Page 11 of 27
PA27.12-13 | Cystic Kidney Disease, Renal Stones & Obstructive Uropathy — SDL Guide (Part 3)
Hydronephrosis — Morphology and Grades
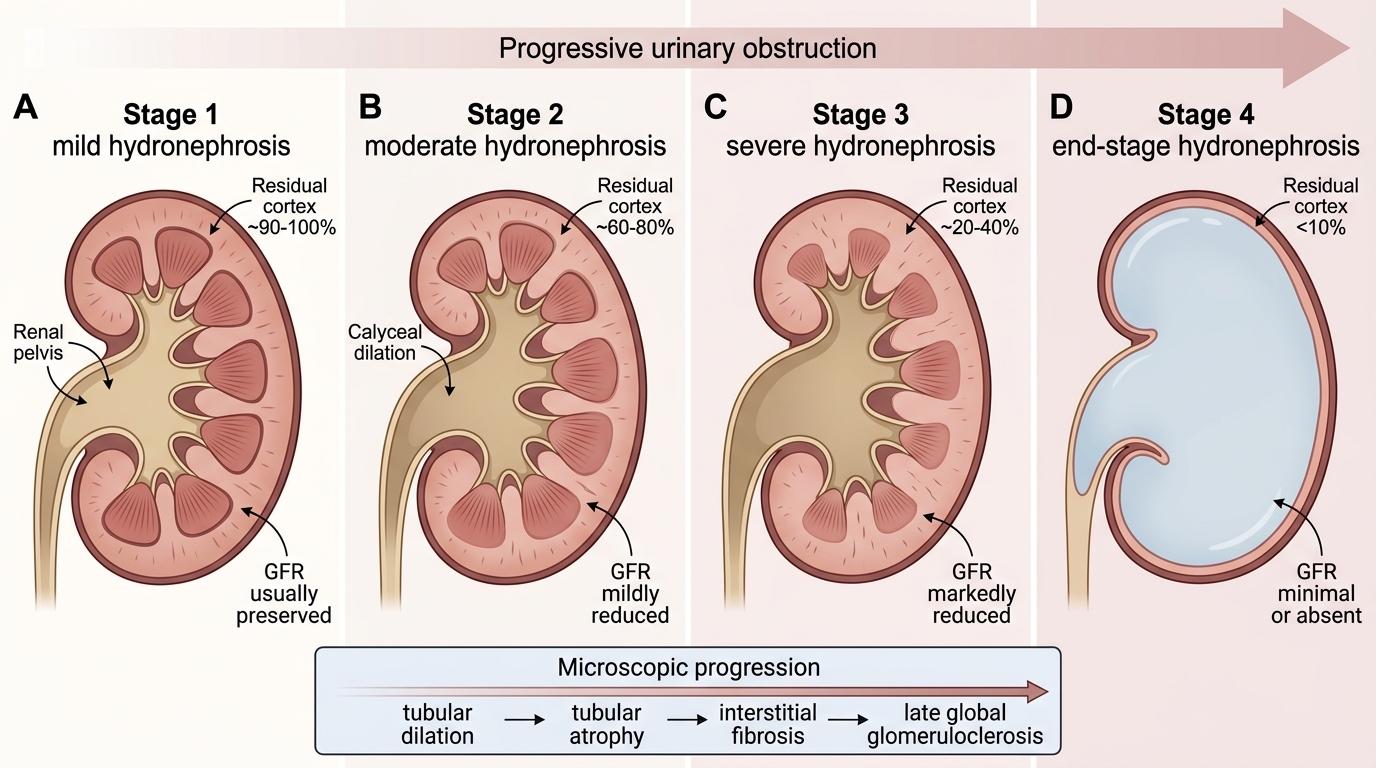
Morphological Grades of Hydronephrosis
Morphological appearance:
Gross: The renal pelvis and calyces are progressively dilated. In early obstruction, only the pelvis is dilated (pelvicaliectasis). In advanced disease, the kidney is converted into a large, thin-walled sac of fluid — the cortex is reduced to a thin rim.
Cut section shows:
- Dilation of calyces → blunting of papillae → progressive papillary atrophy.
- Cortical thinning (normal cortex ~10–12 mm; advanced hydronephrosis may reduce this to 1–2 mm).
- In complete obstruction, the parenchyma is entirely replaced by fibrous tissue and fluid.
Microscopy: Tubular dilation → tubular atrophy → interstitial fibrosis → glomeruli initially spared then globally sclerosed in late stages.
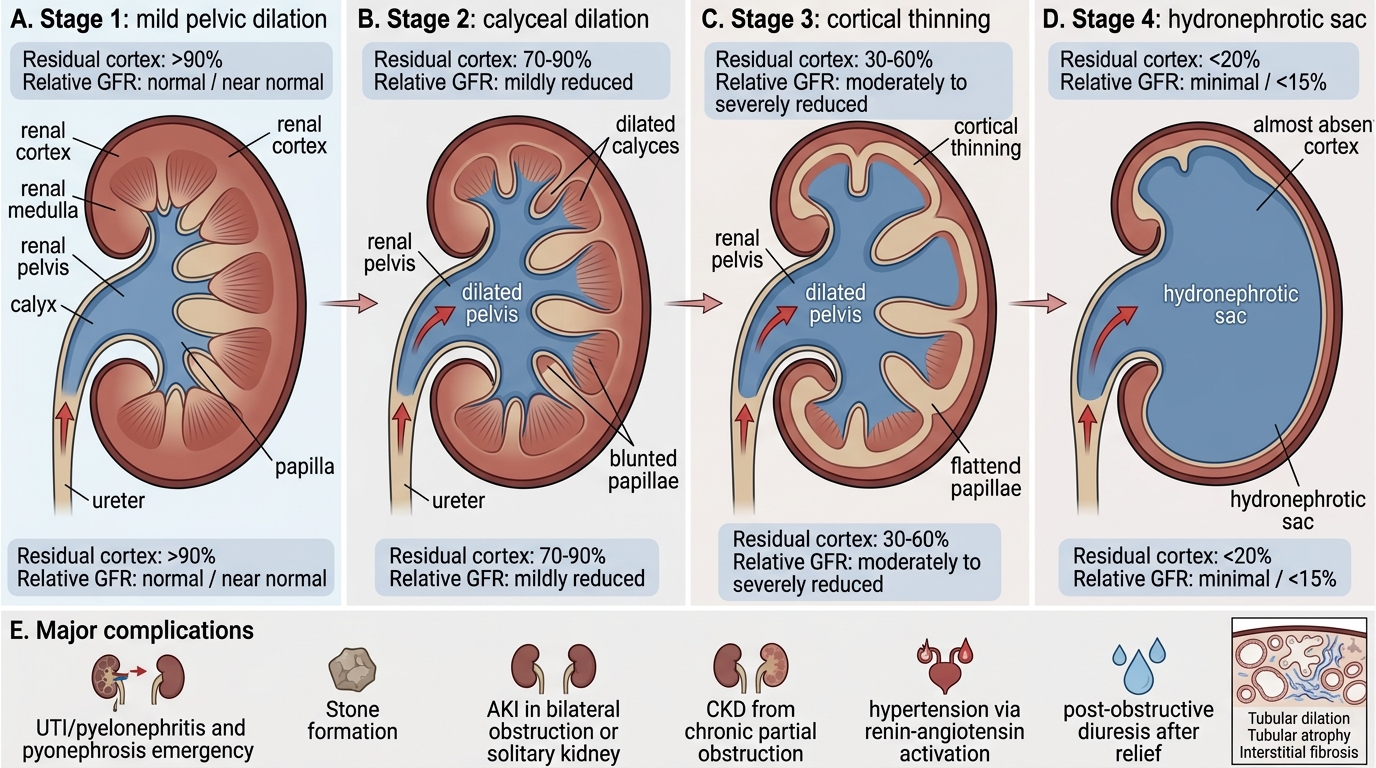
Progression and Complications of Hydronephrosis
Complications of obstructive uropathy:
1. Urinary tract infection → pyelonephritis — stasis promotes bacterial growth; if infected → pyonephrosis (pus-filled hydronephrotic kidney) — surgical emergency.
2. Stone formation — stasis promotes nucleation and crystallisation.
3. AKI — bilateral obstruction or obstruction in a solitary functioning kidney.
4. CKD — chronic partial obstruction is a silent cause of progressive renal impairment.
5. Hypertension — activation of the renin–angiotensin system.
6. Post-obstructive diuresis — after relief of bilateral obstruction, massive salt and water diuresis; requires careful fluid and electrolyte replacement.
SELF-CHECK
A 65-year-old man with BPH presents with bilateral hydroureteronephrosis and raised serum creatinine. Biopsy of the renal cortex would most likely show:
A. Proliferative glomerulonephritis with immune complex deposits
B. Tubular dilation, tubular atrophy, and interstitial fibrosis
C. Necrotising vasculitis of arcuate arteries
D. Diffuse mesangial IgA deposition
Reveal Answer
Answer: B. Tubular dilation, tubular atrophy, and interstitial fibrosis
Obstructive uropathy from BPH causes back-pressure ischaemia and tubular injury. The histological hallmarks are tubular dilation (early) progressing to tubular atrophy and interstitial fibrosis (late) — collectively called obstructive nephropathy. Glomeruli are relatively preserved until late stages. Proliferative GN, vasculitis, and IgA nephropathy are immunologically mediated, not obstructive in mechanism.
Distinguishing ADPKD from Other Cystic Diseases — A Framework
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
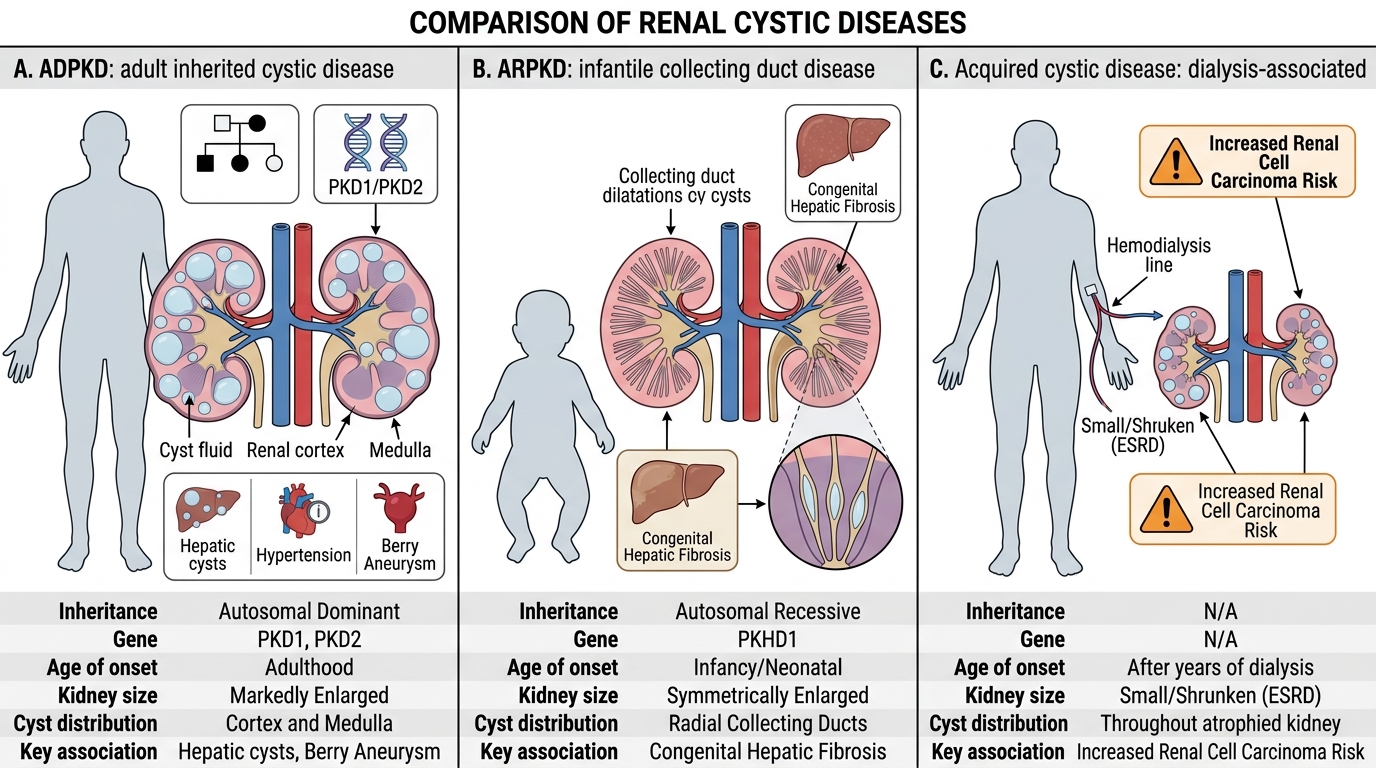
Framework for Distinguishing Cystic Kidney Diseases
Examiners frequently ask you to distinguish ADPKD from ARPKD and from acquired cystic disease. Use this framework:
| Feature | ADPKD | ARPKD | Acquired Cystic Disease |
|---|---|---|---|
| Inheritance | Autosomal dominant | Autosomal recessive | Acquired (dialysis) |
| Gene | PKD1/PKD2 | PKHD1 | Somatic |
| Age of onset | 4th–5th decade | Perinatal / infantile | After 5–10 yrs dialysis |
| Cyst distribution | Bilateral, all segments | Bilateral, collecting ducts | Bilateral, cortex/medulla |
| Cyst size | Large, varied (mm–cm) | Tiny, radial sponge | Small–medium |
| Associated lesion | Berry aneurysm, hepatic cysts, MVP | Congenital hepatic fibrosis | ↑ RCC risk |
| ESRD timing | 5th–6th decade | Childhood (severe forms) | Already in ESRD |
| Key clinical pointer | Family history, palpable kidneys, hypertension, SAH | Neonate / infant, Potter sequence, portal hypertension | Long-term haemodialysis patient |
Simple cortical cysts differ from all of the above: unilateral or few bilateral, large, unilocular, in adults over 50, no genetic basis, no ESRD risk.
SELF-CHECK
In the investigation of nephrolithiasis, which stone type can be dissolved medically by alkalinising the urine, and what is the agent of choice?
A. Calcium oxalate stones — thiazide diuretics reduce urinary calcium
B. Struvite stones — antibiotics eliminate urease-producing organisms
C. Uric acid stones — potassium citrate alkalinises urine above pH 6.5
D. Cystine stones — dietary protein restriction reduces cystine load
Reveal Answer
Answer: C. Uric acid stones — potassium citrate alkalinises urine above pH 6.5
Uric acid stones precipitate in acidic urine (pH <5.5) because uric acid's pKa is 5.5 — below this, the undissociated, insoluble form predominates. Raising urine pH above 6.5 with oral potassium citrate converts uric acid to the soluble urate anion, dissolving existing stones and preventing new ones. Thiazides reduce calcium excretion (useful for calcium oxalate but do not dissolve stones). Struvite stones require surgical removal and antibiotic therapy — they cannot be dissolved medically. Cystine stone management uses D-penicillamine or tiopronin to complex cystine, not diet alone.