Page 8 of 16
PA35.1 | Retinoblastoma & Neuro-Ophthalmic Morphology — SDL Guide (Part 2)
Microscopic Morphology — The Rosettes You Must Know
The histological hallmark of retinoblastoma is sheets of small round blue cells (SRBC) — undifferentiated, hyperchromatic nuclei with scant cytoplasm — punctuated by areas of necrosis and calcification, and by three types of rosette-like structures that represent varying degrees of photoreceptor differentiation.
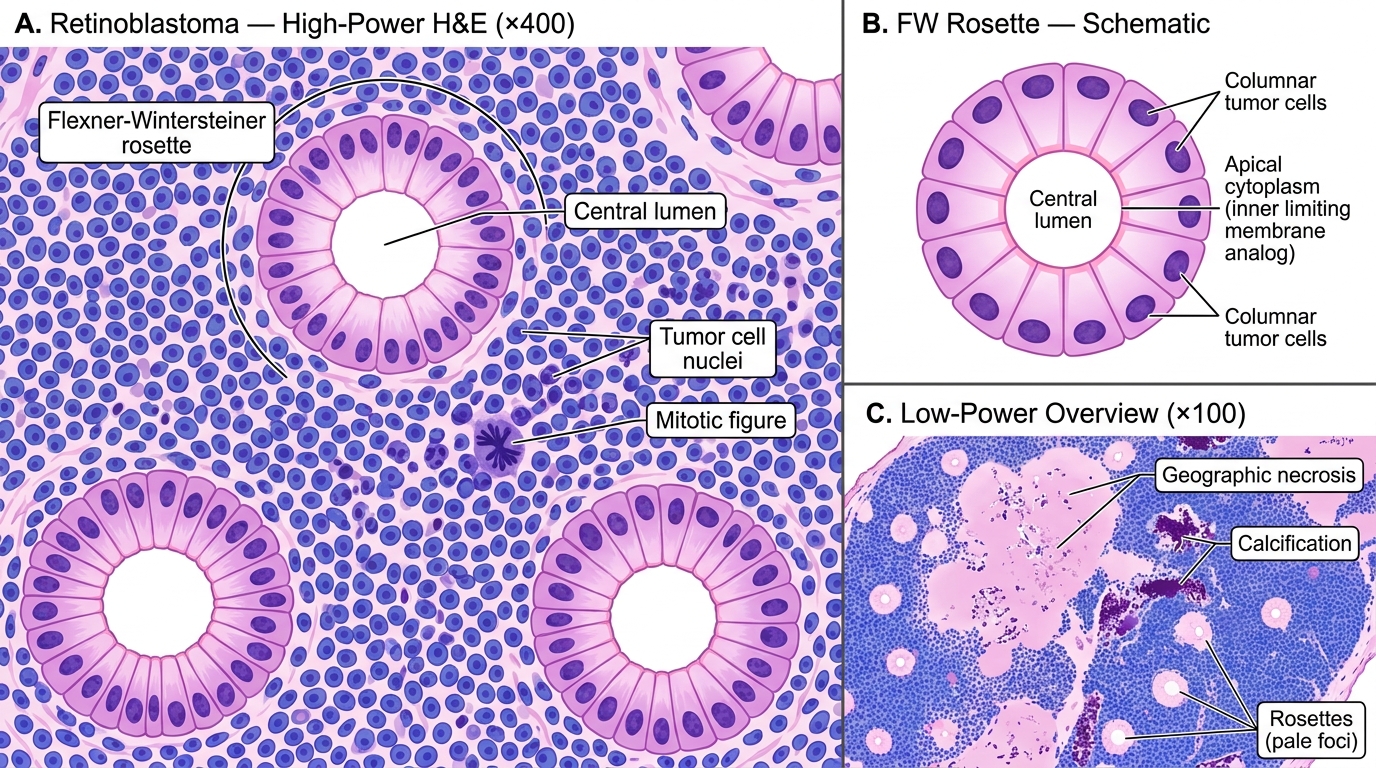
Retinoblastoma Histology — Flexner-Wintersteiner Rosettes (H&E)
Three rosette types — master comparison table:
| Feature | Flexner-Wintersteiner Rosette | Homer-Wright Rosette | Fleurette |
|---|---|---|---|
| Structure | Ring of columnar cells around a true central lumen | Ring of cells around neuropil/fibrillary core (no true lumen) | Clusters of cells with photoreceptor-like bouquet processes projecting outward |
| Central lumen | Present (PAS-positive, bounded by terminal bars / apical junctions) | Absent — centre is fibrillary neuropil | Absent — cells project externally |
| Represents | Photoreceptor differentiation (cone-like) | Primitive neuronal differentiation | Advanced photoreceptor differentiation; benign retinocytoma end of spectrum |
| Tumor | Retinoblastoma (specific) | Retinoblastoma, medulloblastoma, neuroblastoma, pineoblastoma | Retinoblastoma (fleurette-rich variants are less aggressive) |
| PAS stain | Lumen is PAS-positive (glycoprotein membrane material) | Negative | Not applicable |
| Exam tip | Central lumen = Flexner-Wintersteiner | No lumen, fibrils = Homer-Wright | Bouquets = fleurettes |
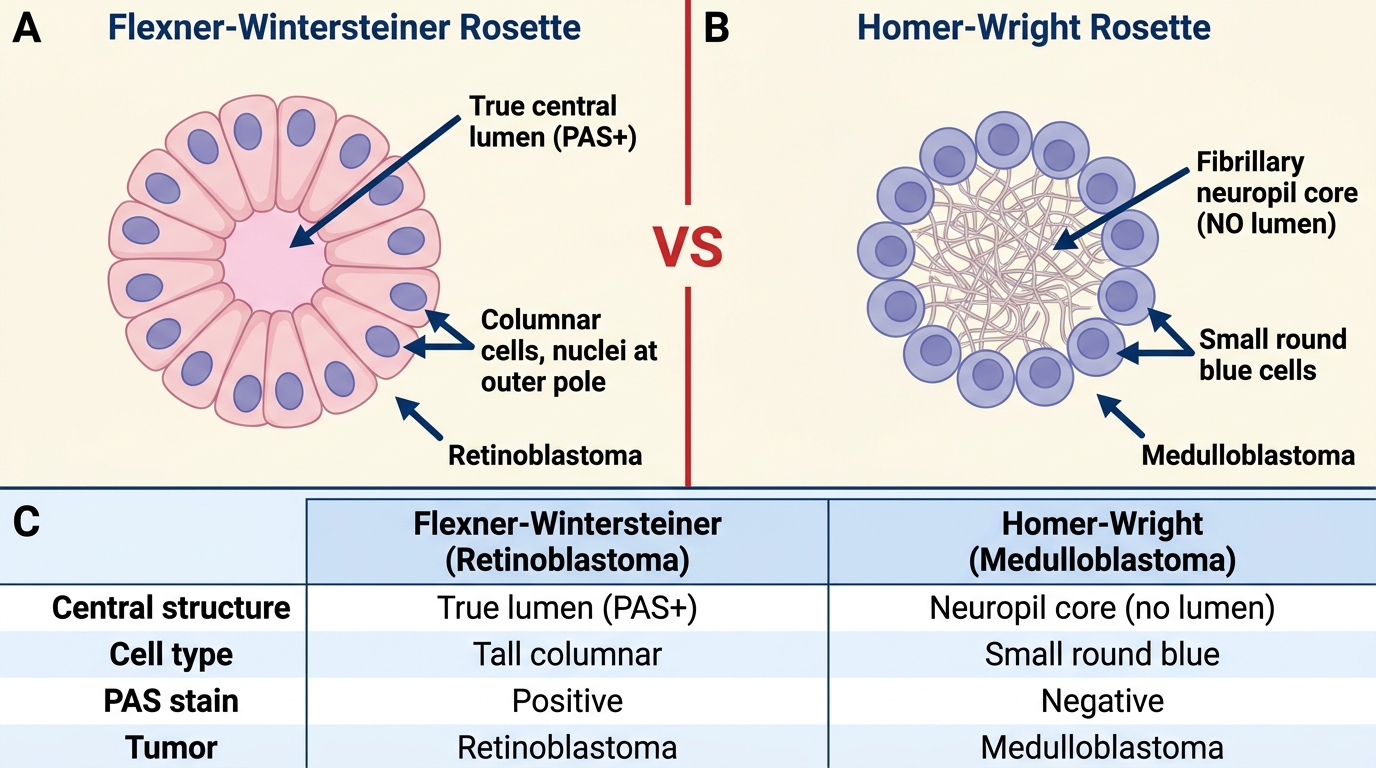
Flexner-Wintersteiner vs Homer-Wright Rosettes: Diagnostic Comparison
Additional morphological features:
• Necrosis and calcification — characteristic; necrosis surrounds vessels (cells farther from vessels die first), calcification is dystrophic. Radiologically, calcification within an intraocular mass in a child is pathognomonic for retinoblastoma.
• Perivascular cuffing — viable tumor cells form collars around blood vessels (Hortega / 'sleeve' pattern) while distant cells necrose.
• High mitotic rate — numerous mitotic figures reflect rapid proliferation.
• Basophilic DNA deposits — freed nuclear chromatin deposits on vessel walls (characteristic of rapidly necrotic tumors).
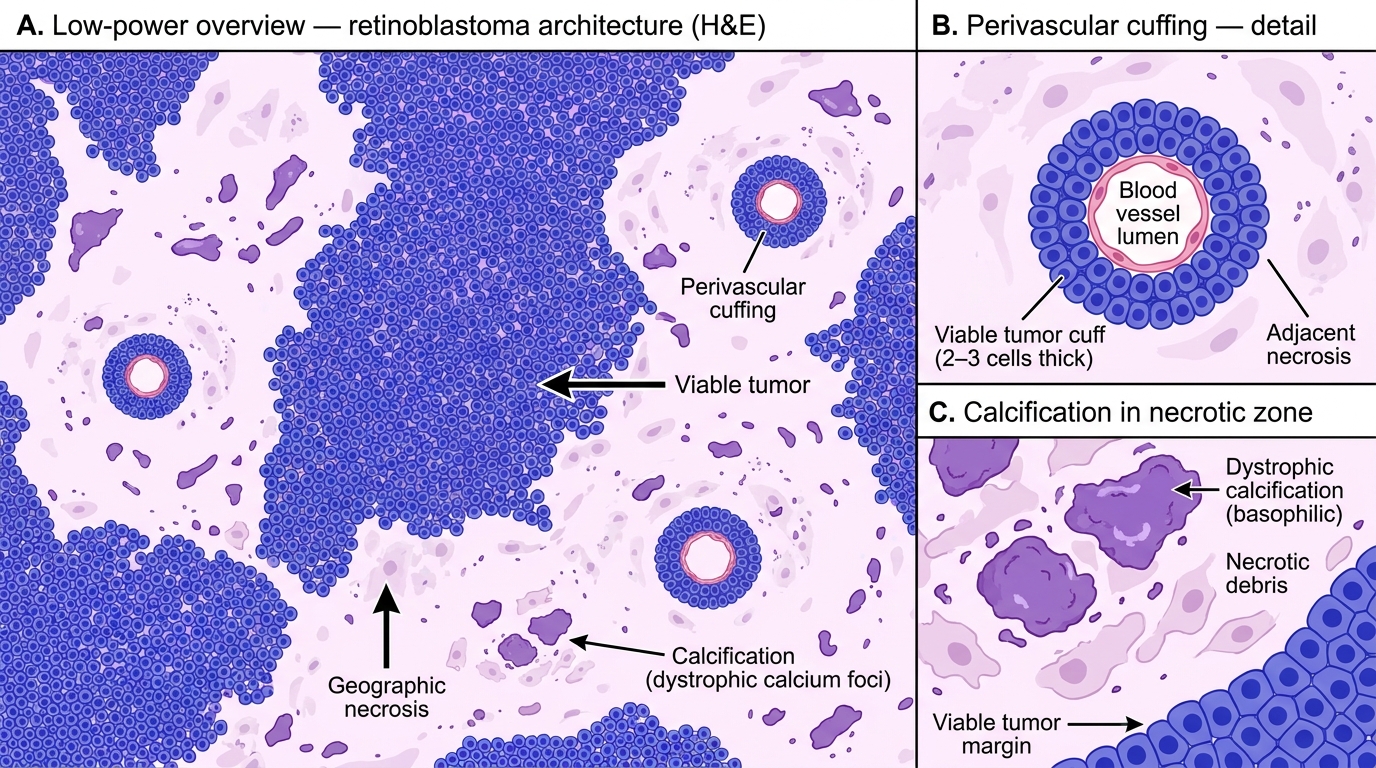
Retinoblastoma — Low-power Histological Architecture (H&E)
Spread, Sequelae, and Complications
Routes of spread — three pathways to know:
1. Local extension within the eye:
• Endophytic: vitreous seeding — detached tumor cell clusters float in vitreous ('snowballs'), making local treatment more difficult.
• Exophytic: subretinal seeding, retinal detachment.
• Anterior extension to iris, ciliary body, trabecular meshwork → raised IOP → secondary glaucoma → buphthalmos (cow's eye — enlarged globe from chronic raised pressure in a child whose sclera is still pliable).
2. Direct (trans-scleral/optic nerve) extension:
• Optic nerve invasion — the most critical prognostic factor assessed on pathology report. Tumor cells track along the optic nerve toward the chiasm and subarachnoid space → intracranial extension → CNS disease (most feared complication).
• Choroidal invasion → scleral invasion → orbital extension.
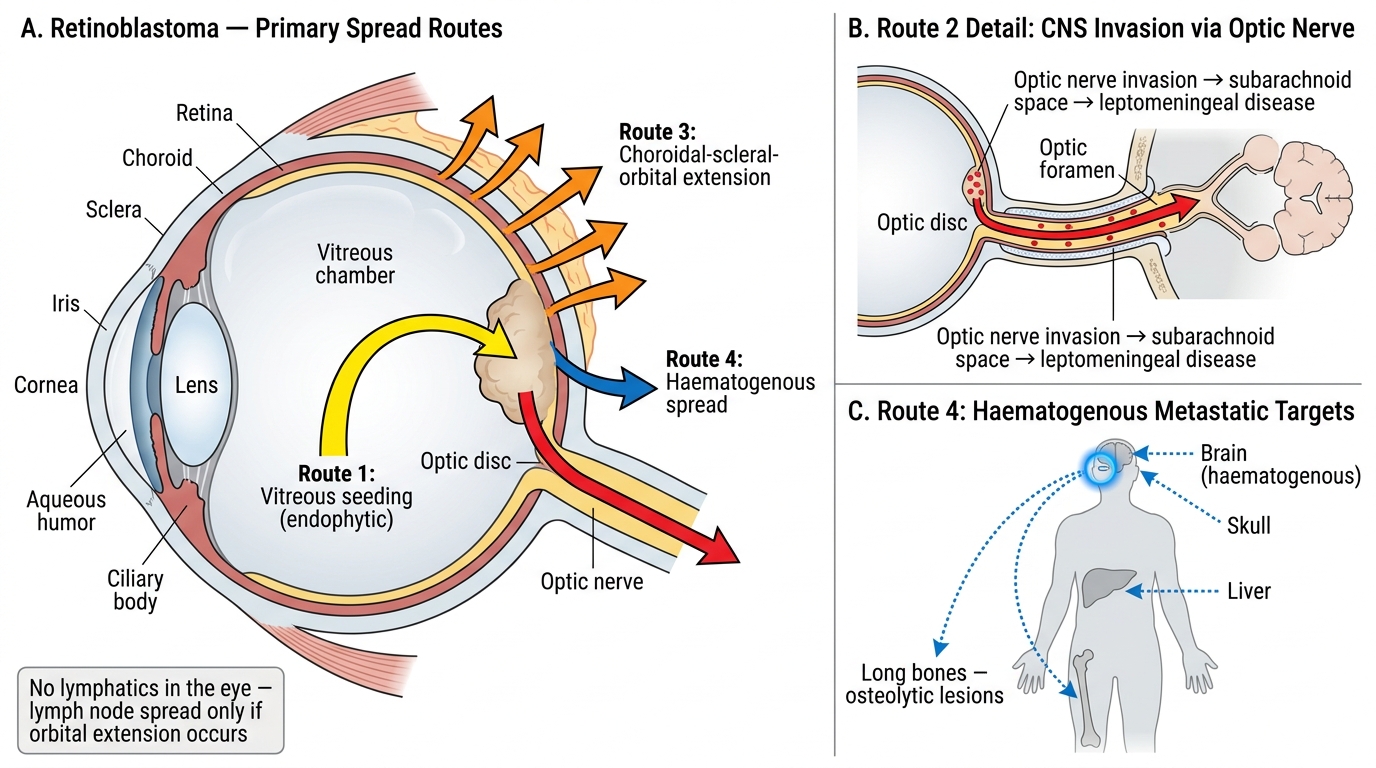
Retinoblastoma: Routes of Spread
3. Metastatic (haematogenous/lymphatic spread — late/advanced):
• Bones (long bones, skull — osteolytic lesions)
• Bone marrow
• Liver
• Lymph nodes (regional, if orbital extension has occurred — note: the eye itself has no lymphatics)
• Brain (hematogenous, distinct from optic nerve direct extension)
Sequelae and complications (exam list):
• Secondary glaucoma — raised IOP from angle infiltration or neovascularisation
• Buphthalmos — enlarged globe
• Retinal detachment — exophytic growth
• Vitreous haemorrhage
• Phthisis bulbi — calcified, shrunken end-stage eye (complete spontaneous regression, extremely rare; more common in retinocytoma — the benign counterpart)
• Orbital cellulitis mimicry — advanced necrotic tumor causes proptosis and periorbital inflammation
• CNS leptomeningeal disease — most lethal complication
• Second malignancies (hereditary RB) — osteosarcoma, STS, melanoma
Prognosis and management principles:
• Survival in intraocular disease (IIRC Groups A–C): >95% with modern treatment
• Enucleation (surgical removal of the eye) — standard for advanced unilateral disease (IIRC Groups D–E)
• Chemoreduction (systemic carboplatin/vincristine/etoposide) + focal therapy (laser, cryotherapy, brachytherapy) — globe-preserving for early bilateral disease
• Intra-arterial chemotherapy (ophthalmic artery infusion) — increasing use for advanced unilateral cases
• Prognosis worsens with: optic nerve involvement beyond the lamina cribrosa, choroidal invasion, scleral extension, vitreous seeding, orbital disease
Exam anchor: The pathology report must specifically state whether optic nerve cut margin is free — a cut margin positive for tumor cells means intracranial extension is probable and systemic chemotherapy is mandatory.
CLINICAL PEARL
Leukocoria is a medical emergency until proven otherwise. In a child under 5, a white pupillary reflex on fundoscopy or in a photograph should trigger urgent ophthalmology referral within 24 hours — never 'watch and wait.' Delayed diagnosis of even a few weeks can mean the difference between a globe-preserving outcome and enucleation. In busy primary care settings, the red reflex test (Brückner test) is a sensitive screening tool: in a darkened room, shine a direct ophthalmoscope from ~50 cm — a normal reflex is symmetric and red/orange in both eyes. Absent or white reflex in one eye = refer immediately. This test should be part of every neonatal examination, immunisation visit, and child health check.
CNS Morphology Walk-Through — Meningitis Patterns
You now enter the practical recognition walk-through — a systematic tour of every CNS and eye lesion you need to identify from slides. For each lesion, focus on three questions: (1) Where are the abnormal cells? (2) What is their shape/arrangement? (3) What background or architectural pattern is present?
Meningitis — two forms, contrasting patterns:
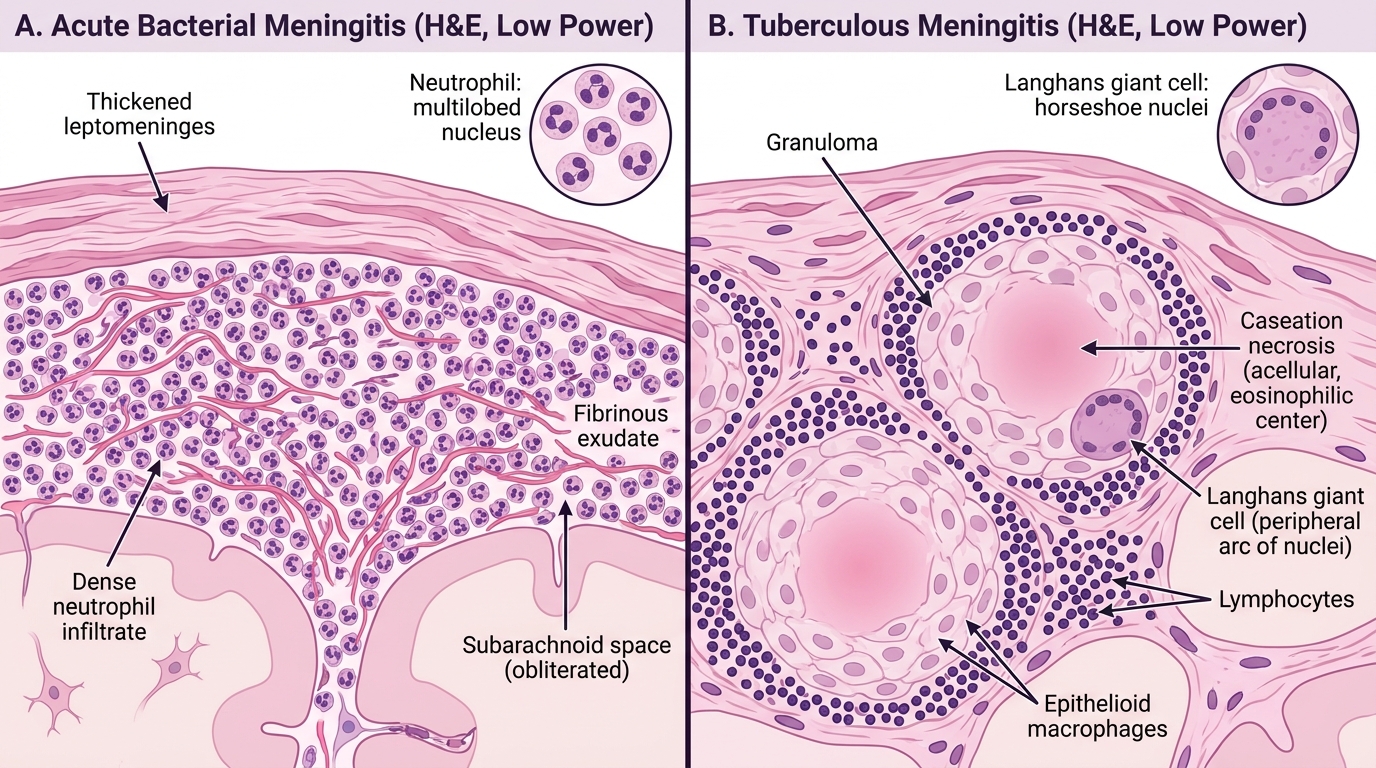
Meningitis Histology: Bacterial vs Tuberculous (H&E, Low Power)
Acute bacterial (purulent) meningitis:
• Gross: thick, creamy, yellow-green exudate in the subarachnoid space, most prominent over convexities and around base. Meningeal vessels congested.
• Micro: subarachnoid space packed with neutrophils and fibrin. Bacteria may be visible on Gram stain. Pia and arachnoid are infiltrated; brain parenchyma shows reactive changes at the surface.
• Causative organisms by age: Neonates → Escherichia coli, Streptococcus agalactiae; Infants/children → Haemophilus influenzae, Streptococcus pneumoniae, Neisseria meningitidis; Adults → Streptococcus pneumoniae, Neisseria meningitidis; Elderly/immunosuppressed → Listeria monocytogenes.
• Sequelae: cerebral oedema, hydrocephalus (exudate blocks CSF flow), cranial nerve palsies, septicaemia, Waterhouse-Friderichsen syndrome (N. meningitidis + adrenal haemorrhage + DIC).
Tuberculous meningitis:
• Gross: thick, gelatinous, grey-green exudate concentrated at the base of the brain (basal exudate); involvement of Sylvian fissure, interpeduncular cistern; miliary granules on meninges.
• Micro: granulomatous inflammation — well-formed epithelioid granulomas with Langhans giant cells (horseshoe-shaped nucleus arrangement), lymphocytes, plasma cells, and central caseation necrosis (pink, acellular, cheese-like material).
• ZN stain: acid-fast bacilli (AFB) — beaded red rods on blue background.
• Sequelae: communicating hydrocephalus (most common complication), arteritis → cerebral infarcts, cranial nerve involvement (II, III, VI most common), tuberculoma formation, spinal arachnoiditis.
Practical tip: The key discriminator is the dominant cell type — neutrophils = bacterial; lymphocytes + granulomas + caseation = TB.