Page 12 of 25
PA27.7 | Glomerular Manifestations of Systemic Disease — SDL Guide (Part 2)
Renal Amyloidosis
Renal Amyloidosis: Morphology and Types
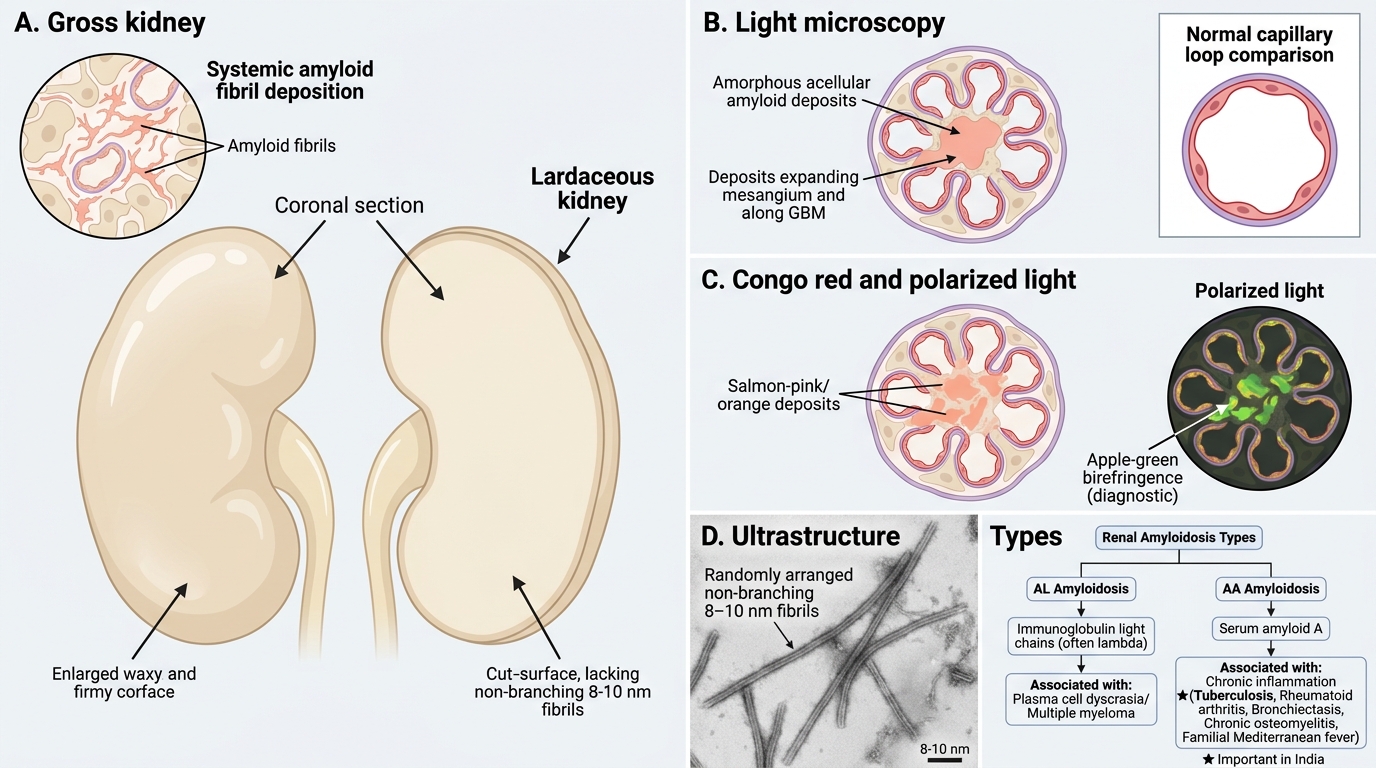
Amyloidosis is the deposition of insoluble fibrillar proteins (β-pleated sheet conformation) in tissues. The kidney is the most commonly and most seriously affected organ in systemic amyloidosis, and renal disease is the leading cause of death in patients with amyloidosis.
Types relevant to renal pathology:
• AL amyloidosis (primary/myeloma-associated) — amyloid derived from immunoglobulin light chains (most often lambda). Occurs in multiple myeloma and plasma cell dyscrasias.
• AA amyloidosis (secondary/reactive) — derived from serum amyloid A protein (SAA), an acute-phase reactant. Occurs in chronic inflammatory conditions: rheumatoid arthritis, tuberculosis, bronchiectasis, chronic osteomyelitis, familial Mediterranean fever.
• In India, AA amyloidosis secondary to tuberculosis is a significant contributor.
Morphology:
• Grossly: enlarged, pale, waxy, firm kidneys ("lardaceous kidney").
• LM: H&E shows amorphous, acellular, eosinophilic deposits in mesangium, expanding it, and along GBM. Initially mesangial, then subendothelial/GBM. Later — tubular basement membranes and vessel walls.
• Congo red stain — deposits stain salmon-pink/orange. Under polarised light: apple-green birefringence — the single most important diagnostic feature of amyloid.
• EM: 8–10 nm non-branching randomly arranged fibrils — distinct from collagen or immune complex deposits.
• IF: AL amyloid may show light-chain restriction (kappa or lambda); AA amyloid is IF-negative for immunoglobulins.
Clinical: Insidious onset nephrotic syndrome is the dominant presentation (massive proteinuria, hypoalbuminaemia, oedema). Renal vein thrombosis is a complication. Renal failure develops over years. Hepatosplenomegaly may be present; cardiac amyloid (stiff heart, low voltage ECG) adds to mortality.
SELF-CHECK
A 45-year-old man with a 20-year history of pulmonary tuberculosis presents with 6+ g/day proteinuria and bilateral leg oedema. Renal biopsy shows acellular eosinophilic deposits in the mesangium and along GBM. Congo red stain is performed. What is the expected finding under polarised light?
A. Yellow-green fluorescence (thioflavin T pattern)
B. Apple-green birefringence
C. Salmon-pink without polarisation change
D. Negative — Congo red is not used for amyloid
Reveal Answer
Answer: B. Apple-green birefringence
Apple-green birefringence under polarised light after Congo red staining is the pathognomonic finding for amyloid. The salmon-pink/orange colour on conventional light microscopy is also characteristic, but polarisation is the diagnostic confirmatory step. This is AA amyloidosis secondary to chronic tuberculosis. Thioflavin T (option A) also stains amyloid (yellow-green fluorescence) but is less specific and not the primary diagnostic stain. Congo red is absolutely the stain of choice for amyloid — option D is incorrect.
Hypertensive Nephrosclerosis — Benign and Malignant
Benign vs Malignant Hypertensive Nephrosclerosis
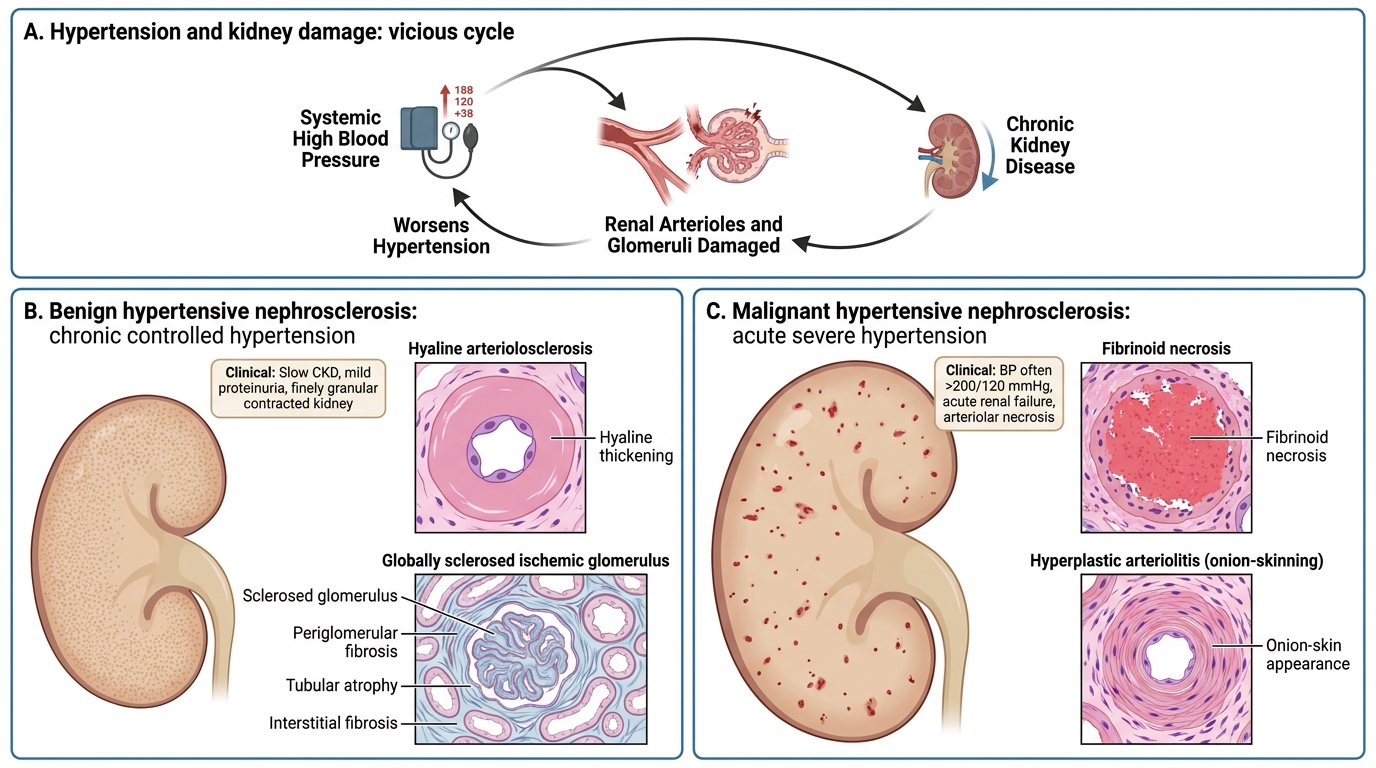
Hypertension is both a cause and a consequence of chronic kidney disease, creating a vicious cycle. Two distinct morphological patterns reflect the speed and severity of BP elevation.
Benign hypertensive nephrosclerosis (chronic, controlled hypertension):
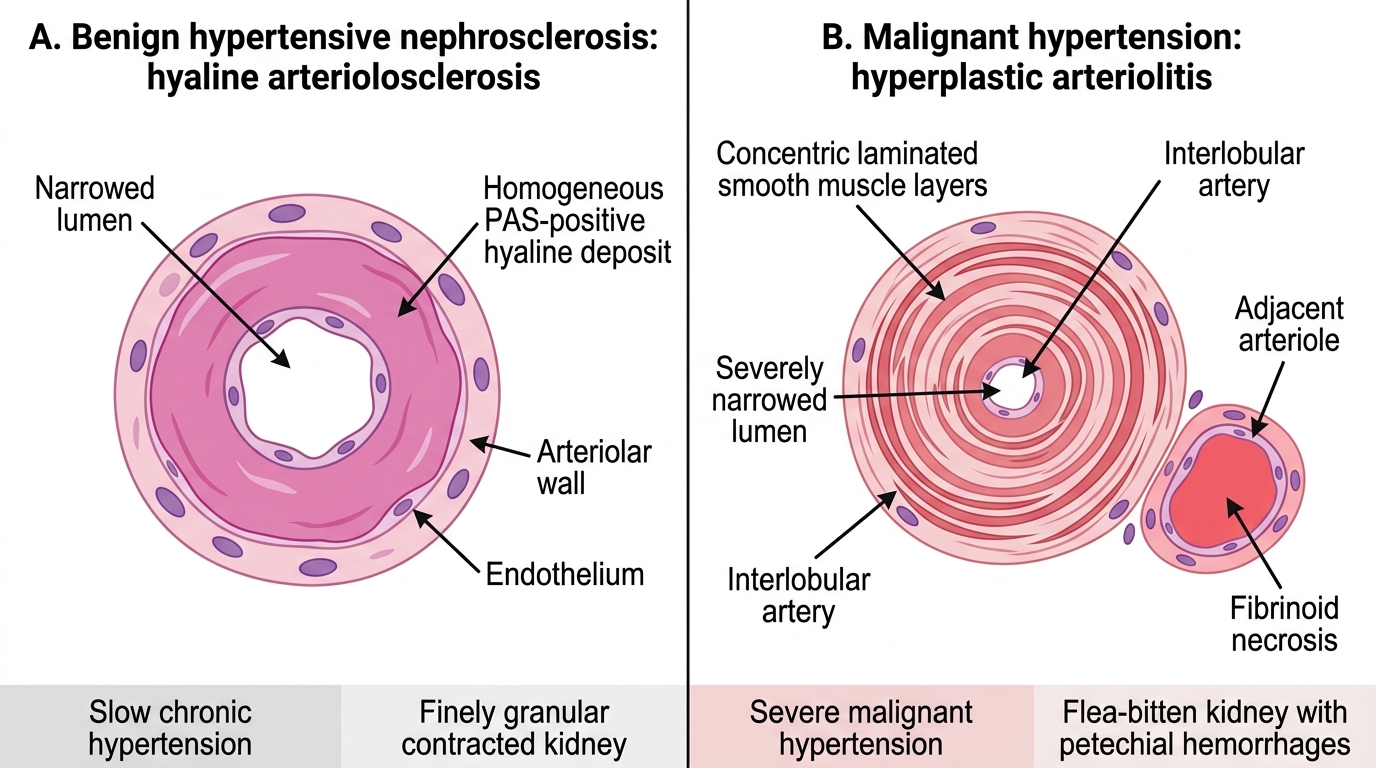
- Hyaline arteriolosclerosis — deposition of homogeneous, eosinophilic, glassy hyaline material in the intima and media of afferent arterioles (plasma protein insudation + smooth muscle degeneration). This is the hallmark vascular change.
- Fibrous intimal thickening of interlobular arteries — concentric intimal fibromuscular proliferation narrows the lumen.
- Glomeruli: ischaemic obsolescence — global glomerulosclerosis (wrinkling and collapse of GBM, periglomerular fibrosis). Tubular atrophy. Interstitial fibrosis.
- Gross appearance: finely granular contracted kidney — diffuse cortical granularity from alternating ischaemic contracted nephrons and compensatorily hypertrophied ones.
- Clinical: slowly progressive CKD; mild proteinuria (usually <1.5 g/day, rarely nephrotic); CKD in hypertensive Afro-Caribbean patients is disproportionately from nephrosclerosis.
Malignant hypertensive nephrosclerosis (BP typically >200/120 mmHg, acute elevation):
- Fibrinoid necrosis of arterioles — vessel wall destroyed by plasma protein insudation → bright eosinophilic granular necrosis; PAS-negative.
- Hyperplastic arteriolitis ("onion-skin" lesion) — concentric layers of smooth muscle proliferation and laminated collagen in interlobular arteries create a distinctive onion-skin appearance, severely narrowing the lumen.
- Glomeruli: necrotising glomerulitis — segmental fibrinoid necrosis of glomerular tufts; capillary thrombosis; crescents.
- Gross: petechial haemorrhages on cortex ("flea-bitten kidney" — red dots on pale cortex from glomerular haemorrhages).
- Clinical: acute kidney injury, haematuria, rapidly rising creatinine, hypertensive encephalopathy, retinal haemorrhages. Medical emergency.
Hypertensive Renal Vascular Lesions
SELF-CHECK
Autopsy of a 40-year-old man who died of hypertensive encephalopathy shows kidneys with a cortical surface resembling a flea-bitten appearance. Histology reveals concentric laminated layers of smooth muscle in interlobular arteries with near-total luminal occlusion, and fibrinoid necrosis in arterioles. Which pattern is being described?
A. Benign hypertensive nephrosclerosis with hyaline arteriolosclerosis
B. Malignant hypertensive nephrosclerosis with hyperplastic arteriolitis
C. Diabetic nephropathy with efferent arteriolar hyalinosis
D. Thrombotic microangiopathy from TTP
Reveal Answer
Answer: B. Malignant hypertensive nephrosclerosis with hyperplastic arteriolitis
The flea-bitten kidney (cortical petechial haemorrhages) + fibrinoid necrosis of arterioles + hyperplastic onion-skin arteriolitis in interlobular arteries = malignant hypertensive nephrosclerosis. Benign hypertensive nephrosclerosis produces a finely granular contracted kidney (NOT flea-bitten) with hyaline arteriolosclerosis (NOT fibrinoid necrosis). TTP also causes fibrinoid-like deposits but is microangiopathic haemolytic anaemia with systemic microthrombi (platelet-fibrin thrombi in glomerular capillaries), not the concentric onion-skin lesion in arteries.
Other Systemic Causes of Glomerular Injury
Systemic Causes of Glomerular and Renal Injury
Several additional systemic diseases produce characteristic glomerular findings that frequently appear in examinations and clinical practice.
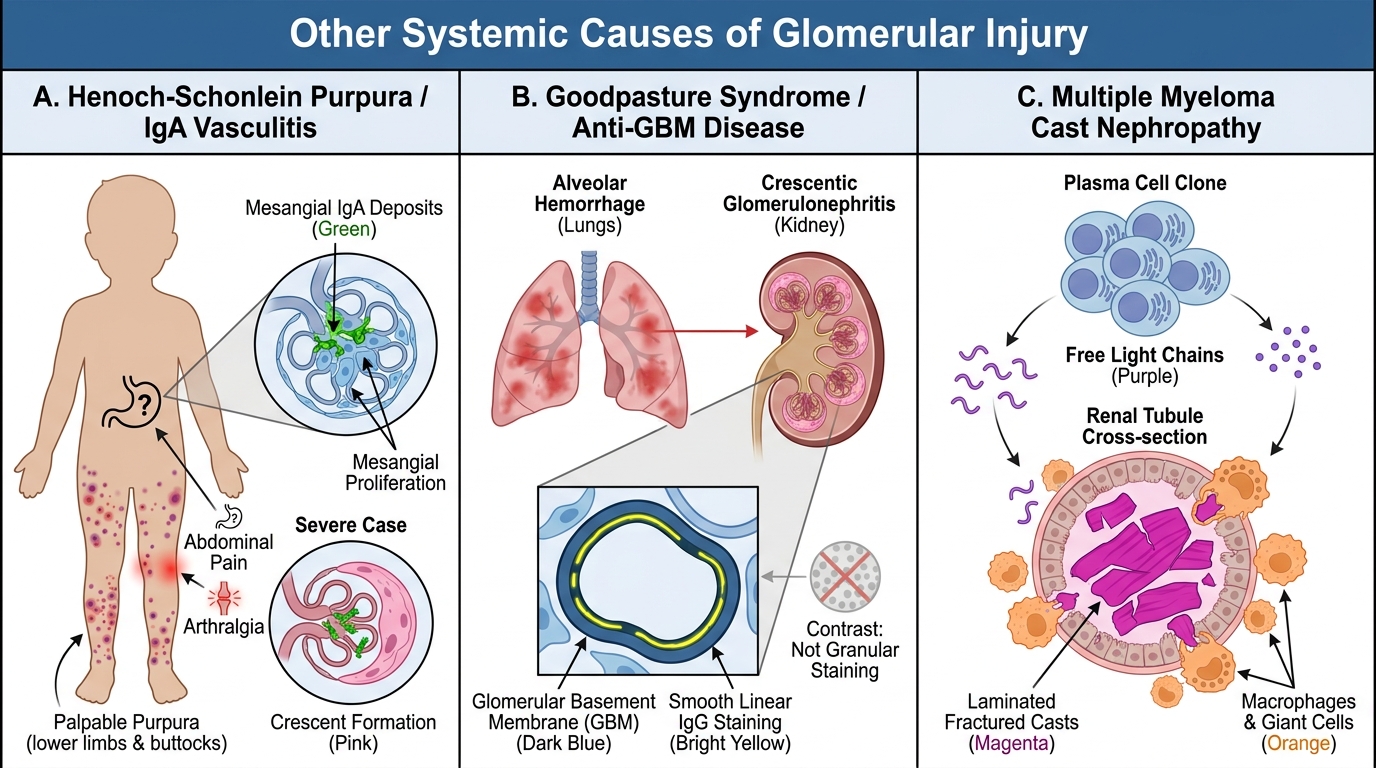
Henoch-Schönlein Purpura (IgA vasculitis)
• Systemic IgA-dominant small-vessel vasculitis (skin, gut, joints, kidney).
• Renal biopsy: mesangial IgA deposits (identical to IgA nephropathy — HSP is its systemic form). Focal to diffuse mesangial proliferation; crescents in severe cases.
• Clinical: palpable purpura on lower limbs and buttocks + abdominal pain + arthralgia + haematuria/proteinuria. Commonest vasculitis in children.
Goodpasture Syndrome (Anti-GBM Disease)
• Autoantibodies against α3 chain of type IV collagen in GBM and alveolar BM → simultaneous pulmonary haemorrhage + rapidly progressive (crescentic) GN.
• IF: linear IgG along GBM — the classic "linear" pattern (vs granular in immune complex, vs negative/pauci in ANCA vasculitis).
• Clinical: haemoptysis + haematuria + rapidly rising creatinine. Medical emergency.
• (Cross-reference: type I RPGN mechanism.)
Multiple Myeloma and Cast Nephropathy
• Free immunoglobulin light chains (Bence Jones proteins) are filtered and overwhelm tubular reabsorption → "myeloma kidney" or cast nephropathy.
• Casts: large, laminated, fractured, PAS-positive tubular casts with surrounding giant cell reaction (macrophage/multinucleated giant cells) — these casts are NOT ordinary hyaline casts.
• AL amyloidosis and light-chain deposition disease are separate myeloma-associated renal conditions.
• Clinical: renal failure + lytic bone lesions + hypercalcaemia + anaemia.
Cryoglobulinaemic GN
• Cryoglobulins are immunoglobulins that precipitate in cold. Type I (monoclonal, myeloma/Waldenström's); Type II and III (mixed, often hepatitis C-associated — MC cause in India).
• Renal: MPGN-like pattern with intraluminal hyaline thrombi (precipitated cryoglobulins), endocapillary proliferation, monocyte infiltration.
• IF: IgM, IgG, C3. EM: organised microtubular or crystalline substructure.
Thrombotic Microangiopathy (TMA)
• Umbrella term: HUS (Shiga toxin — E. coli O157:H7 → primarily in children), TTP (ADAMTS13 deficiency → platelet-fibrin thrombi, thrombocytopaenia, MAHA).
• Renal: glomerular capillary and arteriolar microthrombi, GBM duplication ("double-contour"), endothelial swelling.
• (Brief cross-reference — detailed in vascular pathology module.)
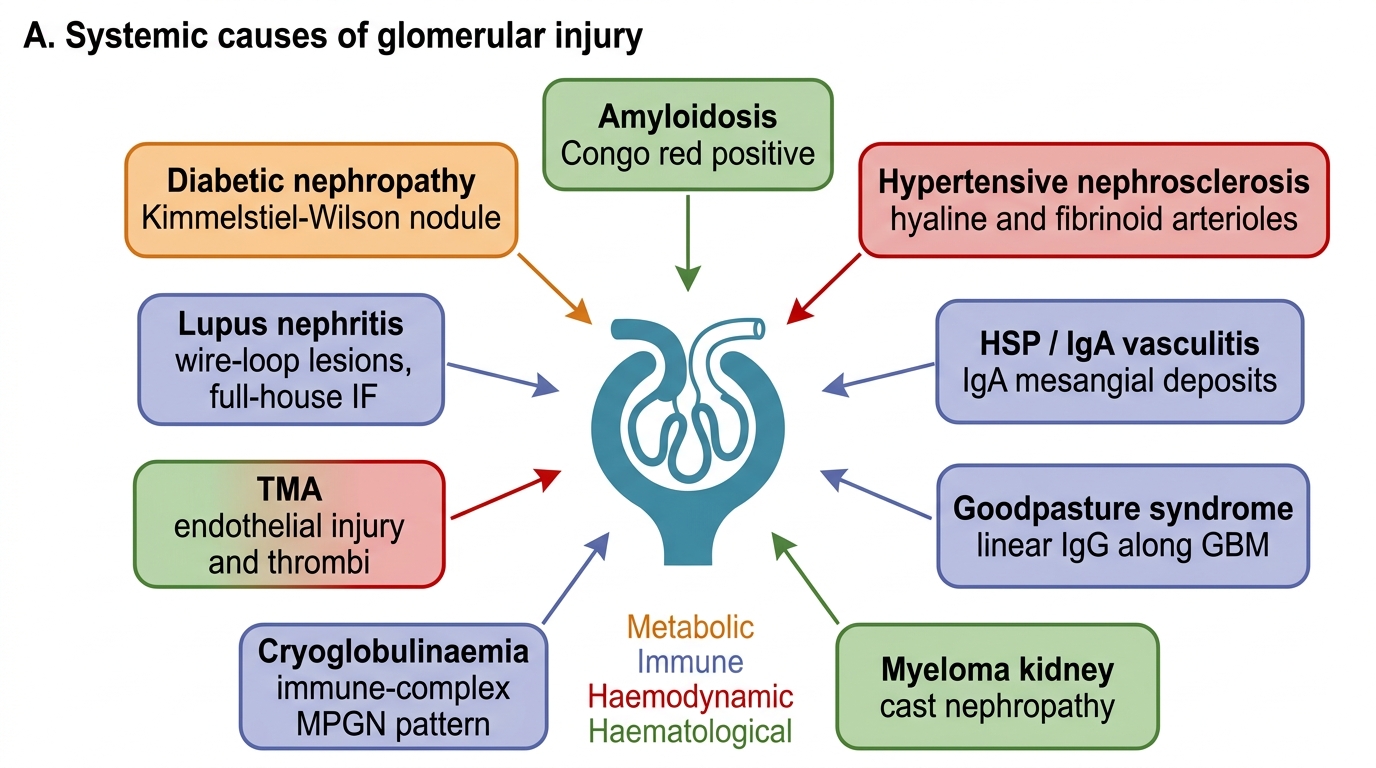
Systemic Causes of Glomerular Injury