Page 1 of 25
PA27.1-2 | Normal Kidney & Clinical Syndromes — SDL Guide
Learning Objectives
- Describe the microanatomy of the nephron — glomerulus (capillary tuft, mesangium, podocytes, GBM, filtration barrier), Bowman capsule, PCT, loop of Henle, DCT, and collecting duct — and identify the juxtaglomerular apparatus.
- Distinguish cortex from medulla by their tubular and vascular contents.
- Define each of the eight renal clinical syndromes and recognise their hallmark urinalysis findings.
- Map a patient's urinalysis profile (cast type, proteinuria magnitude, haematuria) to the appropriate clinical syndrome.
- Differentiate azotaemia from uraemia and link each to the CKD progression spectrum.
- Use the syndrome framework to predict which disease categories to consider before SDL 2–4.
INSTRUCTIONS
Renal pathology begins with two questions: What is the normal kidney supposed to do, and which part has broken down? This module gives you the structural map (nephron anatomy) and the clinical language (syndrome classification) that you will use to decode every renal disease in SDL 2–4. Work through the nephron segment by segment, then practise mapping urinalysis findings to syndromes. Both Robbins Ch 20 and Harsh Mohan Ch 22 cover this material; use either.
References
- Robbins & Kumar: Basic Pathology, 11th ed., Ch 20 (The Kidney) (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch 22 (The Kidney & Lower Urinary Tract) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old student presents after a routine urine dipstick at a health camp: 3+ blood, 2+ protein. She feels completely well. By the end of this module you will know whether her urine tells you she has glomerulonephritis, a nephrotic disorder, or simply a UTI — and why the answer depends on knowing what normal kidney tissue looks like in the first place.
WHY THIS MATTERS
Every renal disease in Years 2 and 3 — glomerulonephritis, nephrotic syndrome, diabetic nephropathy, AKI, CKD — is diagnosed in the clinic before it reaches the microscope. The renal clinical syndromes are the clinician's first sorting tool. Pathologists who cannot map urinalysis findings to a syndrome miss the tissue diagnosis; clinicians who do not understand nephron anatomy cannot interpret the biopsy report. This module is the shared vocabulary.
RECALL
From Year-1 Anatomy and Physiology, bring forward:
• The nephron as the functional unit of the kidney — roughly 1 million per kidney.
• Glomerular filtration rate (GFR) ~125 mL/min; filtration depends on size and charge selectivity.
• Renin–angiotensin–aldosterone axis: renin from the JGA, angiotensin II raises BP, aldosterone retains Na⁺.
• Protein is not normally excreted in urine in significant amounts; its presence signals a filtration barrier defect.
If any of these feel shaky, spend 5 minutes on your Physiology notes before continuing — this module builds on them.
Nephron Architecture: Glomerulus and Filtration Barrier
Glomerulus and Filtration Barrier Architecture
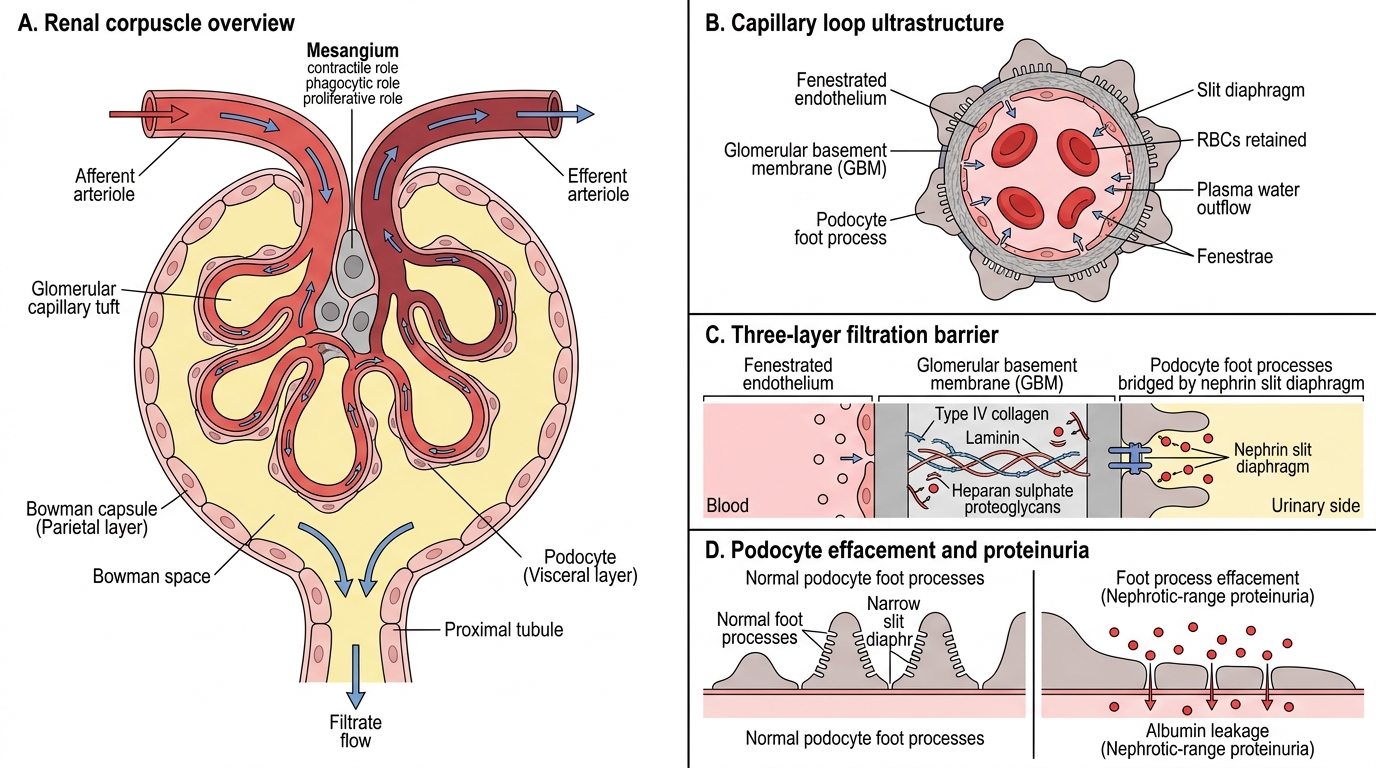
The nephron is the structural and functional unit of the kidney; each kidney contains approximately one million nephrons. The glomerulus sits at the proximal end of each nephron within Bowman space.
Glomerular capillary tuft: A network of fenestrated capillaries supplied by an afferent arteriole and drained by an efferent arteriole. The fenestrae (60–80 nm pores) allow bulk plasma water to pass but retain cells.
Mesangium: A central scaffold of mesangial cells and matrix that supports the capillary loops. Mesangial cells are contractile (regulate capillary surface area), phagocytic (clear immune complexes), and proliferate in many glomerular diseases. Mesangial expansion is an early marker of diabetic nephropathy.
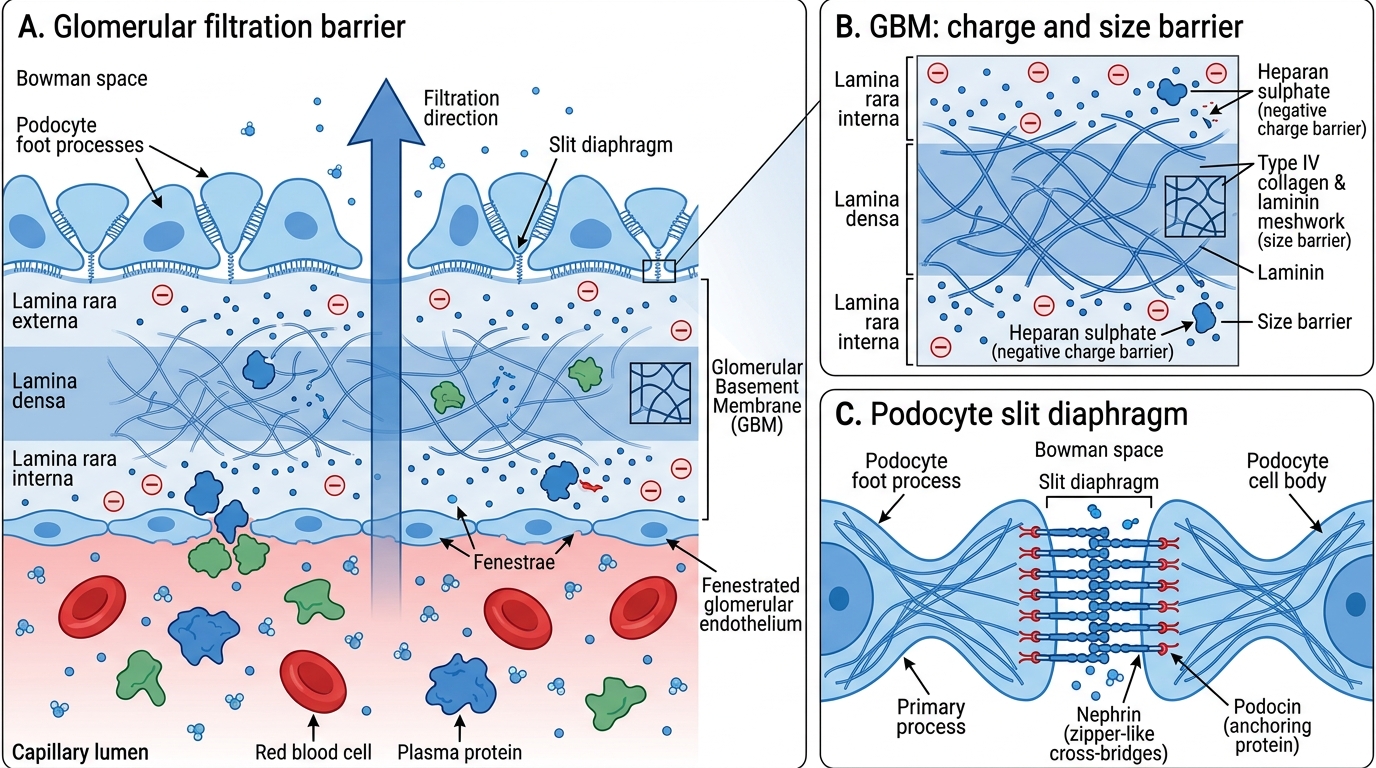
The three-layer filtration barrier (high-yield for MCQs and biopsy interpretation):
1. Fenestrated endothelium — size barrier (excludes RBCs and large proteins).
2. Glomerular basement membrane (GBM) — type IV collagen + laminin + heparan sulphate proteoglycans; the charge barrier (repels anionic albumin).
3. Podocytes and foot processes — podocytes are highly specialised epithelial cells whose interdigitating foot processes are bridged by the slit diaphragm (nephrin protein). Effacement (flattening) of foot processes is the ultrastructural hallmark of nephrotic-range proteinuria.
Bowman capsule: A double-walled cup. The visceral layer = podocytes; the parietal layer = simple squamous epithelium. Bowman space collects the ultrafiltrate. In rapidly progressive GN, the parietal epithelium proliferates to form crescents — covered in SDL 2.
IMG: 3-layer filtration barrier — use this marker for an annotated diagram
Glomerular Filtration Barrier
Nephron Architecture: Tubular Segments and JGA
Nephron Tubular Segments and Juxtaglomerular Apparatus
Beyond Bowman space the filtrate travels through four functionally distinct tubular segments.
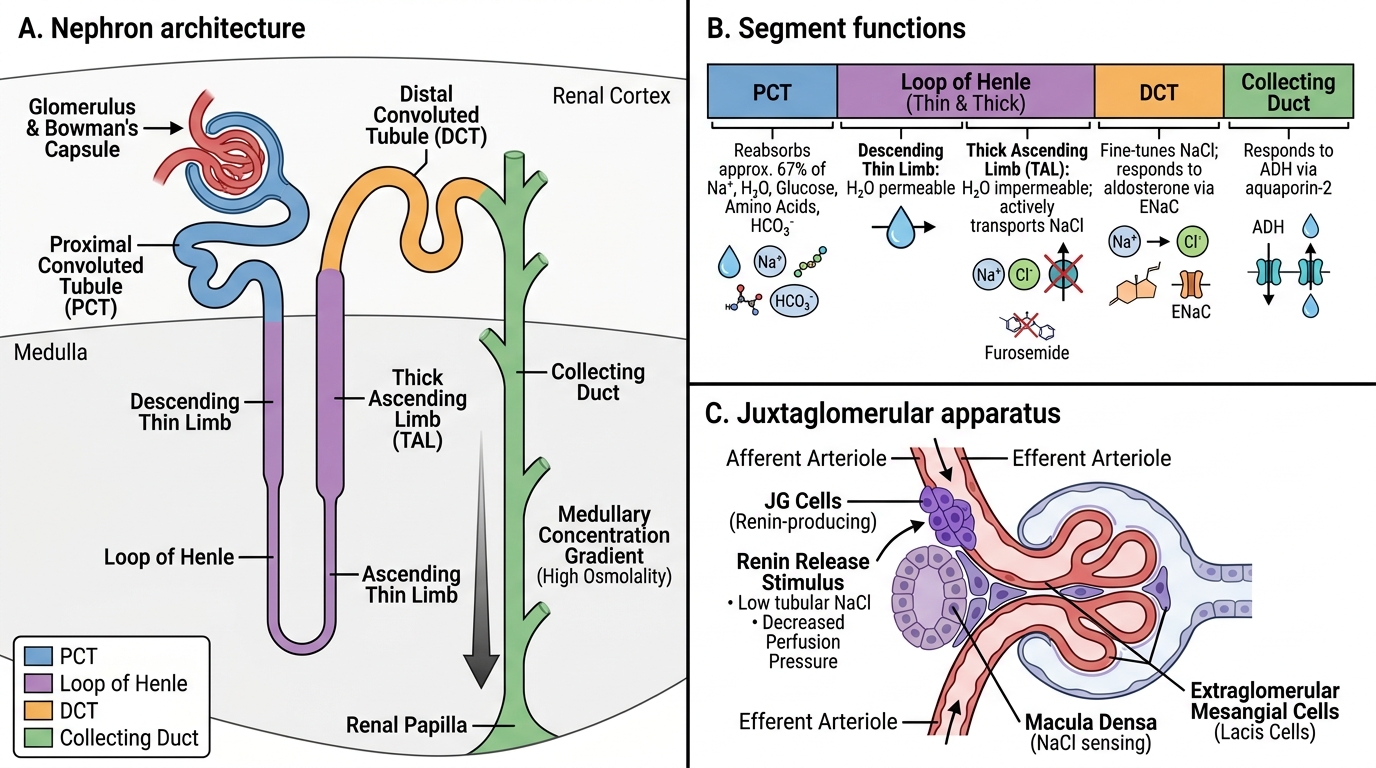
Proximal convoluted tubule (PCT): Reabsorbs ~67% of filtered Na⁺, water, glucose, amino acids, and bicarbonate. Lined by tall cells with a brush border (microvilli) visible on light microscopy — the highest metabolic demand of any tubular segment, making it the most vulnerable to ischaemia and toxins.
Loop of Henle: Descending thin limb (permeable to water), ascending thin limb, and thick ascending limb (TAL; impermeable to water, actively transports NaCl). Creates the medullary concentration gradient. The TAL is the target of loop diuretics (furosemide).
Distal convoluted tubule (DCT): Fine-tunes NaCl reabsorption; aldosterone acts here (via ENaC channels) to retain Na⁺ and secrete K⁺.
Collecting duct: Final water reabsorption under ADH (aquaporin-2 insertion). Passes through the medulla to the renal papilla.
Juxtaglomerular apparatus (JGA): A specialised zone at the vascular pole of the glomerulus comprising:
- Juxtaglomerular (JG) cells in the afferent arteriole wall — store and secrete renin in response to decreased perfusion pressure or low tubular NaCl.
- Macula densa — a patch of modified DCT cells that sense luminal NaCl concentration and signal JG cells.
- Extraglomerular mesangial (lacis) cells — bridging cells with uncertain function.
IMG: nephron segments overview
Full Nephron and Cortex-Medulla Organisation
Cortex vs Medulla — The Zonal Organisation
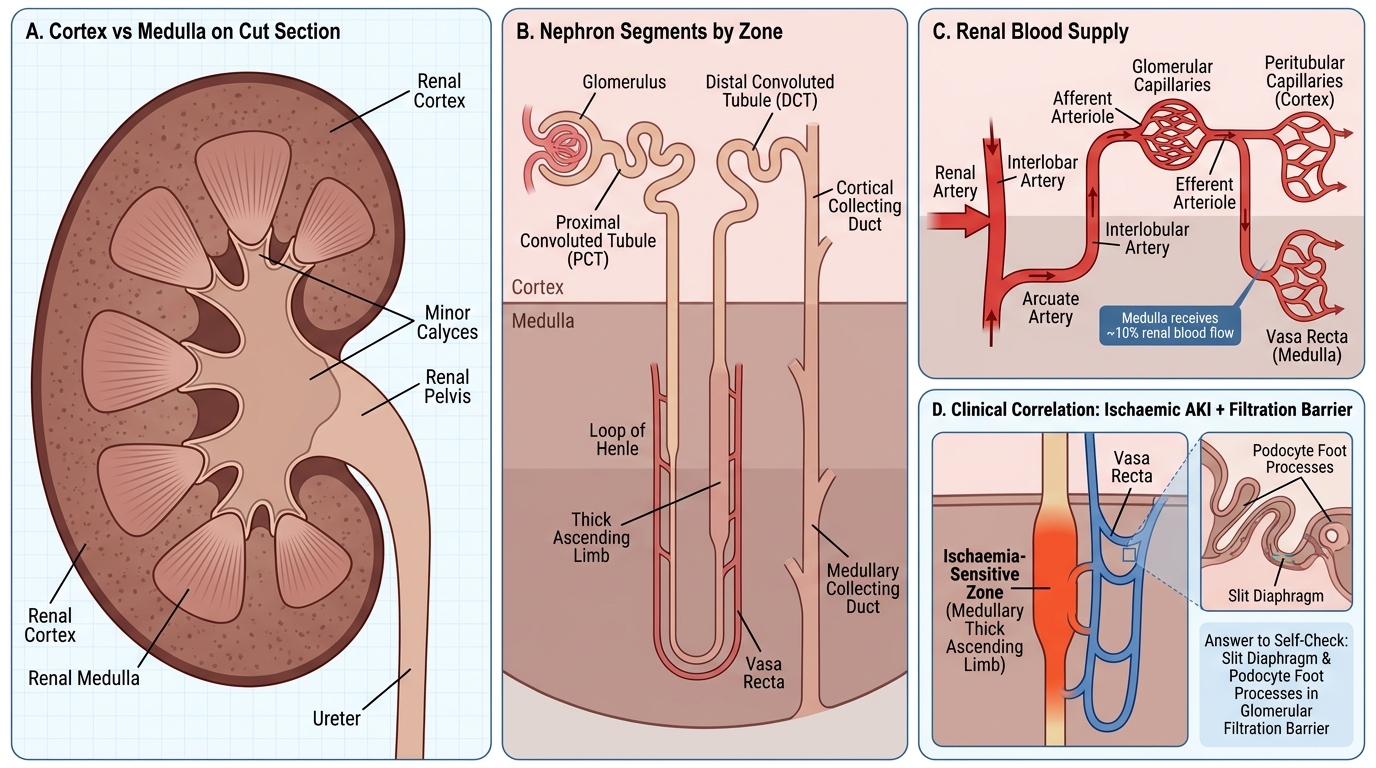
Cortex vs Medulla: Zonal Organisation of the Kidney
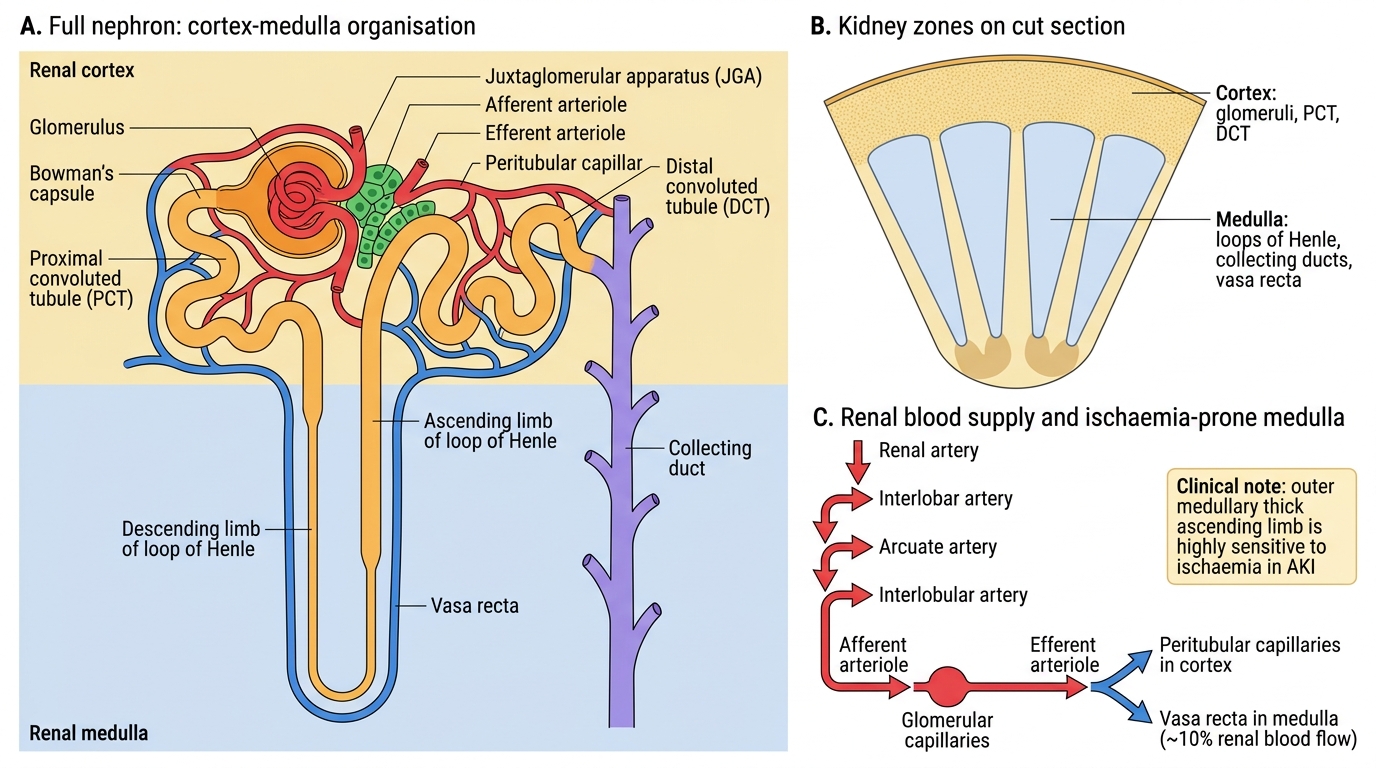
The kidney is organised into two zones visible on cut section.
Cortex (outer zone, ~1 cm thick): Contains all glomeruli, all PCTs, all DCTs, and the outer medullary collecting ducts. The cortex is the denser, granular-appearing zone. Because it houses the glomeruli and metabolically active PCTs, most glomerular and tubular diseases affect the cortex primarily.
Medulla (inner zone, pyramids): Contains the loops of Henle, collecting ducts, and the vasa recta (medullary capillaries that maintain the osmotic gradient by countercurrent exchange). The medullary pyramids open at the renal papilla into the minor calyces.
Blood supply (clinically important):
- Renal artery → interlobar → arcuate → interlobular arteries → afferent arterioles → glomerular capillaries → efferent arterioles → peritubular capillaries (cortex) / vasa recta (medulla).
- The medulla receives only ~10% of renal blood flow via the vasa recta. This makes the medullary thick ascending limb (outer medulla) exquisitely sensitive to ischaemia — the site of injury in ischaemic AKI.
SELF-CHECK
A renal biopsy shows diffuse effacement of foot processes on electron microscopy with no immune deposits. Which component of the filtration barrier is primarily disrupted?
A. Podocyte slit diaphragm
B. Fenestrated endothelium
C. Glomerular basement membrane (GBM)
D. Mesangial matrix
Reveal Answer
Answer: A. Podocyte slit diaphragm
Foot process effacement (flattening/fusion) disrupts the slit diaphragm formed by nephrin between adjacent podocyte foot processes. This is the hallmark ultrastructural finding in minimal change disease (the most common nephrotic syndrome in children). The GBM and endothelium are intact; mesangial changes would not explain protein leakage of this pattern.