Page 2 of 25
PA27.1-2 | Normal Kidney & Clinical Syndromes — SDL Guide (Part 2)
The Renal Clinical Syndromes — Framework Overview
Urinalysis Framework for Renal Clinical Syndromes
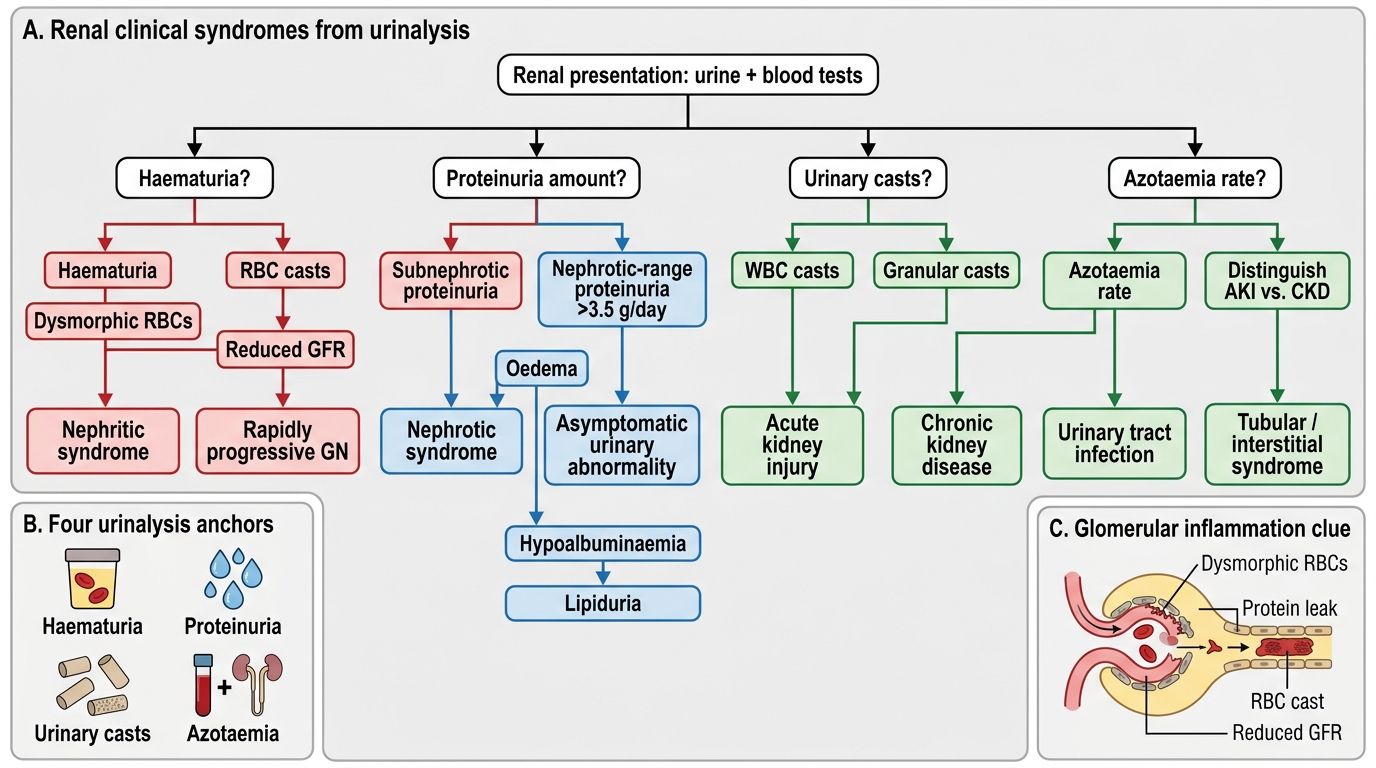
A renal clinical syndrome is a constellation of signs, symptoms, and urinalysis findings that points to a pathophysiological mechanism and a disease category — before histology is available. Eight syndromes cover nearly all renal presentations. Mastering them lets you generate a differential before the biopsy report arrives.
The framework rests on four urinalysis parameters:
1. Haematuria (RBCs in urine) — present/absent; dysmorphic RBCs indicate glomerular origin.
2. Proteinuria — subnephrotic (<3.5 g/day) vs nephrotic-range (>3.5 g/day).
3. Urinary casts — cylindrical moulds formed in tubular lumina; their cellular content identifies the injury zone.
4. Azotaemia — elevated serum creatinine/urea indicating reduced GFR; rate of rise distinguishes AKI from CKD.
IMG: syndrome classification map
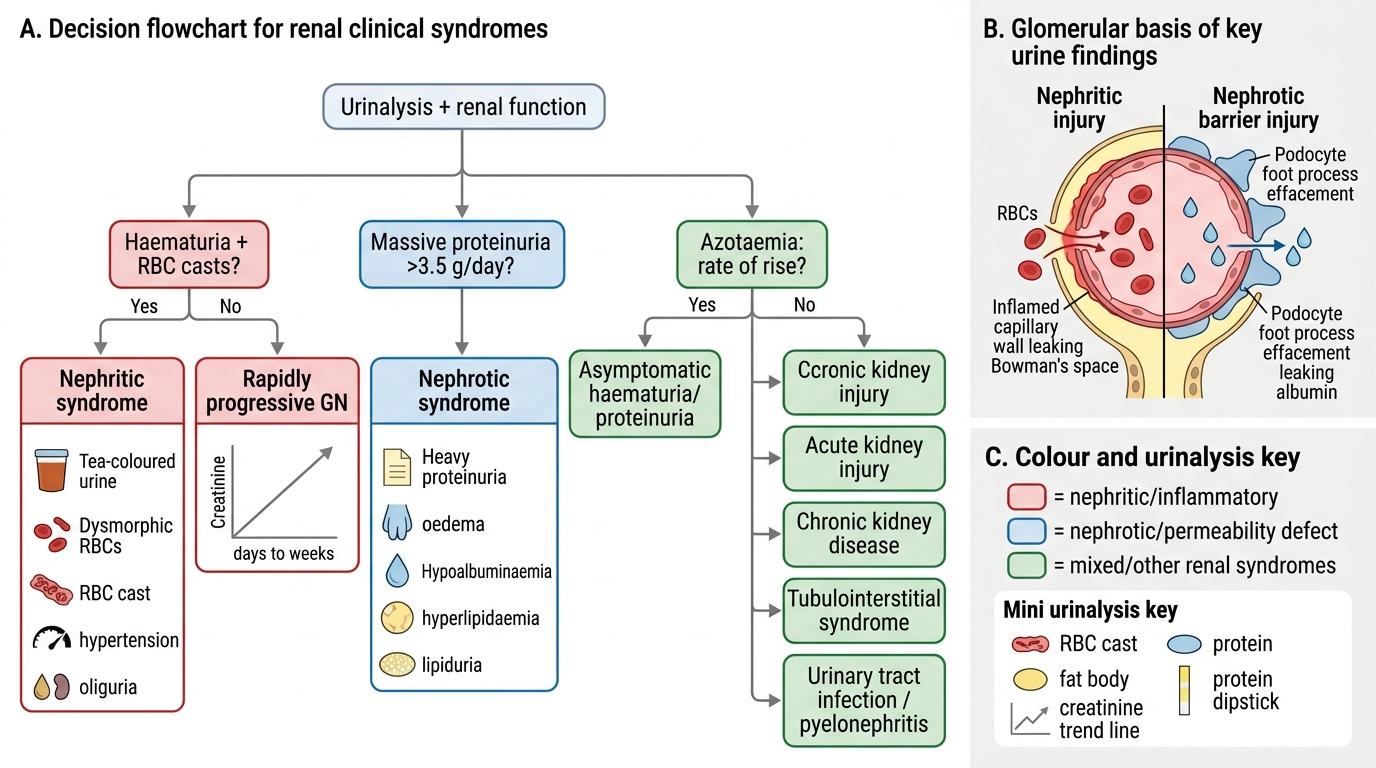
Urinalysis Decision Flowchart for Renal Clinical Syndromes
Nephritic Syndrome
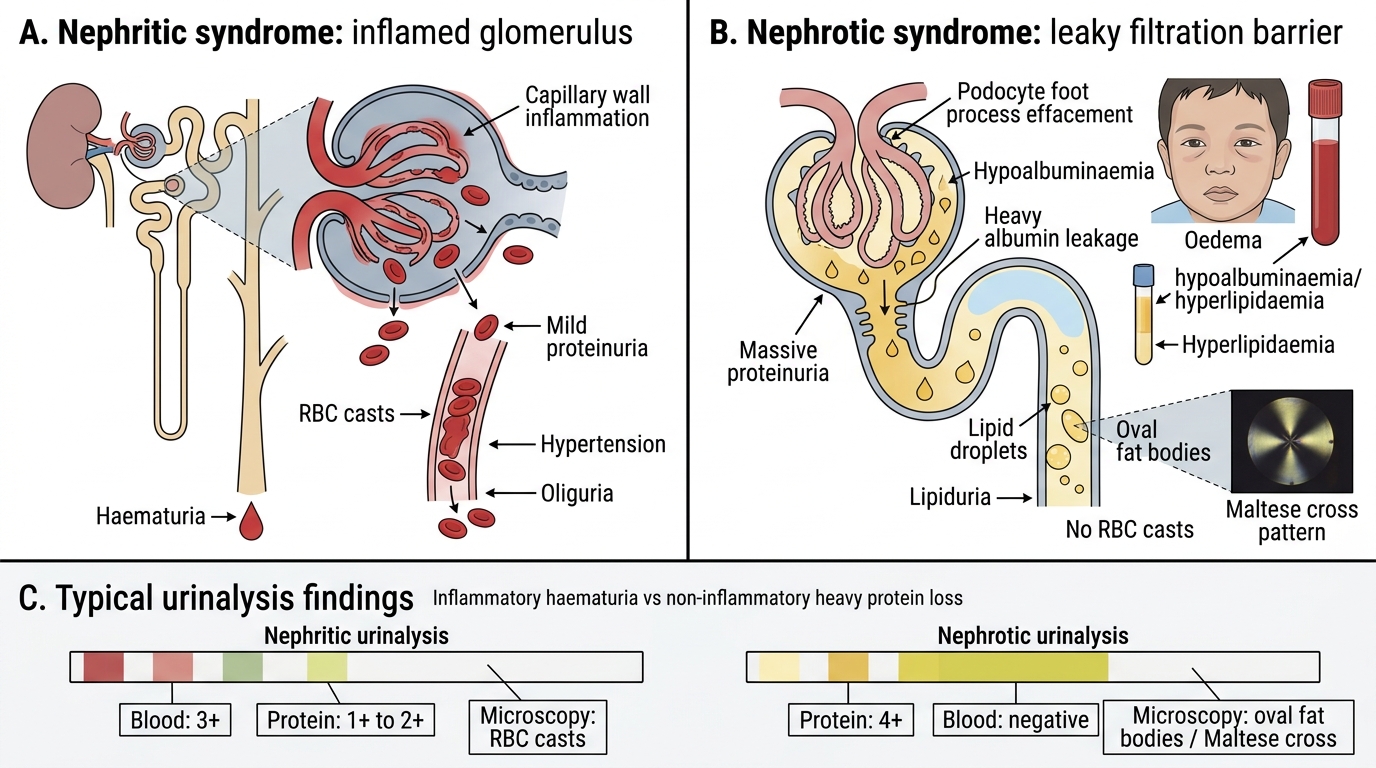
Nephritic syndrome is the prototypical presentation of glomerular inflammation. Inflammation disrupts capillary walls, allowing RBCs and protein to leak while reducing GFR.
Hallmark features (all five must be considered):
- Haematuria — macroscopic (tea-coloured or smoky urine) or microscopic; dysmorphic RBCs (acanthocytes) indicate passage through the damaged GBM.
- RBC casts in urine — pathognomonic of glomerulonephritis. RBCs trapped in Tamm-Horsfall protein matrix within the tubule lumen form cylindrical casts.
- Mild-to-moderate proteinuria — typically <3.5 g/day; the GBM is inflamed but not completely destroyed.
- Hypertension — due to Na⁺/water retention from reduced GFR + RAAS activation.
- Oliguria and azotaemia — reduced urine output and rising creatinine from fall in GFR.
Prototype diseases: post-streptococcal GN, IgA nephropathy (Berger disease), lupus nephritis (Class III/IV), membranoproliferative GN.
Key distinction: In nephritic syndrome the problem is inflammation reducing filtration, so haematuria and azotaemia dominate. Proteinuria is secondary, not massive.
Nephrotic Syndrome
Nephrotic Syndrome: Barrier Dysfunction and Consequences
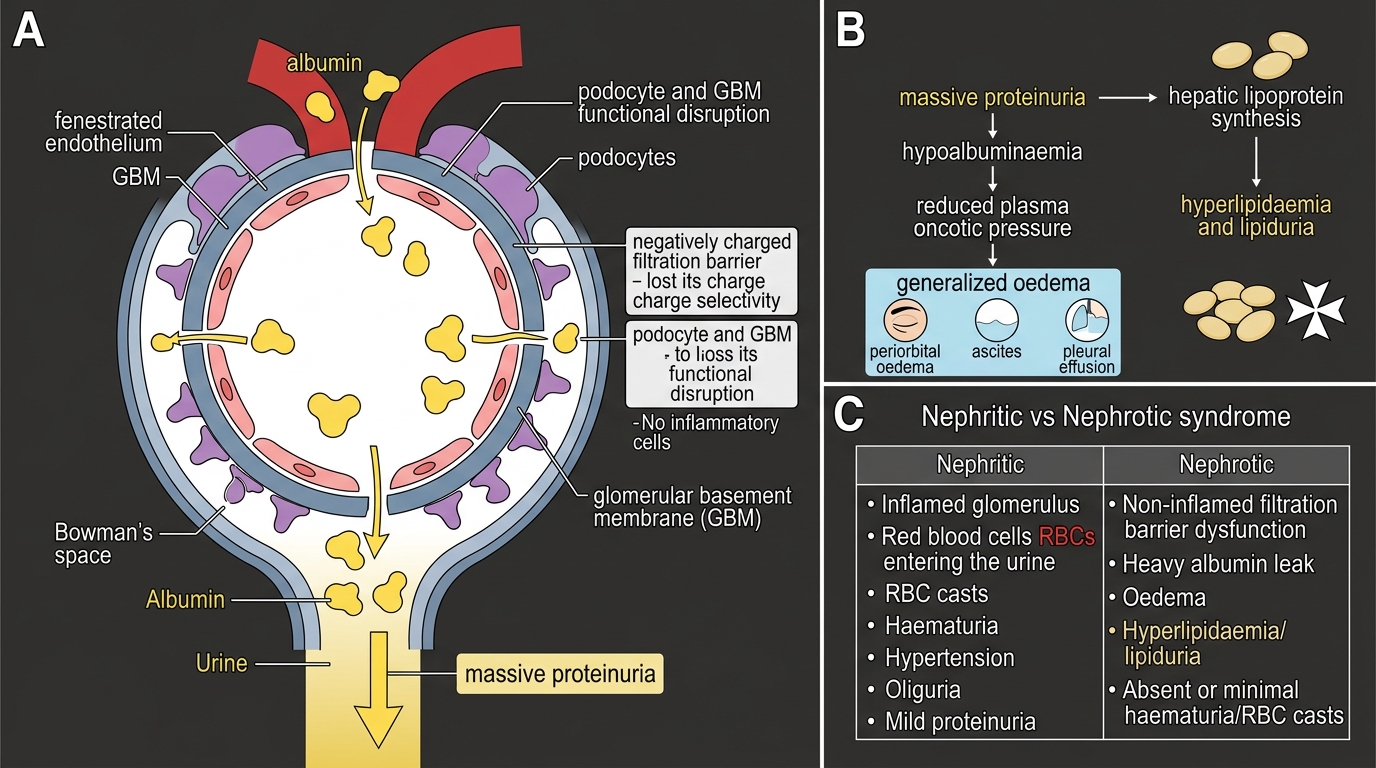
Nephrotic syndrome results from glomerular diseases that disrupt the filtration barrier's permselectivity — particularly the charge barrier — without (initially) causing inflammation.
Four defining features:
- Massive proteinuria >3.5 g/day (in practice >3 g/day in adults) — the sine qua non.
- Hypoalbuminaemia — albumin lost in urine faster than the liver can synthesise it.
- Generalised oedema — reduced plasma oncotic pressure; fluid shifts to the interstitium (periorbital oedema, ascites, pleural effusion).
- Hyperlipidaemia and lipiduria — compensatory hepatic lipoprotein synthesis; lipid casts and oval fat bodies (Maltese cross pattern under polarised light) in urine.
Additional complications: hypercoagulability (antithrombin III lost in urine → renal vein thrombosis), susceptibility to encapsulated organism infections (IgG lost), vitamin D deficiency (vitamin D–binding protein lost).
Prototype diseases: Minimal change disease (children), focal segmental glomerulosclerosis (FSGS; adults), membranous nephropathy, diabetic nephropathy (advanced).
Key distinction: In nephrotic syndrome the GBM/podocytes are functionally disrupted but not inflamed — haematuria and RBC casts are absent or minimal. Proteinuria and its downstream consequences dominate.
IMG: nephritic vs nephrotic comparison
Nephritic vs Nephrotic Syndrome
SELF-CHECK
A 6-year-old boy presents with puffy eyes on waking and frothy urine. His urine dipstick shows 4+ protein with no blood. Serum albumin is 1.8 g/dL. Which urinalysis finding would be MOST characteristic of his condition?
A. RBC casts
B. Granular casts
C. Oval fat bodies (Maltese cross under polarised light)
D. WBC casts
Reveal Answer
Answer: C. Oval fat bodies (Maltese cross under polarised light)
This is classic nephrotic syndrome (massive proteinuria, hypoalbuminaemia, oedema). The hallmark urinary finding in nephrotic syndrome is lipiduria — oval fat bodies derived from tubular reabsorption of filtered lipoproteins; they show a Maltese cross birefringence pattern under polarised light. RBC casts indicate glomerular inflammation (nephritic). WBC casts suggest pyelonephritis or interstitial nephritis. Granular casts are non-specific and appear in many tubular injuries.