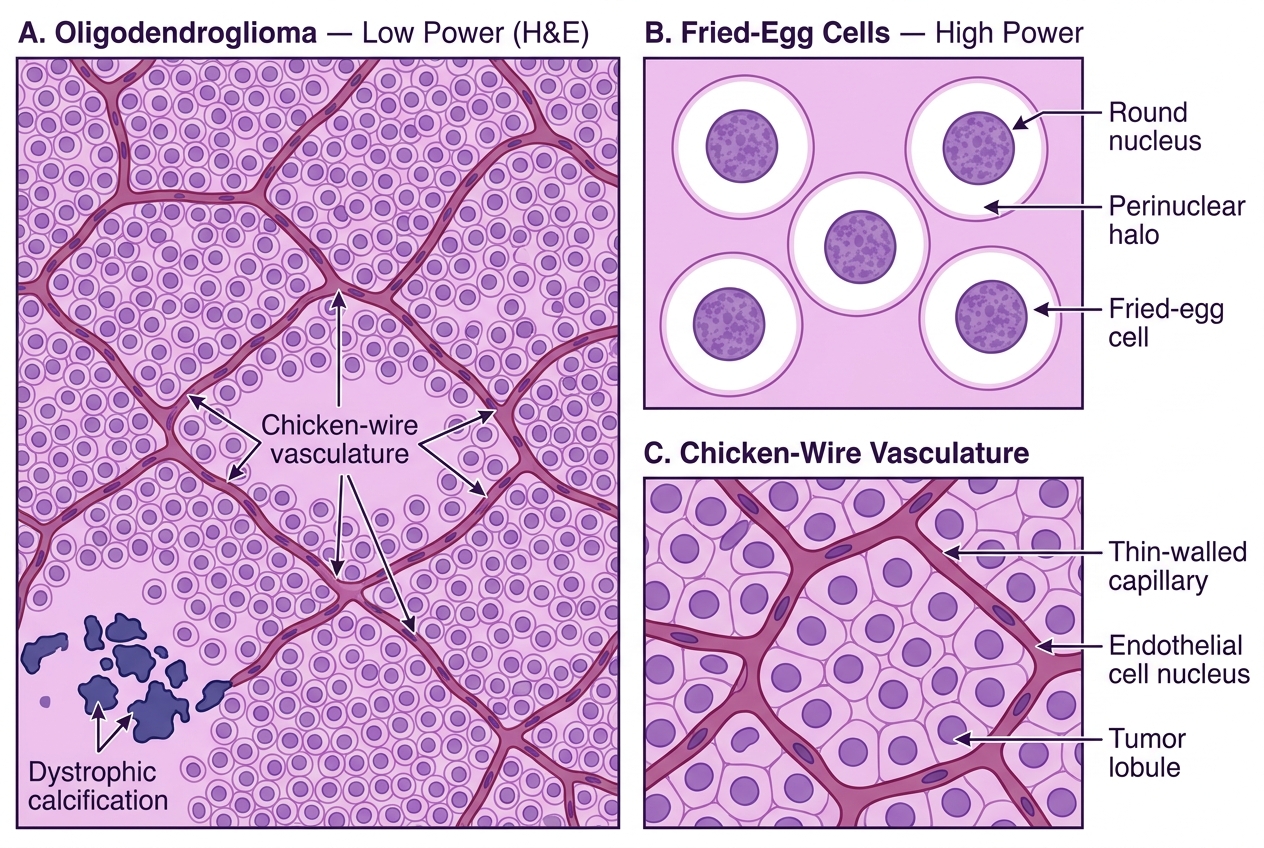
Oligodendroglioma — H&E Histology: Fried-Egg Cells and Chicken-Wire Vasculature
CNS Morphology Walk-Through — Embryonal Tumors and Nerve Sheath
Medulloblastoma:
• Origin: Cerebellar granule cell precursors (most cases); posterior fossa, midline vermis in children
• WHO Grade 4 embryonal tumor
• Micro: Dense sheets of small round blue cells (SRBC) — hyperchromatic nuclei, scant cytoplasm, high N:C ratio, brisk mitoses. Two structural patterns:
1. Homer-Wright rosettes (neuroblastic rosettes) — ring of cells around a central fibrillary neuropil core (no true lumen). Represent neuronal differentiation.
2. Desmoplastic/nodular pattern — nodules of less cellular, 'pale island' reticulin-free zones (differentiated) surrounded by dense reticulin-rich zones (undifferentiated).
• IHC: Synaptophysin positive (neuronal differentiation), GFAP negative or focally positive
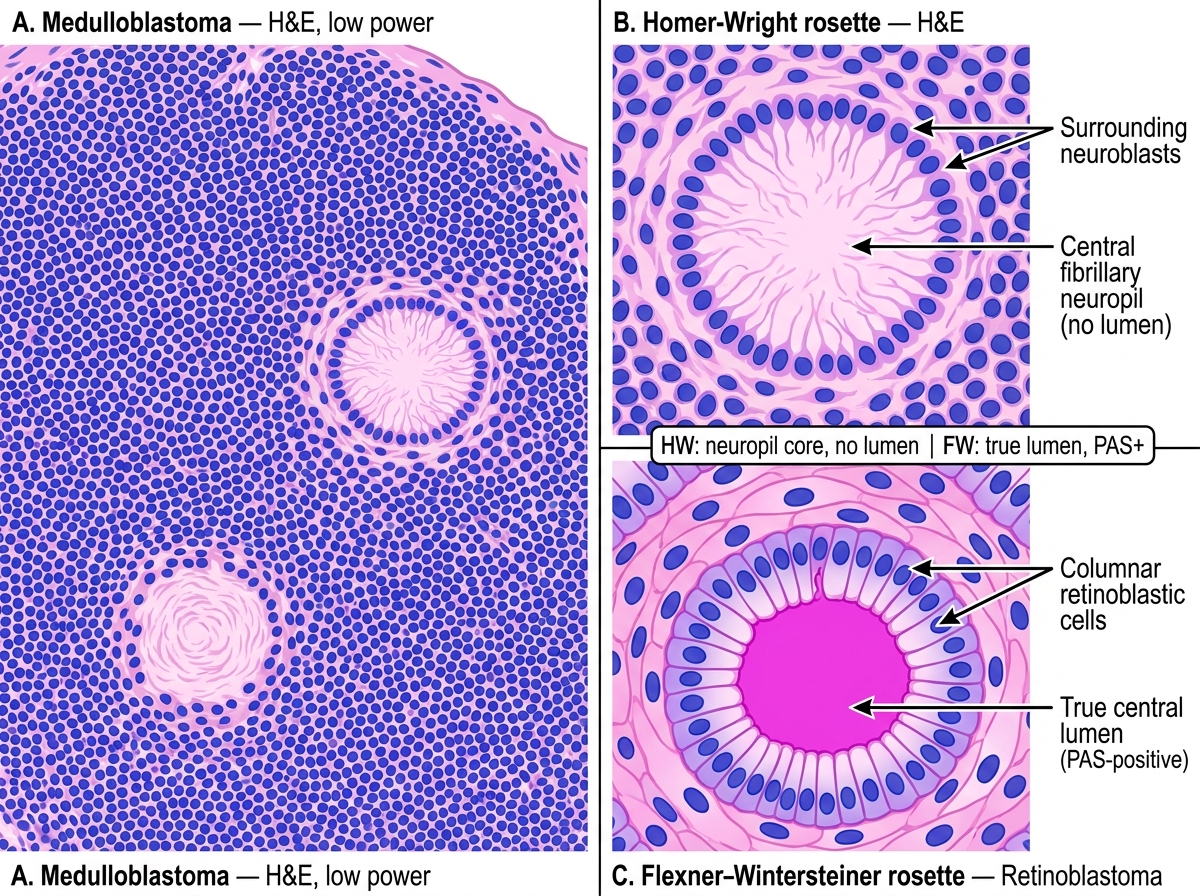
Rosette Types in Embryonal Tumours — Homer-Wright vs Flexner-Wintersteiner
Schwannoma:
• Origin: Schwann cells of peripheral nerve sheath; WHO Grade 1; associated with NF2 (bilateral vestibular schwannomas = acoustic neuromas)
• Micro: Two alternating tissue patterns that define schwannoma:
1. Antoni A — hypercellular areas; elongated spindle cells with pale eosinophilic cytoplasm arranged in palisading fascicles (parallel aligned nuclei). Verocay bodies = compact parallel rows of palisading nuclei flanking an anuclear eosinophilic zone (fibrillary processes). The Verocay body is the pathognomonic feature.
2. Antoni B — hypocellular areas; loose, myxoid (pale, watery) background with scattered stellate cells; disorganised, feels 'wet' on the slide; may have cystic change and hyalinised vessels.
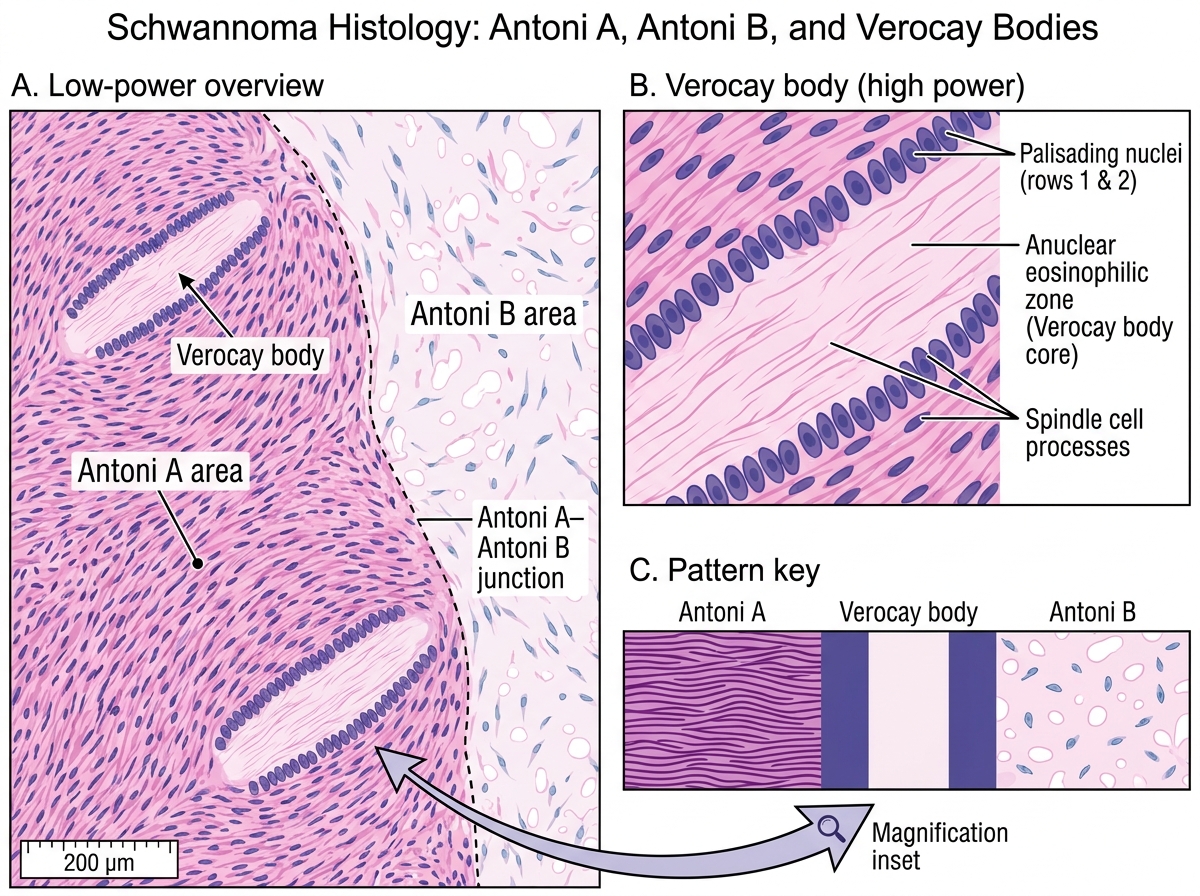
Schwannoma Histology (H&E): Antoni A, Verocay Bodies, and Antoni B Areas
Master recognition table for CNS/eye practical:
| Lesion | Key cells | Key pattern/structure | Special feature |
|---|---|---|---|
| Bacterial meningitis | Neutrophils | Subarachnoid exudate | Gram-positive diplococci / gram-negative bacilli |
| TB meningitis | Lymphocytes, epithelioid cells, Langhans giant cells | Basal granulomas + caseation | AFB on ZN stain |
| Glioblastoma | Pleomorphic astrocytes | Pseudopalisading necrosis + glomeruloid vessels | IDH-wildtype, GFAP+, EGFR amplification |
| Oligodendroglioma | Oligodendrocyte-like cells | Fried-egg cells + chicken-wire vessels | IDH-mutant, 1p/19q co-deletion |
| Meningioma | Meningothelial cells | Whorls + psammoma bodies | EMA+, arachnoid attachment |
| Medulloblastoma | SRBC | Homer-Wright rosettes (no lumen) | Posterior fossa, synaptophysin+ |
| Schwannoma | Spindle (Schwann) cells | Antoni A/B + Verocay bodies | S100+, encapsulated |
| Retinoblastoma | SRBC | Flexner-Wintersteiner rosettes (true lumen) + necrosis + calcification | RB1 loss, synaptophysin+, leukocoria |
CLINICAL PEARL
The small-round-blue-cell differential in a child's tumor is a classic exam and clinical challenge. When you see dense sheets of small hyperchromatic cells with scant cytoplasm, your differential should include: medulloblastoma, retinoblastoma, neuroblastoma, Ewing sarcoma / PNET, and Wilms tumor. The site is your first discriminator — retinoblastoma is intraocular, medulloblastoma is posterior fossa/cerebellar, neuroblastoma is adrenal/paraspinal, Ewing is bone/soft tissue. The rosette type narrows further: Flexner-Wintersteiner (true lumen) = retinoblastoma (photoreceptor differentiation); Homer-Wright (no lumen, neuropil) = medulloblastoma/neuroblastoma (neuronal differentiation). IHC helps: synaptophysin+ is shared; GFAP is typically negative in all of these embryonal tumors; CD99 (membranous) + FLI-1 = Ewing.
SELF-CHECK
A 3-year-old girl presents with leukocoria in the left eye. Enucleation is performed. Histology shows sheets of small round blue cells with rosettes having a central lumen bounded by a PAS-positive membrane. Which rosette type is present, and what does its central lumen represent?
A. Homer-Wright rosette — central fibrillary neuropil representing neuronal differentiation
B. Flexner-Wintersteiner rosette — central lumen representing photoreceptor (cone-like) differentiation
C. Pseudorosette — cells arranged around a blood vessel
D. Fleurette — cells projecting bouquet-like processes outward
Reveal Answer
Answer: B. Flexner-Wintersteiner rosette — central lumen representing photoreceptor (cone-like) differentiation
Flexner-Wintersteiner rosettes are the specific rosette of retinoblastoma. The ring of columnar cells surrounds a true central lumen lined by a PAS-positive glycoprotein-rich membrane, analogous to the subretinal space. This structure represents photoreceptor (cone-like) differentiation. Homer-Wright rosettes (no true lumen; central neuropil) are seen in medulloblastoma, neuroblastoma, and also retinoblastoma — but the presence of a PAS-positive central lumen confirms the Flexner-Wintersteiner type. Pseudorosettes form around blood vessels (seen in ependymoma). Fleurettes represent the most differentiated end of the retinoblastoma spectrum.
SELF-CHECK
A 28-year-old man with a history of bilateral retinoblastoma treated in childhood presents with pain and swelling in his right femur. X-ray shows a lytic lesion in the diaphysis. What is the most likely diagnosis, and why is it related to his retinoblastoma history?
A. Osteosarcoma arising from loss of the RB1 tumor suppressor gene in bone cells
B. Fibrous dysplasia — a benign condition unrelated to retinoblastoma
C. Ewing sarcoma — associated with EWSR1-FLI1 translocation unrelated to RB1
D. Metastatic retinoblastoma to bone from the primary eye tumor
Reveal Answer
Answer: A. Osteosarcoma arising from loss of the RB1 tumor suppressor gene in bone cells
Individuals with germline (hereditary) RB1 mutations are at significantly elevated risk for second malignancies — most commonly osteosarcoma. The RB1 protein regulates cell cycle progression in all tissues, not just the retina. Loss of pRb function in osteoblast precursors predisposes to osteosarcoma, which typically occurs in the second to third decade of life. The risk is further increased if the patient received external beam radiotherapy to the orbit in childhood. This is the classic 'second cancer' of hereditary retinoblastoma. Metastatic retinoblastoma to bone (Option D) would be extremely unusual decades after successful treatment of the primary tumor.
SELF-CHECK
On a histology slide from the posterior fossa of a 7-year-old, you see dense sheets of small round blue cells with a fibrillary neuropil core at the centre of cellular rosettes. There is NO true central lumen and NO calcification. The tumor is in the cerebellar vermis. What is the most likely diagnosis?
A. Retinoblastoma — metastatic to the cerebellum
B. Oligodendroglioma — fried-egg cells with chicken-wire vasculature
C. Medulloblastoma — Homer-Wright rosettes in a cerebellar embryonal tumor
D. Schwannoma — Antoni A pattern with Verocay bodies
Reveal Answer
Answer: C. Medulloblastoma — Homer-Wright rosettes in a cerebellar embryonal tumor
Medulloblastoma is the most common malignant brain tumor of childhood and arises in the posterior fossa (cerebellar vermis in children). The histological hallmarks are sheets of small round blue cells and Homer-Wright rosettes — ring of cells around a central fibrillary neuropil core WITHOUT a true central lumen. This distinguishes it from retinoblastoma (which has Flexner-Wintersteiner rosettes with a true PAS-positive central lumen). Calcification is characteristic of retinoblastoma, not medulloblastoma. Oligodendroglioma has fried-egg cells and chicken-wire vasculature, not rosettes. Schwannoma is a nerve sheath tumor with Antoni A/B patterns and Verocay bodies.