Page 17 of 27
PA27.17 | Kidney Disease & Tumour Morphology — Practical — SDL Guide
Learning Objectives
- Describe the systematic approach to reading a renal specimen: gross → compartment → microscopic pattern → diagnosis.
- Identify and describe the gross and microscopic features of glomerular diseases: diabetic nephropathy, crescentic GN, membranous nephropathy, and minimal change disease.
- Identify and describe the histological features of tubulointerstitial diseases: acute tubular necrosis, acute pyelonephritis, and chronic pyelonephritis.
- Identify vascular lesions: benign nephrosclerosis (granular kidney, hyaline arteriolosclerosis) and malignant nephrosclerosis (onion-skin/fibrinoid necrosis).
- Recognise the gross and microscopic appearances of ADPKD, hydronephrosis, clear-cell RCC, Wilms tumour, and urothelial carcinoma.
- Correlate the H&E appearances with immunofluorescence (IF) and electron microscopy (EM) findings where relevant.
INSTRUCTIONS
Practical pattern-recognition is the bridge between textbook knowledge and examination success. In a pathology practical — whether in an MBBS viva, a postgraduate entrance, or clinical practice — you are handed a specimen and asked: 'What is this?' This SDL walks you through a systematic reading strategy, then applies it to every major renal lesion you will encounter. Work through each section actively: pause at the micro_quiz checkpoints before reading the answer, and use the reflection prompts to build your own diagnostic vocabulary. Bring this framework to your next glass-slide or museum-specimen session.
References
- Robbins & Kumar Basic Pathology, 11th ed., Ch 14 (Kidney) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 20 (Kidney & Urinary Tract) (textbook)
- Bancroft's Theory & Practice of Histological Techniques, 8th ed. (Stain protocols) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You pick up a pot containing a kidney. It is small, shrunken, and has a finely granular surface. The cut surface shows thinning of the cortex and small, firm nodules scattered through the parenchyma. The vascular pedicle shows thickened, rubbery arteries.
Three different conditions could plausibly give you this picture — and they each have completely different pathogeneses, prognoses, and complications. By the end of this practical SDL, you will be able to separate them in under two minutes.
WHY THIS MATTERS
PA27.17 requires you to identify and describe features of kidney diseases and tumours in gross and microscopic specimens. This maps directly to:
• University theory-practical examinations (specimen viva, spotting)
• PG entrance MCQs that describe a photomicrograph or gross specimen
• Clinical correlation when a nephrologist asks you to interpret a renal biopsy report
The competency is not about memorising definitions — it is about reading a slide or pot specimen the way a pathologist does: systematically, in layers.
RECALL
Before starting, check you can answer these in 30 seconds:
- Name the four compartments of the kidney examined histologically.
- What does the glomerular filtration barrier consist of? (Three layers)
- What is the difference between nephritic and nephrotic syndrome?
- Where do kidney tumours most commonly arise — cortex or medulla?
(Answers: 1. Glomeruli, tubules, interstitium, blood vessels. 2. Fenestrated endothelium, glomerular basement membrane (GBM), podocyte foot processes. 3. Nephritic = haematuria + oliguria + hypertension + mild proteinuria; nephrotic = heavy proteinuria + oedema + hypoalbuminaemia. 4. Cortex — RCC.)
The Reading Framework: Gross → Compartment → Pattern → Diagnosis
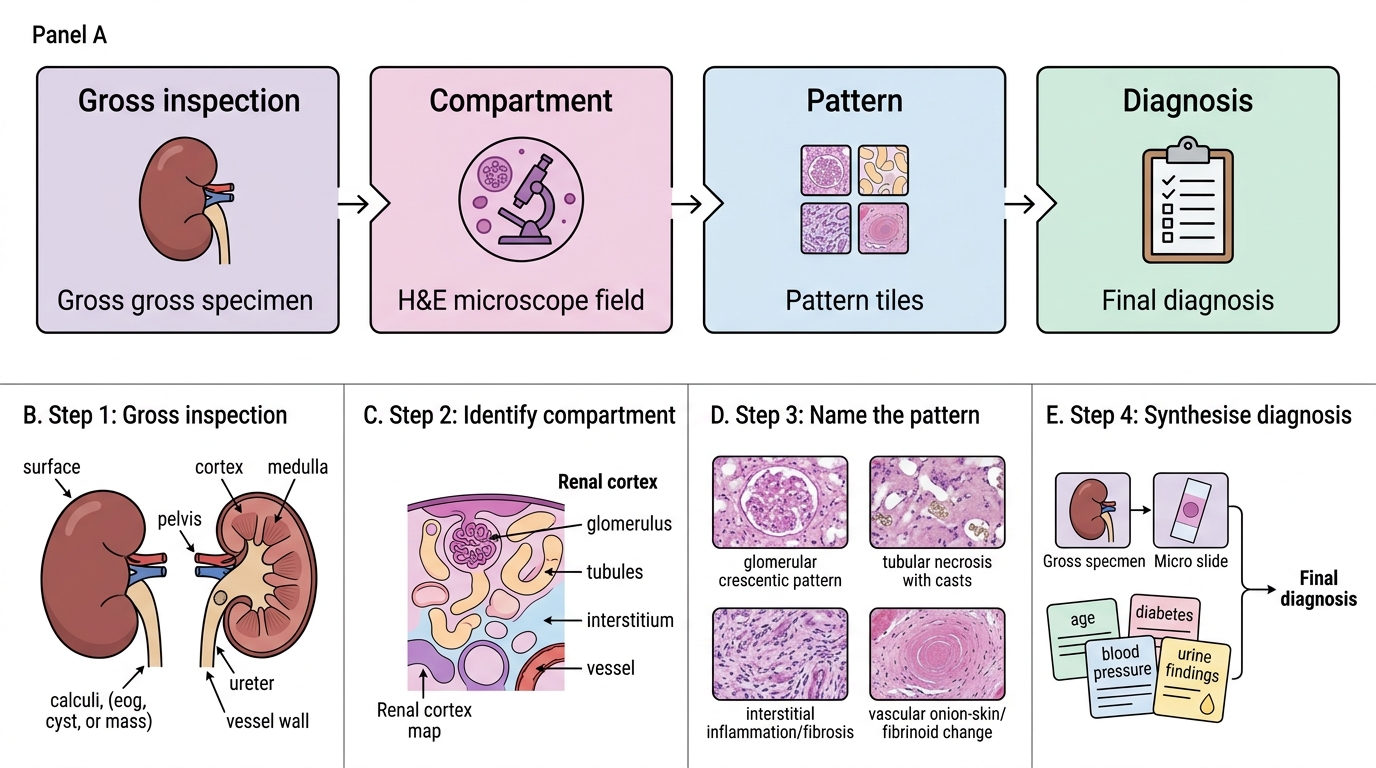
Renal Specimen Reading Framework
Apply this four-step ladder to every renal specimen:
Step 1 — Gross inspection
• Size: normal (10-12 cm) vs. enlarged vs. shrunken
• Surface: smooth vs. granular (fine = vascular/glomerular scarring; coarse = pyelonephritic scars)
• Cut surface: cortex thickness, medullary pattern, cysts, masses, calculi
• Pelvis/ureter: dilated? pus? stones?
• Vessels: wall thickening, calcification
Step 2 — Identify the compartment
On H&E, ask: is the lesion predominantly in the glomeruli, tubules, interstitium, or vessels?
Step 3 — Name the pattern
Within the compartment, use specific descriptors:
• Glomerular: proliferative / membranous / sclerotic / crescentic
• Tubular: necrotic / casts / dilated
• Interstitial: inflammatory infiltrate / fibrosis / abscesses
• Vascular: hyaline / onion-skin / fibrinoid
Step 4 — Synthesise the diagnosis
Combine gross + micro + clinical context (age, diabetes, BP, urine findings) to name the entity.
The sections below apply this framework to each lesion category. Use the IMAGE_NEEDED composite panel (below) as your orientation slide.
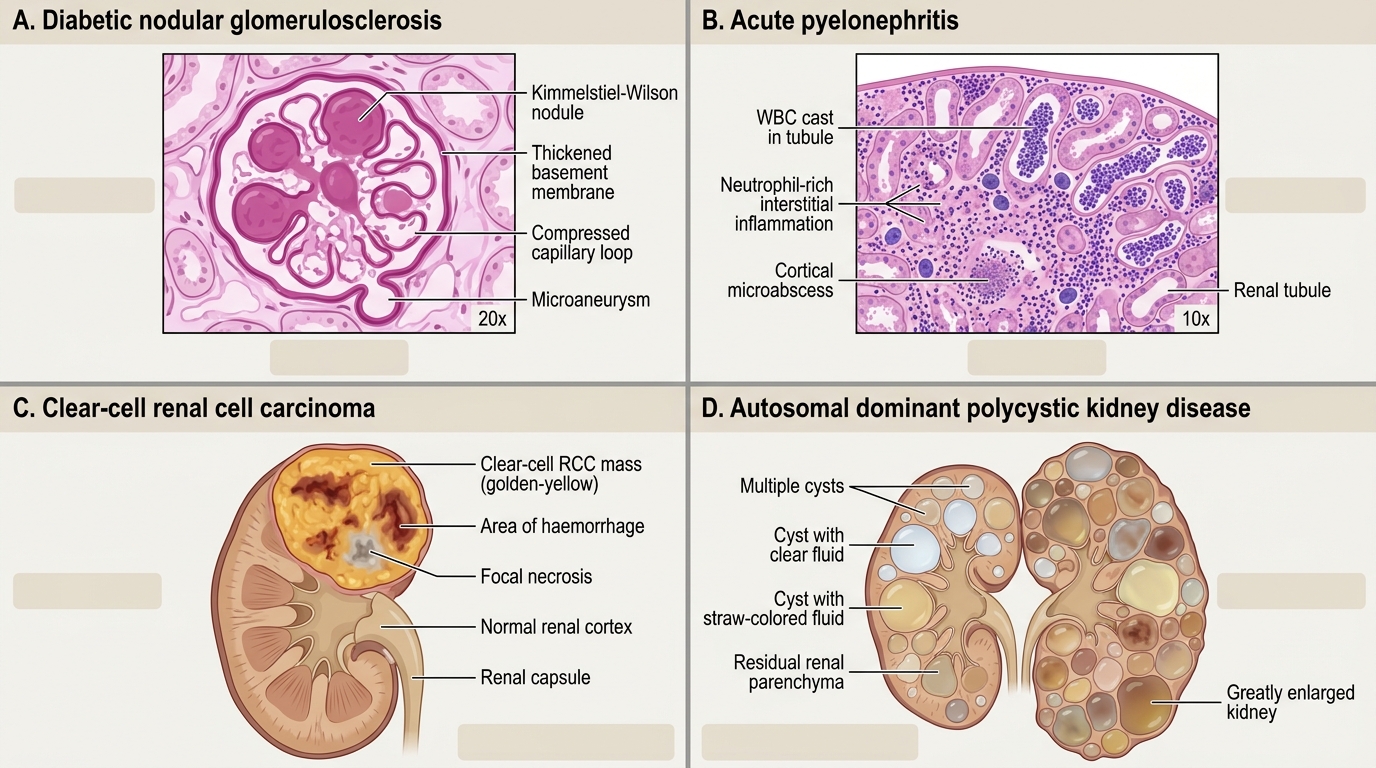
Orientation: Four Renal Specimens Side by Side
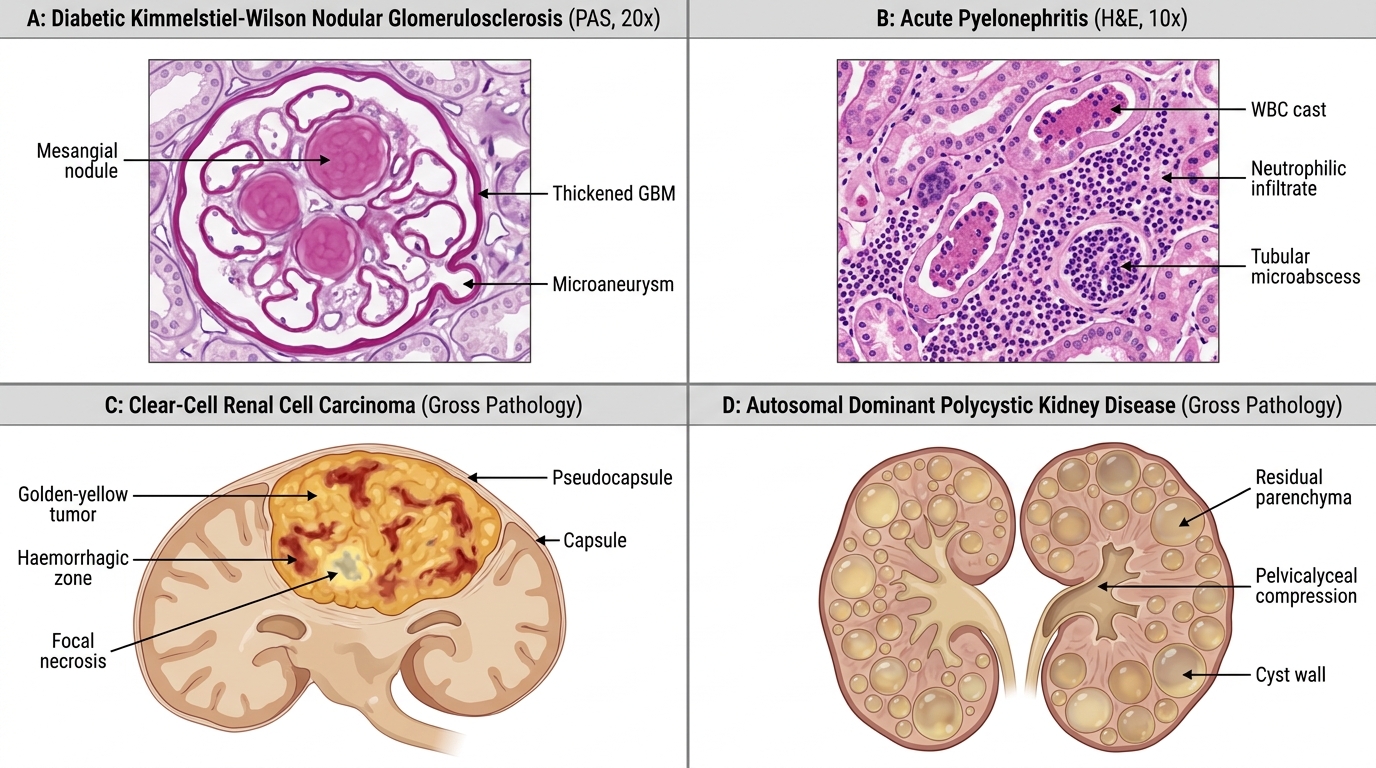
Four Key Renal Pathology Specimens
The composite panel below shows four key specimens — one from each major category. Study the labels before reading the detailed sections.
Renal Pathology: Microscopic and Gross Diagnostic Patterns
Hotspot guide for faculty:
• Panel A: mark mesangial nodule, thickened GBM, microaneurysm
• Panel B: mark WBC cast, tubular microabscess, neutrophilic infiltrate
• Panel C: mark capsule, golden-yellow parenchyma, haemorrhagic zone
• Panel D: mark cyst wall, residual parenchyma, pelycalyceal compression
Glomerular Diseases: Diabetic Nephropathy
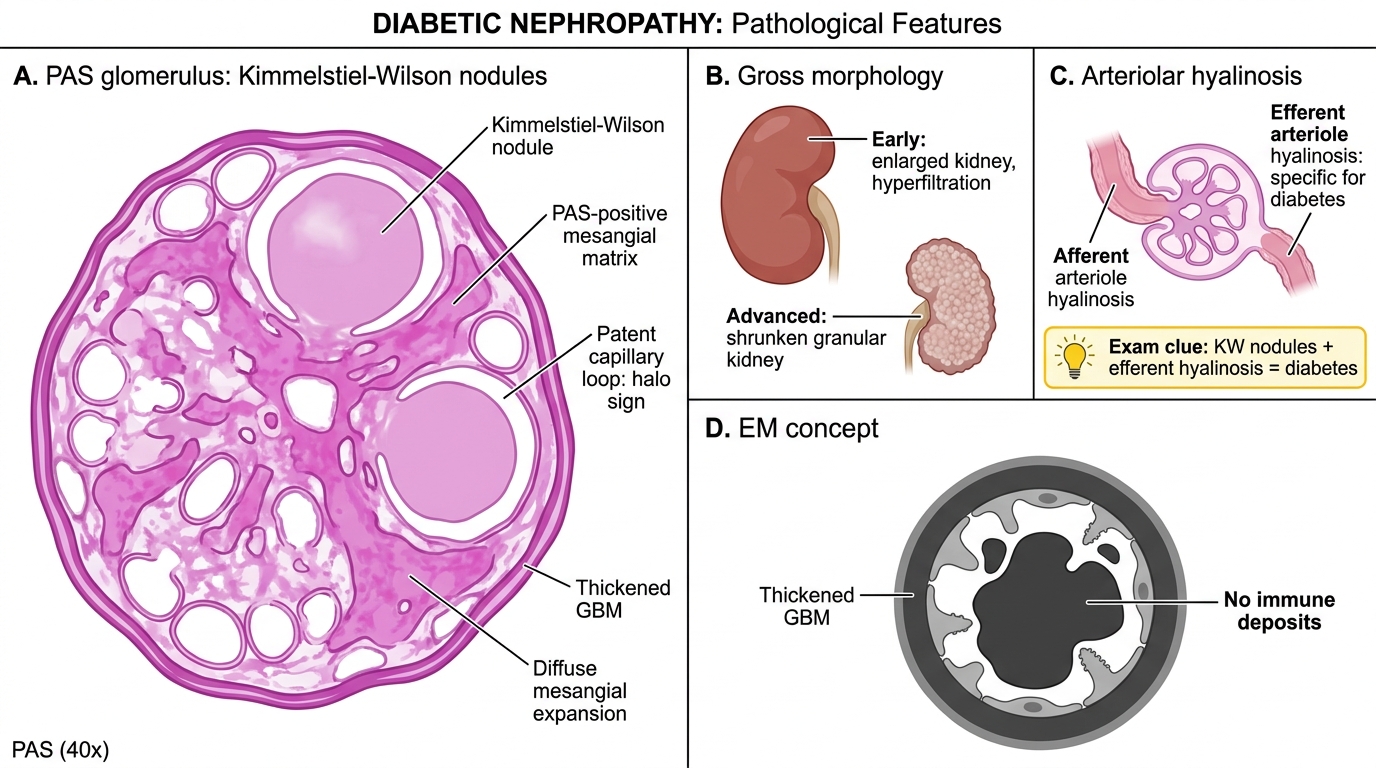
Diabetic Nephropathy: Key Morphologic Features
Diabetic nephropathy is the leading cause of end-stage renal disease worldwide and a favourite examination specimen.
Gross: In early disease the kidneys are large and heavy. In advanced disease they become shrunken with a finely granular surface (indistinguishable grossly from benign nephrosclerosis — micro is the key).
Microscopy (H&E + PAS):
• Diffuse glomerulosclerosis: uniform expansion of the mesangium with PAS-positive material (most common, early)
• Nodular glomerulosclerosis (Kimmelstiel-Wilson nodules): round to oval, acellular, strongly PAS-positive mesangial nodules at the periphery of the glomerulus — pathognomonic of diabetic nephropathy. Nodules are typically surrounded by patent capillary loops (the halo sign).
• Thickening of the GBM throughout
• Hyalinosis of afferent AND efferent arterioles (hyaline arteriolosclerosis of the efferent arteriole is specific to diabetes)
• Armanni-Ebstein change (glycogen vacuolation of tubular cells) — a transient feature in uncontrolled hyperglycaemia
IF/EM concept: EM shows massive GBM thickening and mesangial expansion with electron-dense deposits absent (matrix expansion, not immune deposits).
Exam tip: KW nodules + efferent arteriolar hyalinosis = diabetes. Efferent hyalinosis alone appears in NO other condition.
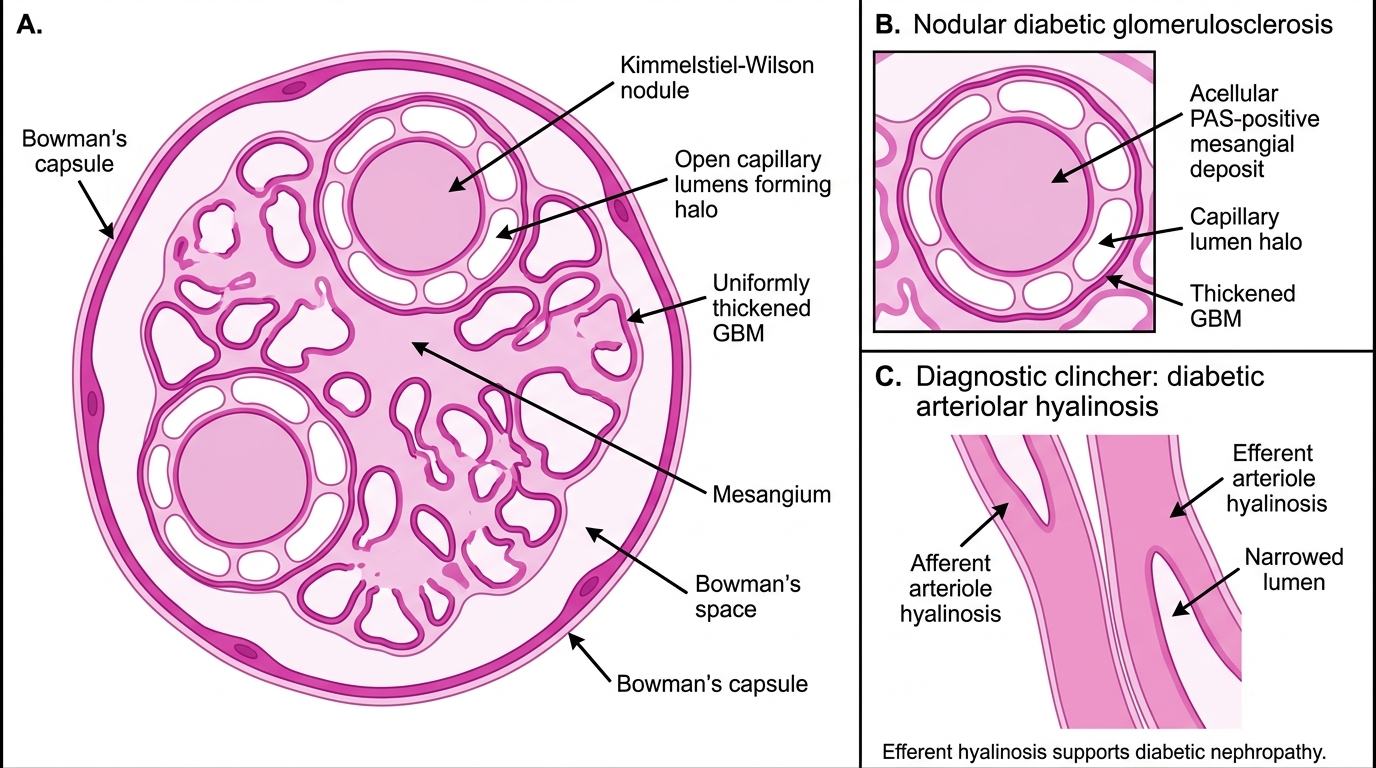
Diabetic Nodular Glomerulosclerosis
SELF-CHECK
A 58-year-old man with 20-year history of type 2 diabetes has proteinuria of 4 g/day. His renal biopsy shows round, PAS-positive, acellular mesangial deposits at the glomerular periphery surrounded by open capillary loops. Which additional histological finding would clinch the diagnosis of diabetic nephropathy over other causes of nodular glomerulosclerosis?
A. Subepithelial 'spike and dome' deposits on silver stain
B. Hyalinosis of both afferent and efferent arterioles
C. Linear IgG deposits on immunofluorescence
D. Diffuse crescentic transformation of glomeruli
Reveal Answer
Answer: B. Hyalinosis of both afferent and efferent arterioles
Hyalinosis of the efferent arteriole is virtually pathognomonic of diabetic nephropathy — no other condition causes efferent hyalinosis. Silver stain spike-and-dome (A) is membranous nephropathy. Linear IgG (C) is Goodpasture/anti-GBM disease. Crescents (D) indicate crescentic GN, a different process.