Page 9 of 25
PA27.5-6 | Glomerular Diseases — SDL Guide (Part 4)
IgA Nephropathy (Berger Disease) — PA27.6 In Depth
IgA Nephropathy: Pathogenesis and Clinical Hallmark
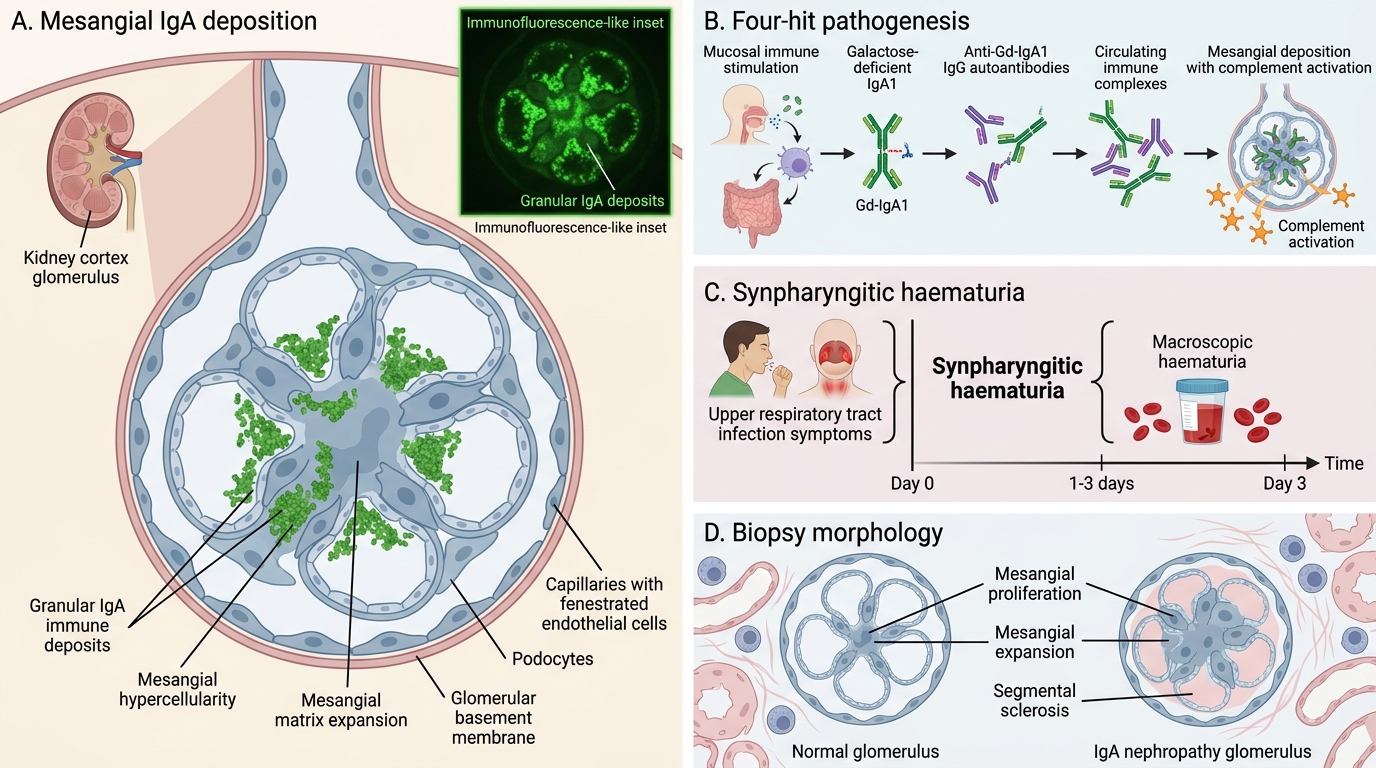
IgA nephropathy (Berger disease) is the commonest primary glomerulonephritis worldwide, particularly in Asia and Southeast Asia. It is characterised by mesangial IgA deposition and a distinctive clinical-temporal pattern.
Epidemiology: Commonest in Asian men, aged 15-35 years. Prevalence up to 30-40% of primary GN in biopsy series in East and South Asia.
Pathogenesis (four-hit model):
1. Hit 1 — Aberrant IgA1 glycosylation: The hinge region of IgA1 is normally O-glycosylated. In IgA nephropathy, galactose-deficient IgA1 (Gd-IgA1) is produced in excess — a structural defect recognised as 'foreign'.
2. Hit 2 — Anti-Gd-IgA1 autoantibodies (usually IgG) form against the aberrant IgA1.
3. Hit 3 — Immune complex formation: Gd-IgA1 + anti-Gd-IgA1 IgG form large immune complexes in the circulation.
4. Hit 4 — Mesangial deposition: These complexes deposit in the mesangium, activate mesangial cells and complement (alternative + lectin pathways), causing mesangial expansion, hypercellularity, and eventually sclerosis.
Why mucosal infection triggers episodes? Mucosal (respiratory, GI) infections drive IgA secretion — in IgA NP, this also drives aberrant Gd-IgA1 production, producing clinical flares.
Clinical hallmark — synpharyngitic haematuria: Macroscopic haematuria occurring simultaneously with (or within 1-3 days of) an upper respiratory tract infection — 'syn' = simultaneous. This is in contrast to PSGN where haematuria occurs 1-3 weeks AFTER the infection (the latent period). This timing distinction is diagnostically critical.
IgA Nephropathy: Mesangial IgA Deposits on Immunofluorescence
Pathology:
• LM: Most common finding is mesangial hypercellularity and mesangial matrix expansion. Can range from minimal change (focal, mild) to florid mesangial proliferation, focal endocapillary proliferation (in active disease), or crescents (in severe disease — Oxford MEST-C score grades lesions).
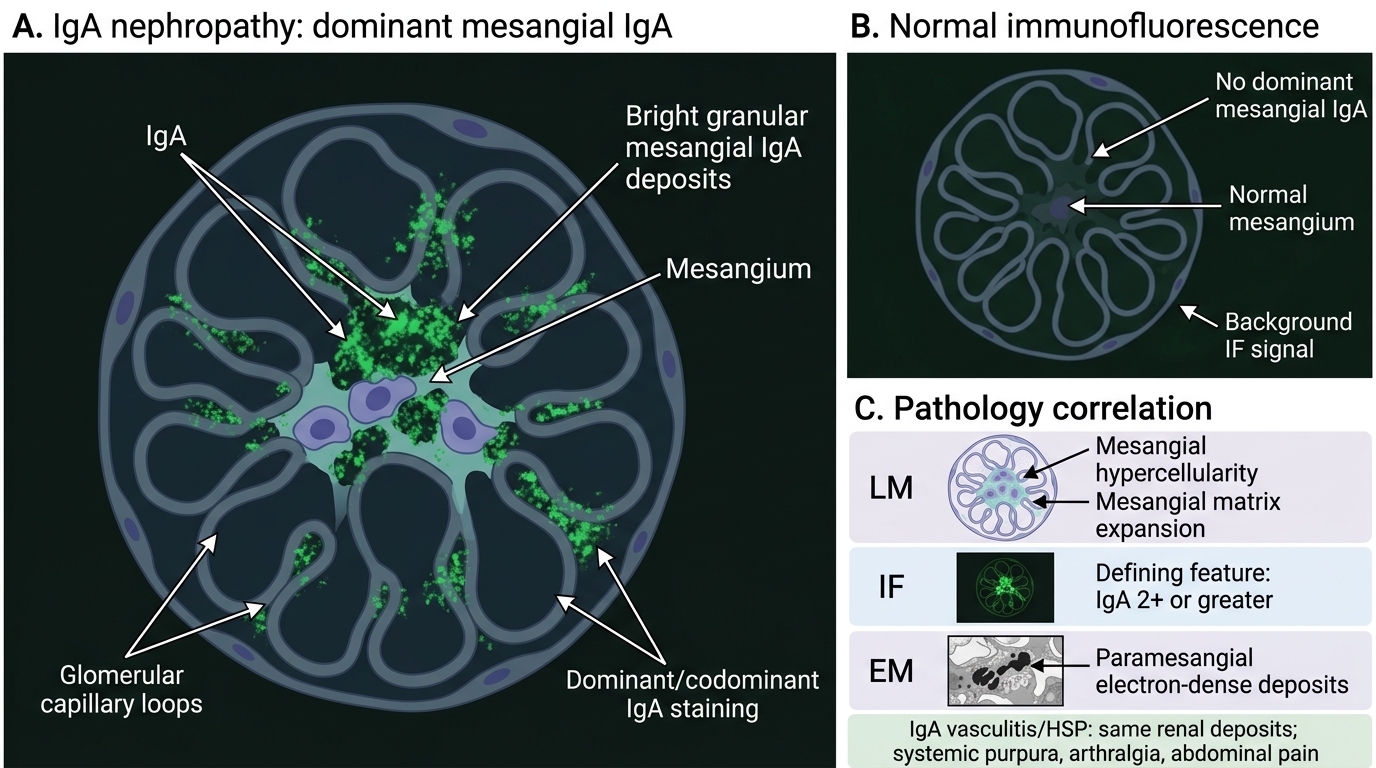
• IF: Dominant or codominant mesangial IgA deposits — this is the DEFINING FEATURE. IgA staining must be 2+ or greater and dominant/co-dominant (not just incidental). Often accompanied by C3 and IgM; IgG is typically weak or absent.
• EM: Electron-dense deposits predominantly in the mesangium (paramesangial), occasionally extending into the subendothelial space in active disease.
Association with Henoch-Schönlein Purpura (HSP) / IgA vasculitis: HSP (now called IgA vasculitis) is considered the systemic form of IgA nephropathy. It shares the same mesangial IgA deposits and the same Gd-IgA1 pathogenesis. In addition to the nephritis, HSP shows: palpable purpura (non-thrombocytopenic, legs and buttocks), arthralgia, and abdominal pain (GI IgA vasculitis). The renal histology is indistinguishable from isolated IgA nephropathy — the distinction is purely clinical.
Alport syndrome (brief): Alport syndrome is an X-linked (most common) hereditary nephritis caused by mutations in COL4A5 encoding the α5 chain of type IV collagen. LM shows progressive GBM thickening and lamellation. EM is pathognomonic: irregular GBM thickening with basket-weave/lamellar splitting. IF is negative (no IgA, no Ig). Associated with sensorineural hearing loss and ocular abnormalities (lenticonus). Unlike IgA nephropathy, it is hereditary, NOT immune-complex mediated.
Thin Basement Membrane Nephropathy (TBMND): Benign familial haematuria; EM shows diffuse thinning of the GBM (< 250 nm; normal 300-400 nm) without splitting. Excellent prognosis. Important differential for isolated haematuria.
Oxford MEST-C classification of IgA NP: Mesangial hypercellularity (M), Endocapillary proliferation (E), Segmental sclerosis (S), Tubular atrophy/interstitial fibrosis (T), Crescents (C) — each scored 0/1 on biopsy. High MEST-C score predicts progression to ESRD.
CLINICAL PEARL
IgA nephropathy vs PSGN timing is the most-tested distinction in Indian exams:
• IgA NP: Haematuria SIMULTANEOUS with the infection (synpharyngitic — within 1-3 days). Complement NORMAL.
• PSGN: Haematuria 1-3 weeks AFTER the infection (post-streptococcal — latent period). Complement LOW (C3).
If a student gets the timing backwards, the entire differential collapses. Drill this table until it is automatic.
SELF-CHECK
A 22-year-old medical student develops painless cola-coloured urine on the same day he develops a fever and sore throat. Urinalysis shows RBC casts. Serum C3 is NORMAL. Kidney biopsy is most likely to show:
A. Subepithelial humps on EM and low C3 confirming post-infectious GN
B. Linear IgG on IF confirming anti-GBM disease
C. Dominant mesangial IgA deposits on IF confirming IgA nephropathy
D. Diffuse foot process effacement on EM confirming minimal change disease
Reveal Answer
Answer: C. Dominant mesangial IgA deposits on IF confirming IgA nephropathy
The simultaneous onset of haematuria with the respiratory infection (synpharyngitic haematuria) and normal complement are the two diagnostic clues for IgA nephropathy (Berger disease). PSGN requires 1-3 weeks latency and shows LOW C3. The biopsy hallmark is dominant mesangial IgA on IF. This is the most common GN worldwide.
Syndrome Comparison Table: Nephrotic vs Nephritic
Nephrotic vs Nephritic Syndrome
| Feature | Nephrotic | Nephritic |
|---|---|---|
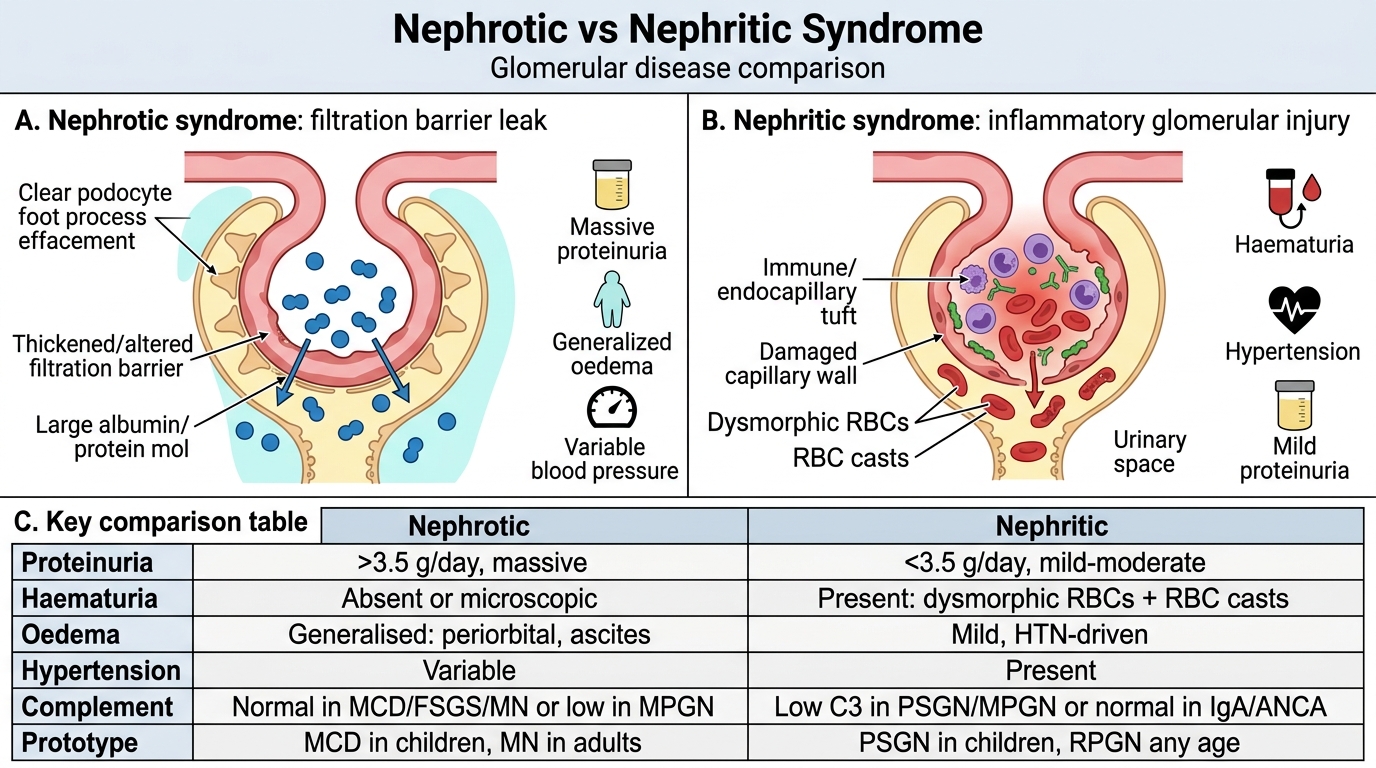
| Proteinuria | > 3.5 g/day (massive) | < 3.5 g/day (mild-mod) |
| Haematuria | Absent (or microscopic) | Present — dysmorphic RBCs + RBC casts |
| Oedema | Generalised (periorbital, ascites) | Mild (HTN-driven) |
| Hypertension | Variable | Present |
| Complement | Normal (MCD, FSGS, MN) OR low (MPGN) | Low C3 (PSGN, MPGN) or Normal (IgA, ANCA) |
| Prototype | MCD (children), MN (adults) | PSGN (children), RPGN (any age) |
Glomerular disease — LM / IF / EM at a glance:
| Disease | LM | IF | EM |
|---|---|---|---|
| MCD | Normal | Negative | Foot process effacement |
| FSGS | Focal segmental sclerosis | IgM/C3 in sclerotic areas | Foot process effacement |
| Membranous NP | GBM thickening, spikes | Granular IgG subepithelial | Subepithelial deposits, spikes |
| MPGN | Mesangial proliferation, tram-track | Granular C3 ± Ig | Subendothelial deposits (I) / intramembranous ribbon (DDD) |
| PSGN | Diffuse endocapillary hypercellularity | Lumpy-bumpy IgG/C3 | Subepithelial humps |
| RPGN (I) | Crescents (≥50%) | Linear IgG | — |
| RPGN (III) | Crescents (≥50%) | Negative | — |
| IgA NP | Mesangial proliferation | Dominant mesangial IgA | Mesangial deposits |
| Alport | GBM thickening | Negative | GBM basket-weave splitting |
Diabetic Nephropathy — Cross-Reference
Diabetic Nephropathy: Glomerular Lesions and Diagnostic Clues
Diabetic nephropathy (covered in depth in SDL3 — Metabolic and Vascular Renal Diseases) is the most common cause of ESRD worldwide, but its glomerular changes are relevant here for the differential diagnosis of nephrotic syndrome in adults.
Glomerular lesions:
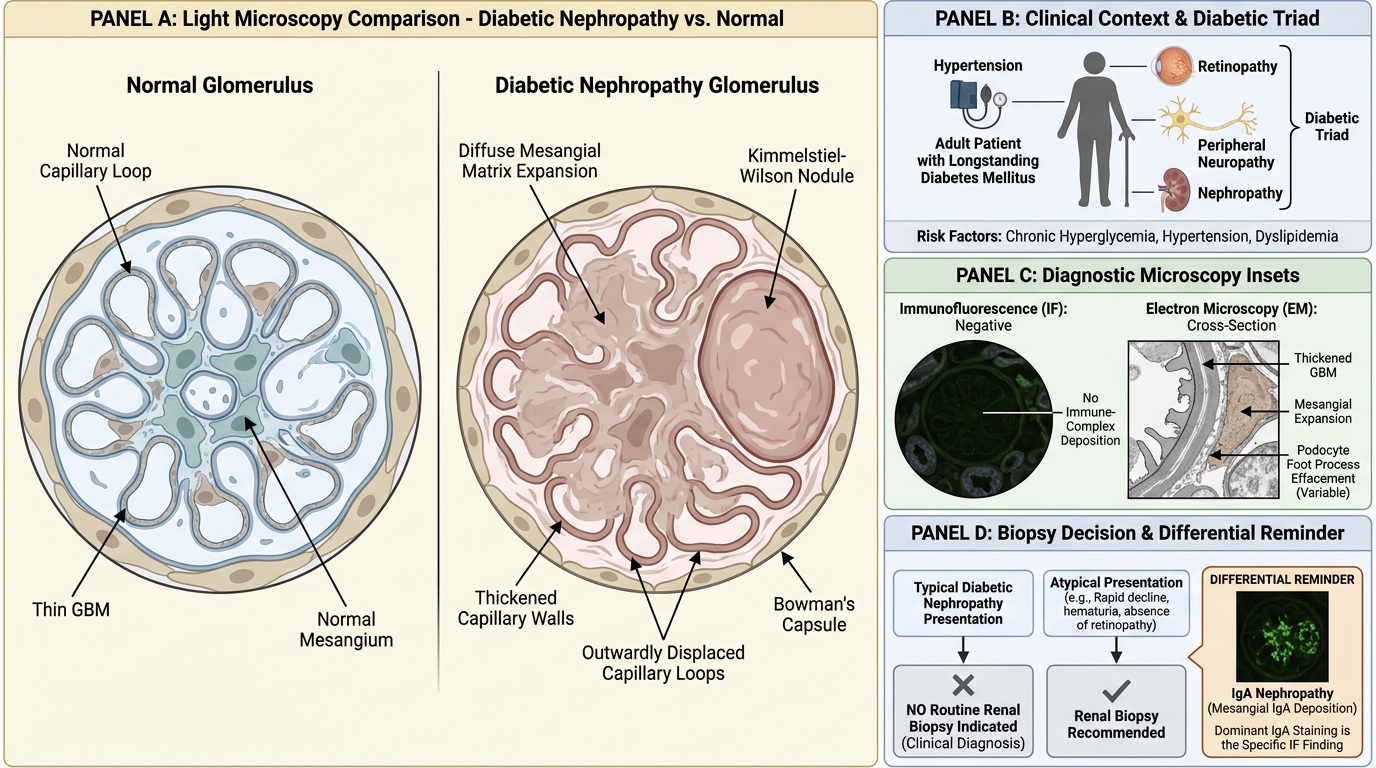
• Diffuse glomerulosclerosis: Generalised increase in mesangial matrix — the most common diabetic glomerular lesion.
• Nodular glomerulosclerosis (Kimmelstiel-Wilson nodules): Pathognomonic oval/spherical deposits of matrix in the periphery of the glomerulus, pushing peripheral capillaries outward. Seen in < 20% of diabetics but diagnostic when present.
• GBM thickening: Early, universal finding.
Tip for differential: Diabetic nephropathy produces nephrotic-range proteinuria in an adult with longstanding diabetes, hypertension, and retinopathy — the 'diabetic triad' (retinopathy + nephropathy + neuropathy). IF is negative (no immune-complex deposition). EM shows GBM thickening and mesangial expansion. Biopsy is NOT routinely performed in clear-cut diabetic nephropathy — it is reserved for atypical presentations.
SELF-CHECK
On a renal biopsy immunofluorescence panel, which of the following findings is MOST specific for IgA nephropathy?
A. Diffuse granular C3 and IgG along the capillary wall
B. Linear IgG along the GBM
C. Dominant mesangial IgA deposition (2+ or greater, dominant or co-dominant)
D. Negative immunofluorescence with normal complement
Reveal Answer
Answer: C. Dominant mesangial IgA deposition (2+ or greater, dominant or co-dominant)
Dominant or co-dominant mesangial IgA (≥ 2+ intensity, with IgA being the dominant immunoglobulin) is the defining and most specific IF finding for IgA nephropathy. Granular IgG/C3 is seen in PSGN and other immune-complex GN. Linear IgG is anti-GBM disease. Negative IF with normal complement characterises ANCA-pauci-immune RPGN or minimal change disease.