Page 13 of 25
PA27.7 | Glomerular Manifestations of Systemic Disease — SDL Guide (Part 3)
Interpreting the Clinical Syndrome in Context
Clinical Interpretation of Systemic Renal Disease
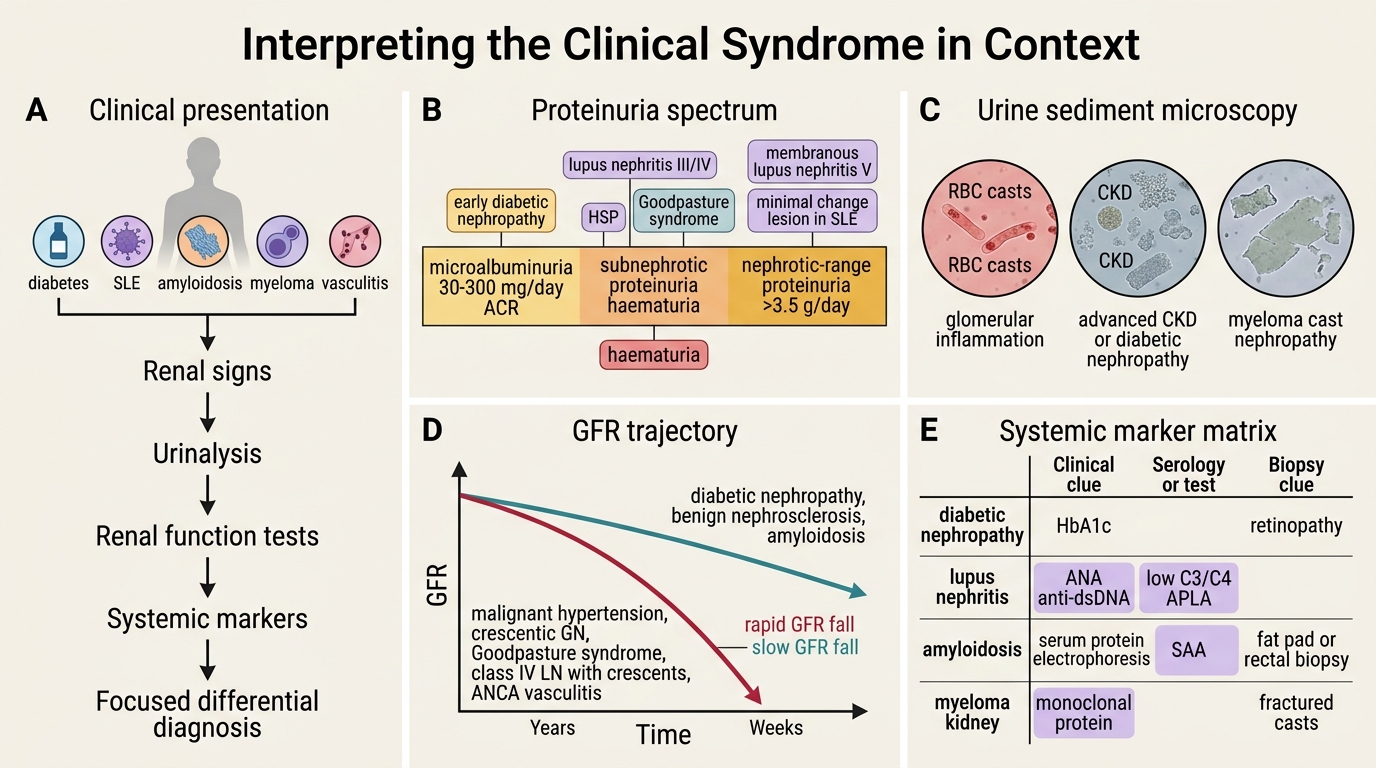
When a patient with a known systemic disease develops renal signs, a structured approach to the urinalysis and renal function tests narrows the differential rapidly.
Step 1 — Proteinuria quantification:
• Microalbuminuria (30–300 mg/day ACR): early diabetic nephropathy, stage III Mogensen.
• Nephrotic-range (>3.5 g/day): diabetic nephropathy (advanced), amyloidosis, membranous LN (class V), minimal change lesion in SLE.
• Subnephrotic + haematuria: lupus (classes III/IV), HSP, Goodpasture.
Step 2 — Urine sediment:
• RBC casts → glomerular inflammation (nephritis) → lupus IV, Goodpasture, ANCA vasculitis.
• Granular casts + waxy casts → CKD, diabetic nephropathy (advanced).
• Large fractured casts, giant cell reaction on biopsy → myeloma cast nephropathy.
Step 3 — GFR trajectory:
• Slowly progressive over years → diabetic nephropathy, benign nephrosclerosis, amyloidosis.
• Rapidly progressive (weeks) → malignant hypertension, crescentic GN (Goodpasture, class IV LN with crescents, ANCA).
Step 4 — Correlate with systemic markers:
| Systemic Disease | Key Serological / Clinical Clue |
|---|---|
| Diabetic nephropathy | HbA1c, retinopathy (co-existing microvascular disease), NO biopsy usually needed |
| Lupus nephritis | ANA, anti-dsDNA, low C3+C4, APLA |
| Amyloidosis | Serum protein electrophoresis, SAA level, rectal/fat pad biopsy |
| Myeloma | Serum + urine protein electrophoresis, Bence Jones protein |
| Goodpasture | Anti-GBM antibody, haemoptysis |
| Hypertension | BP history, fundoscopy, cardiac LVH |
| HSP | Palpable purpura, IgA levels |
The key rule: proteinuria in a diabetic patient + retinopathy = diabetic nephropathy (no biopsy needed). Atypical features (rapid decline, haematuria, short diabetes duration, NO retinopathy) → biopsy to exclude superimposed non-diabetic renal disease.
CLINICAL PEARL
An important examination and clinical pitfall: not all renal disease in a diabetic is diabetic nephropathy. Studies show 30–40% of diabetic patients biopsied for atypical features have an underlying non-diabetic cause (IgA nephropathy, FSGS, membranous GN, ANCA vasculitis). The biopsy decision hinge-points are: (1) absent diabetic retinopathy (retinopathy almost always precedes nephropathy in type 1 DM; less reliable in type 2), (2) heavy haematuria, (3) rapid GFR decline (>3.5 mL/min/year), (4) short duration of DM (<5 years). In these situations, biopsy changes management in a majority of cases.
SELF-CHECK
A 35-year-old woman with SLE develops rapidly progressive renal failure over 6 weeks. Urinalysis shows 2+ blood with dysmorphic RBCs and RBC casts. Serum C3 and C4 are markedly depressed. Anti-dsDNA titre is very high. Which finding on renal biopsy would MOST specifically indicate that she requires aggressive immunosuppression?
A. Mesangial IgA deposits with mesangial hypercellularity
B. Subepithelial spikes on GBM with diffuse GBM thickening
C. Wire-loop lesions with full-house IF in >50% of glomeruli
D. Acellular mesangial deposits that stain with Congo red
Reveal Answer
Answer: C. Wire-loop lesions with full-house IF in >50% of glomeruli
Wire-loop lesions (massive subendothelial immune complex deposits) with full-house IF (IgG+IgA+IgM+C3+C4+C1q) in >50% of glomeruli defines class IV diffuse lupus nephritis — the most severe class with the worst prognosis and the strongest indication for aggressive immunosuppression (cyclophosphamide/mycophenolate + steroids). Option A describes IgA nephropathy/HSP (not the dominant IF pattern in SLE). Option B describes membranous LN (class V — heavy proteinuria but NOT nephritic/rapidly progressive). Option D describes amyloidosis, not SLE.
Comparing the Major Systemic Glomerulopathies — Summary Table
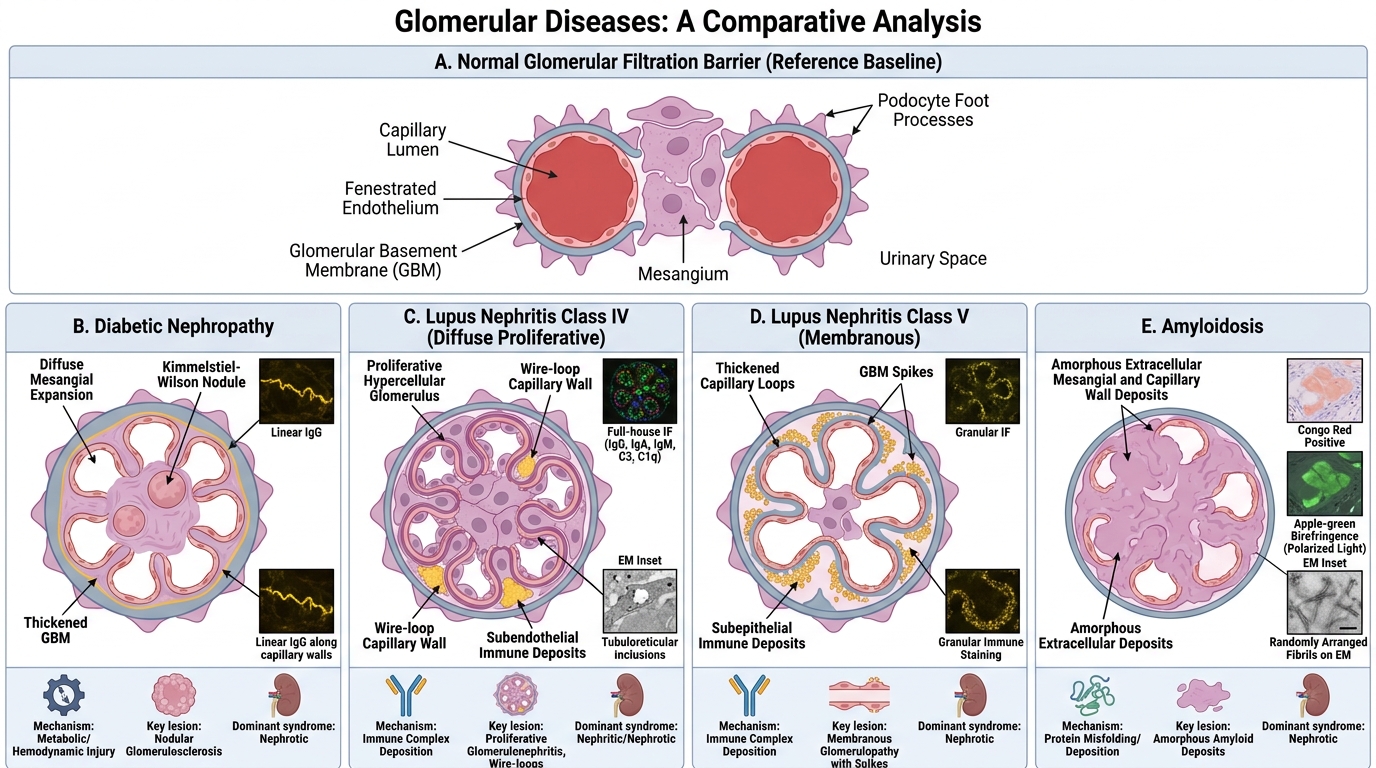
Major Systemic Glomerulopathies: Mechanisms and Key Lesions
| Disease | Primary Mechanism | LM Key Lesion | IF Pattern | EM Key Finding | Dominant Syndrome |
|---|---|---|---|---|---|
| Diabetic nephropathy | AGEs, haemodynamic | KW nodules, diffuse mesangial ↑ | Non-specific linear IgG | GBM thickening, mesangial ↑ | Nephrotic (late) |
| Lupus nephritis IV | Immune complex (anti-dsDNA) | Wire-loop, endocap proliferation | Full-house | Subendothelial deposits, TRI | Nephrotic + nephritic |
| Lupus nephritis V | Immune complex | GBM spikes/thickening | IgG, IgA, IgM subepithelial | Subepithelial deposits | Nephrotic |
| Amyloidosis | Fibril deposition | Amorphous eosinophilic mesangial | Negative (AA); LC-restricted (AL) | 8–10 nm non-branching fibrils | Nephrotic |
| Benign HTN nephrosclerosis | Ischaemia, haemodynamic | Hyaline arteriolosclerosis | Negative | Non-specific | Mild proteinuria, CKD |
| Malignant HTN nephrosclerosis | Vascular injury | Fibrinoid necrosis, onion-skin | Negative | Fibrin/platelet thrombi | AKI, haematuria |
| Goodpasture | Anti-GBM Ab | Crescentic GN | Linear IgG along GBM | GBM disruption | Rapidly progressive GN |
| Amyloid (myeloma-related) | AL protein fibrils | Same as above | Lambda (or kappa) LC | Fibrils | Nephrotic |
| HSP | IgA vasculitis | Mesangial proliferation | IgA dominant mesangial | Mesangial electron-dense deposits | Haematuria + proteinuria |
| Cast nephropathy (myeloma) | LC toxicity | Fractured casts, giant cells | Light-chain casts | Non-specific | AKI + myeloma features |