Page 3 of 25
PA27.1-2 | Normal Kidney & Clinical Syndromes — SDL Guide (Part 3)
The Other Six Renal Clinical Syndromes
The Other Six Renal Clinical Syndromes
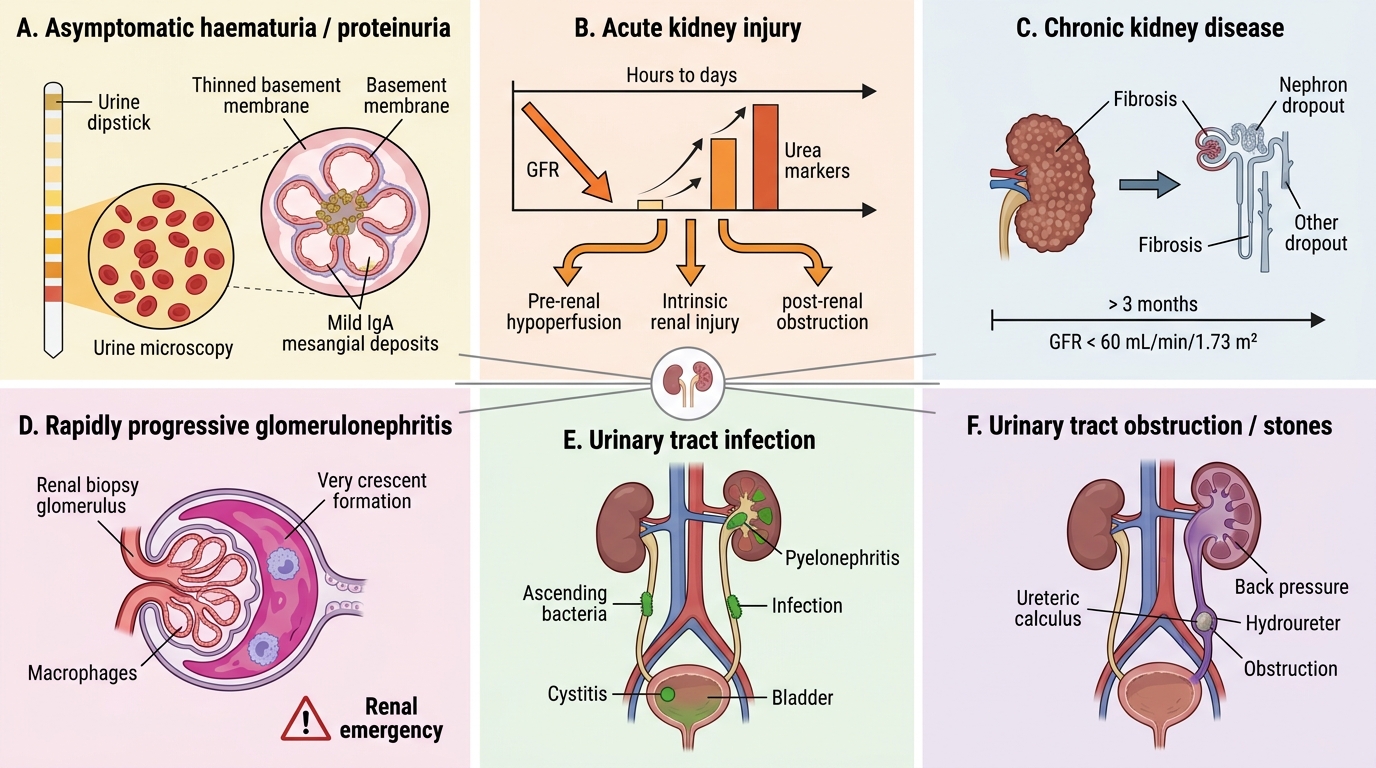
1. Asymptomatic haematuria / proteinuria: Isolated urinary abnormalities without systemic features. Subnephrotic proteinuria (<1 g/day) or microscopic haematuria found incidentally. Common causes: IgA nephropathy (most common GN worldwide), thin basement membrane disease, early hereditary nephritis (Alport syndrome).
2. Acute kidney injury (AKI): Rapid (hours to days) decline in GFR producing azotaemia (rising creatinine and urea) with or without oliguria (<400 mL/day). Causes are classified as pre-renal (hypoperfusion), intrinsic renal (tubular, glomerular, interstitial, vascular), or post-renal (obstruction). The key question: is the kidney salvageable? (covered in SDL 3).
3. Chronic kidney disease (CKD): Progressive, usually irreversible loss of GFR over months to years. GFR <60 mL/min/1.73m² for >3 months defines CKD. Ultimately produces uraemia — the clinical syndrome of accumulation of nitrogenous waste products (urea, creatinine, guanidino compounds) causing encephalopathy, pericarditis, platelet dysfunction, anaemia (EPO deficiency), and renal osteodystrophy.
4. Rapidly progressive glomerulonephritis (RPGN): A nephritic syndrome that deteriorates to renal failure within weeks to months. Histological hallmark: crescents in >50% of glomeruli (proliferating parietal epithelial cells ± macrophages). A renal emergency. Causes: anti-GBM disease (Goodpasture), ANCA-associated vasculitis, immune complex GN.
5. Urinary tract infection (UTI): Dysuria, frequency, bacteriuria, pyuria (WBC casts if pyelonephritis). Not primarily a glomerular disease. WBC casts in urine → upper tract infection (pyelonephritis) or acute interstitial nephritis.
6. Nephrolithiasis (renal stones): Flank pain, haematuria, no proteinuria, no casts. Stones classified by composition: calcium oxalate/phosphate (most common), uric acid, struvite (infection stones), cystine.
Urinary Casts — Reading the Urine Microscopy
Urinary Casts in Urine Microscopy
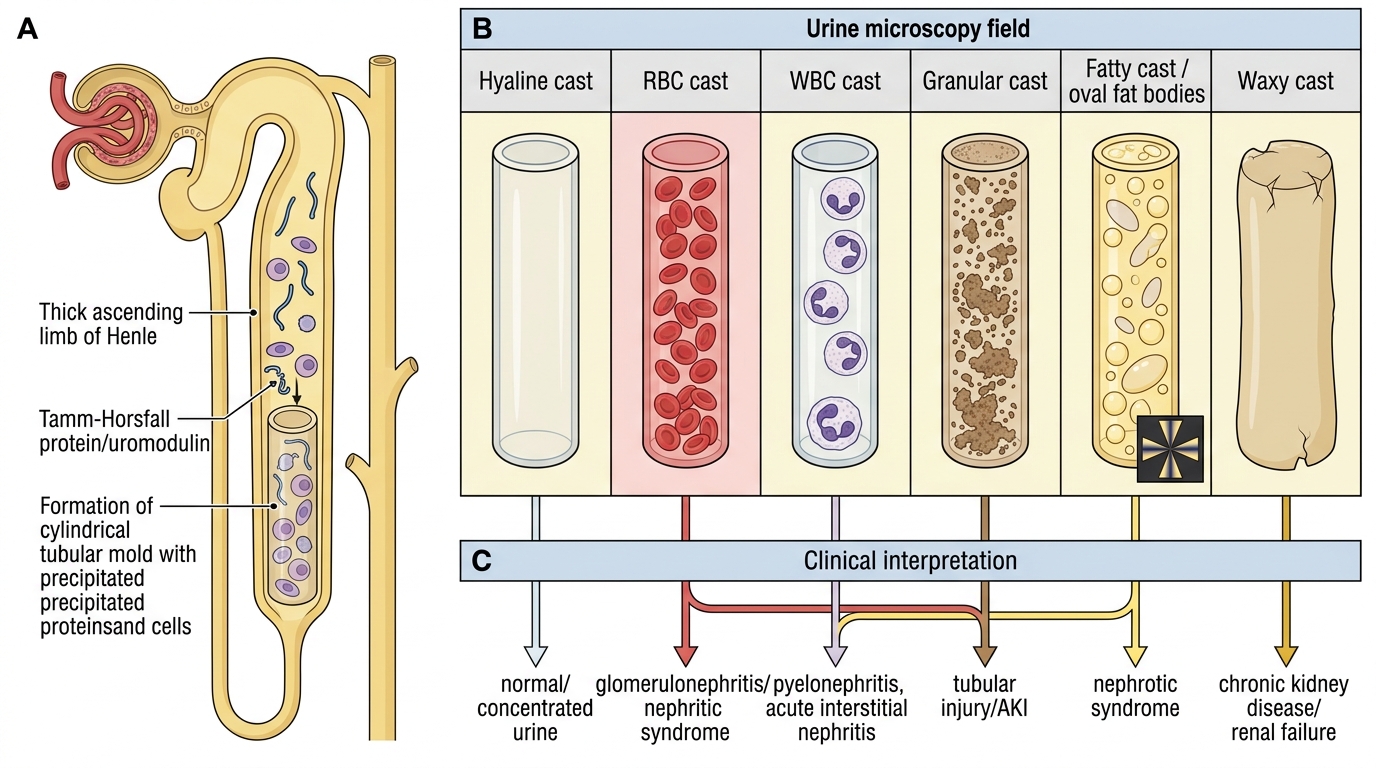
Urinary casts are cylindrical structures formed when proteins or cells precipitate within the tubular lumen, moulded by the tubule shape. All casts have a Tamm-Horsfall protein (uromodulin) matrix secreted by the TAL of Henle.
Cast types and their clinical significance:
| Cast type | Appearance | Significance |
|---|---|---|
| Hyaline casts | Pale, homogeneous | Non-specific; normal in small numbers, concentrated urine |
| RBC casts | Red-tinged, packed with RBCs | Pathognomonic of glomerulonephritis (nephritic syndrome) |
| WBC casts | White cells embedded | Pyelonephritis or acute interstitial nephritis |
| Granular casts | Coarse or fine granules | Non-specific tubular injury; in abundance → AKI |
| Fatty casts / oval fat bodies | Lipid droplets, Maltese cross | Nephrotic syndrome |
| Waxy / broad casts | Waxy, wide diameter | Advanced CKD — form in dilated atrophic tubules |
| Epithelial cell casts | Renal tubular cells | Acute tubular necrosis (ischaemic or toxic AKI) |
IMG: urinary casts microscopy panel
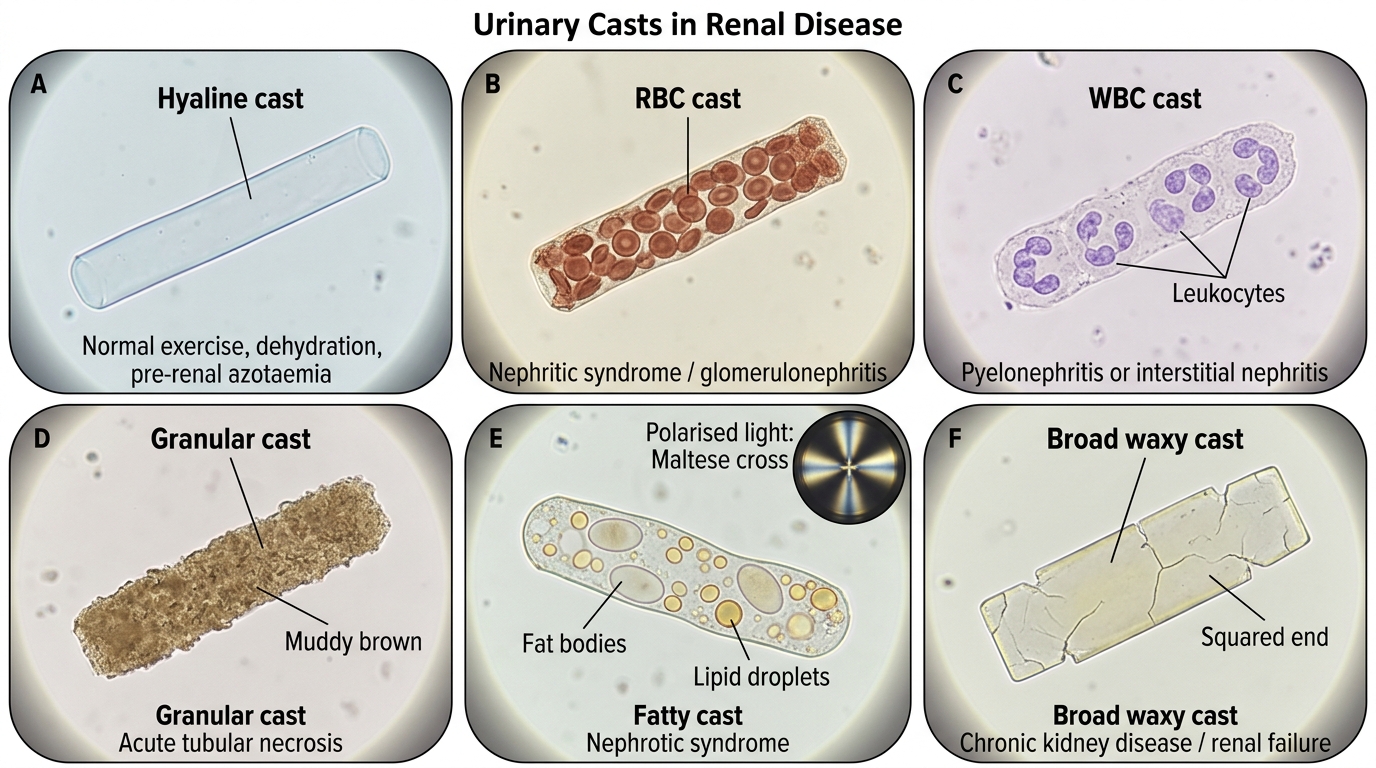
Urinary Casts and Clinical Associations
Azotaemia vs Uraemia — A Critical Distinction
Azotaemia vs Uraemia
Two terms that are often conflated but have distinct meanings:
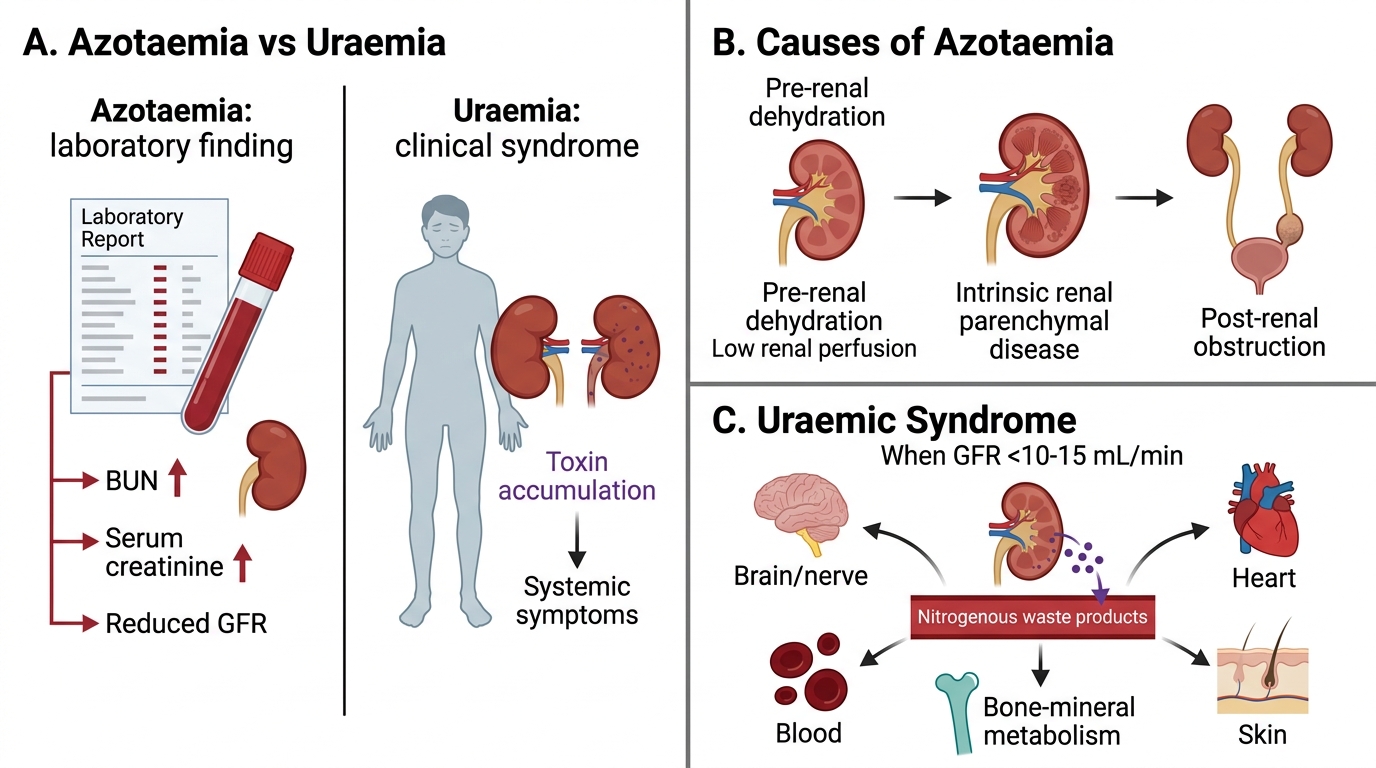
Azotaemia is a laboratory finding: elevated blood urea nitrogen (BUN) and serum creatinine reflecting reduced GFR. It is asymptomatic by itself and can be pre-renal (dehydration), renal (parenchymal disease), or post-renal (obstruction).
Uraemia is a clinical syndrome: the constellation of symptoms caused by accumulation of nitrogenous waste products and metabolic derangements when GFR falls to <10–15 mL/min. Features:
- Neurological: encephalopathy, asterixis, peripheral neuropathy
- Cardiovascular: uraemic pericarditis (friction rub), accelerated atherosclerosis
- Haematological: normochromic normocytic anaemia (↓ EPO), platelet dysfunction (bleeding tendency)
- Metabolic: hyperphosphataemia → secondary hyperparathyroidism → renal osteodystrophy; metabolic acidosis; hyperkalaemia
- Dermatological: uraemic frost (urea crystallisation on skin), pruritus
Mnemonic: Azotaemia = a lab value (BUN/Cr up). Uraemia = Unwell patient (symptoms of toxin accumulation).
Pre-renal azotaemia has a BUN:Cr ratio >20:1 (urea is reabsorbed passively with water in concentrated urine); intrinsic renal azotaemia has BUN:Cr ~10-15:1.
SELF-CHECK
A 55-year-old with longstanding diabetes presents with serum creatinine 6.8 mg/dL (baseline 1.0 mg/dL one year ago), BUN 98 mg/dL, haemoglobin 8.2 g/dL, and asterixis on exam. Which term BEST describes his condition?
A. Pre-renal azotaemia
B. Nephrotic syndrome
C. Asymptomatic azotaemia
D. Uraemia
Reveal Answer
Answer: D. Uraemia
This patient has symptomatic end-stage renal disease. Uraemia is the correct term because he has clinical manifestations (asterixis = metabolic encephalopathy, anaemia from EPO deficiency) caused by accumulation of nitrogenous waste products, not merely a lab abnormality. Pre-renal azotaemia would have a BUN:Cr >20:1 and respond to fluids. 'Asymptomatic azotaemia' is a contradiction here given his neurological and haematological findings. Nephrotic syndrome is characterised by massive proteinuria and oedema, not encephalopathy or anaemia.