Page 4 of 25
PA27.1-2 | Normal Kidney & Clinical Syndromes — SDL Guide (Part 4)
Mapping Findings to Syndromes — A Clinical Decision Framework
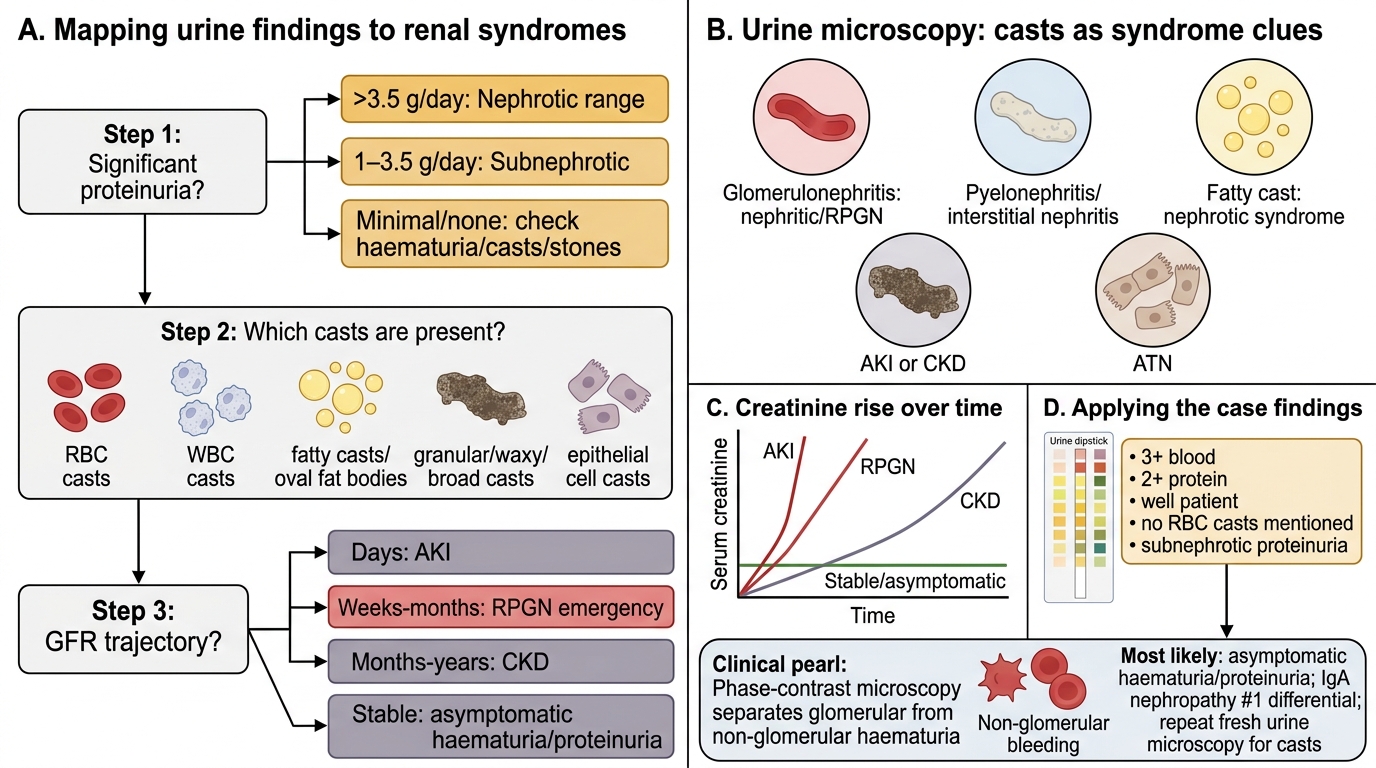
Urine Findings to Renal Syndrome: A Three-Step Framework
When you face a urine dipstick + microscopy result, apply this three-question algorithm:
Step 1 — Is there significant proteinuria?
- >3.5 g/day → Nephrotic range → suspect nephrotic syndrome
- 1–3.5 g/day → Subnephrotic → consider nephritic, asymptomatic, AKI, RPGN
- Minimal/none → look for haematuria, casts, or stone
Step 2 — What casts are present?
- RBC casts → glomerulonephritis (nephritic, RPGN)
- WBC casts → pyelonephritis or interstitial nephritis
- Fatty casts / oval fat bodies → nephrotic syndrome
- Granular / waxy / broad → AKI or CKD
- Epithelial cell casts → acute tubular necrosis
Step 3 — What is the GFR trajectory?
- Sudden rise in creatinine (days) → AKI
- Rapid rise (weeks–months) + glomerulitis → RPGN (emergency)
- Slow rise (months–years) → CKD
- Stable, normal → asymptomatic haematuria/proteinuria
Applying to the opening case: 3+ blood, 2+ protein, well patient. No RBC casts were mentioned; proteinuria is subnephrotic. Most likely: asymptomatic haematuria/proteinuria — IgA nephropathy is #1 on the differential. A repeat urine with microscopy for casts would be the next step. SDL 2 will reveal the diagnosis.
CLINICAL PEARL
The one test that separates glomerular from non-glomerular haematuria: Phase-contrast microscopy of a fresh urine specimen. Dysmorphic RBCs (acanthocytes — spiky, irregular-shaped RBCs distorted by passage through the damaged GBM) indicate glomerular bleeding. Isomorphic RBCs (normal biconcave discs) suggest lower urinary tract bleeding (stone, tumour, infection). A finding of >5% acanthocytes has ~95% specificity for glomerulonephritis. This single test can save the patient a cystoscopy.