Page 18 of 25
PA27.3-4 | Acute & Chronic Renal Failure — SDL Guide (Part 4)
AKI vs CKD — Distinguishing Features
AKI vs CKD: Distinguishing Features
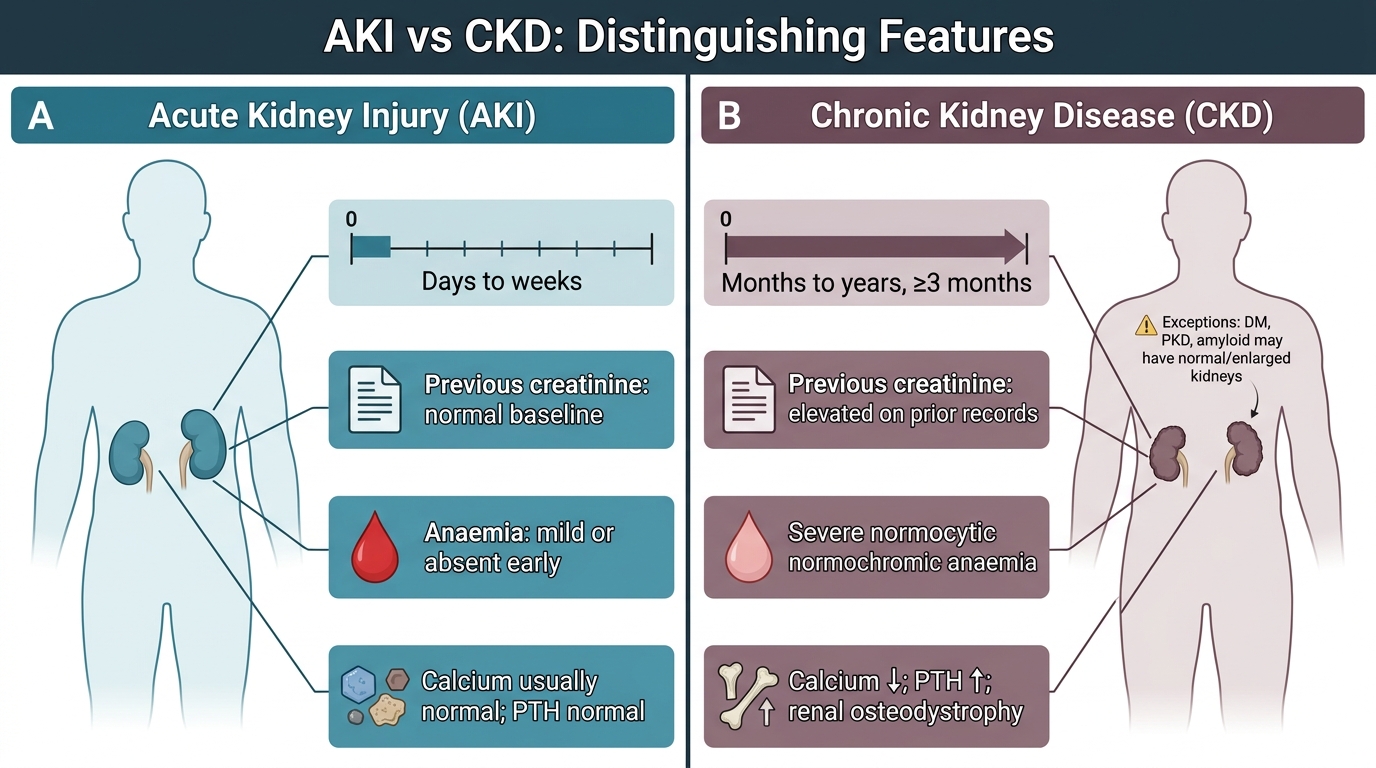
Distinguishing AKI from CKD at presentation is a critical clinical-pathological skill:
| Feature | AKI | CKD |
|---|---|---|
| Onset | Days to weeks | Months to years (≥3 months criterion) |
| Previous creatinine | Normal baseline | Elevated on prior records |
| Kidney size (USS) | Normal to enlarged | Small, contracted (except DM, PKD, amyloid) |
| Anaemia | Mild or absent (early) | Severe normocytic normochromic |
| Calcium | Usually normal | ↓ (renal osteodystrophy) |
| PTH | Normal | ↑ (secondary hyperparathyroidism) |
| Nails/neuropathy | Absent | Mees' lines, peripheral neuropathy |
| Renal biopsy | Tubular necrosis; recoverable | Glomerulosclerosis, fibrosis, atrophy — irreversible |
| Reversibility | Potentially full recovery | Irreversible; progressive |
Important: AKI on CKD — a patient with pre-existing CKD may develop an acute insult (dehydration, sepsis, contrast) that worsens GFR acutely. Treating the acute component may restore to the CKD baseline (not normal). Always look for a reversible precipitant.
Management principles (brief):
- AKI: treat the cause (fluids for prerenal; remove nephrotoxins), prevent complications, renal replacement therapy (RRT) if AEIOU criteria met.
- CKD: slow progression (RAAS blockade, BP control, glycaemic control), manage complications (EPO for anaemia, vitamin D analogues + phosphate binders for bone disease, dietary K⁺/phosphate restriction), plan for RRT (haemodialysis, peritoneal dialysis, or transplant — the curative option).
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
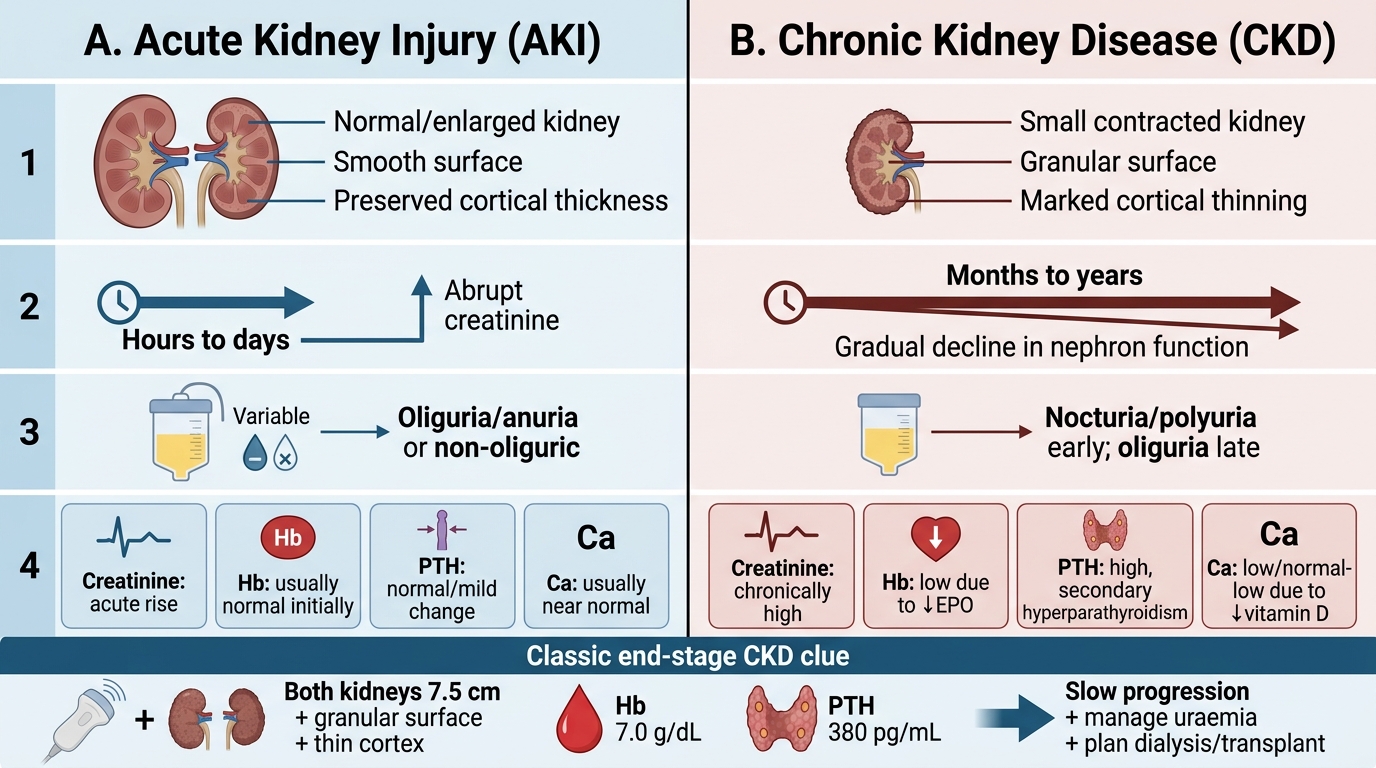
AKI vs CKD: Morphology, Timeline, Urine Output, and Labs
SELF-CHECK
Ultrasound of a patient with renal failure shows both kidneys measuring 7.5 cm with granular surfaces and markedly thinned cortices. Haemoglobin is 7.0 g/dL, PTH is 380 pg/mL. Which diagnosis is most consistent, and what is the primary management goal?
A. AKI due to ATN; aggressive fluid resuscitation
B. Prerenal AKI; IV fluid challenge and recheck creatinine
C. Chronic kidney disease (likely end-stage); slow progression and plan renal replacement therapy
D. Polycystic kidney disease; genetic counselling
Reveal Answer
Answer: C. Chronic kidney disease (likely end-stage); slow progression and plan renal replacement therapy
Small contracted granular kidneys + severe anaemia (normocytic, ↓EPO) + markedly elevated PTH (secondary hyperparathyroidism from ↓vitamin D) are the classical triad of end-stage CKD. In AKI, kidneys are normal or enlarged and anaemia/osteodystrophy are absent or mild. PKD kidneys are massively enlarged, not contracted. Management now shifts to slowing any residual progression, managing uraemic complications, and planning haemodialysis/peritoneal dialysis or transplant referral.