Page 18 of 27
PA27.17 | Kidney Disease & Tumour Morphology — Practical — SDL Guide (Part 2)
Glomerular Diseases: Crescentic GN, Membranous, and MCD
Key Patterns in Crescentic GN, Membranous Nephropathy, and MCD
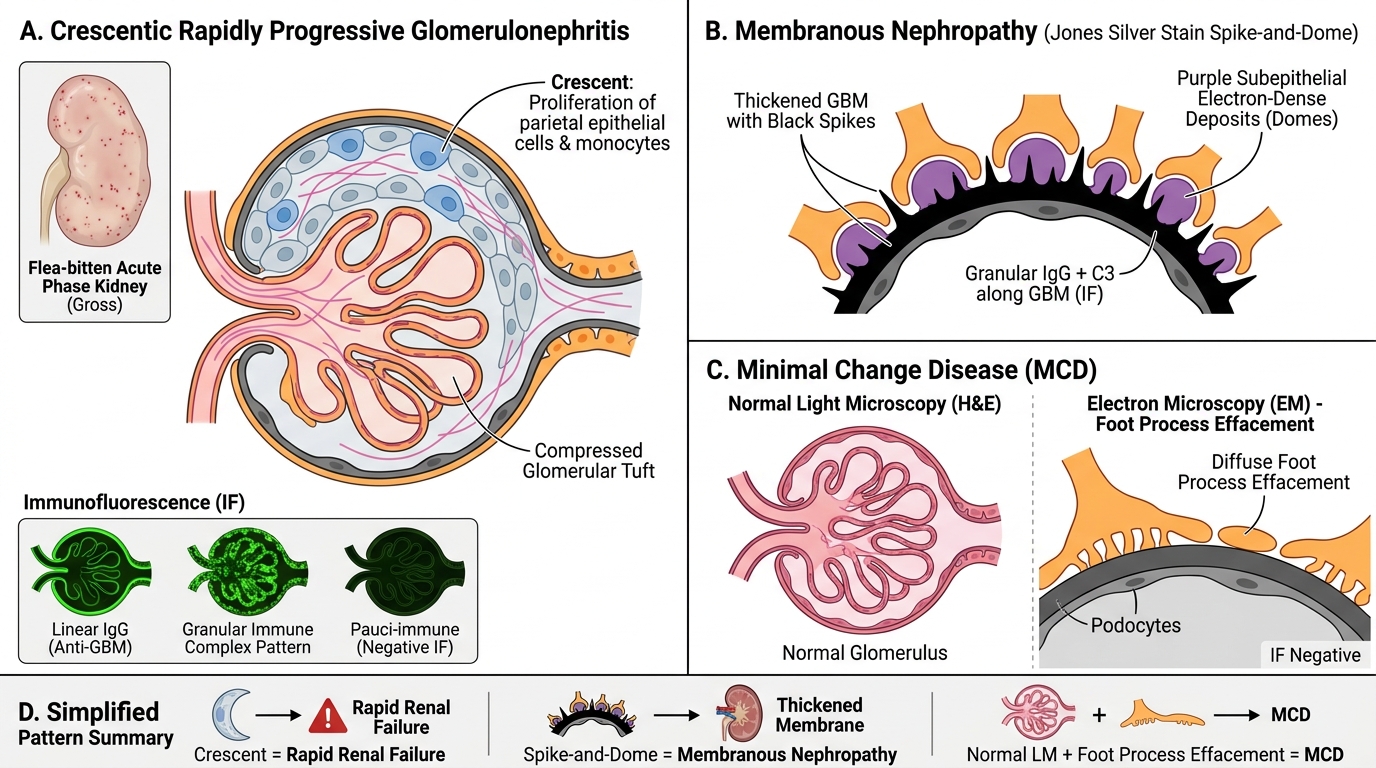
Crescentic (Rapidly Progressive) GN
• Gross: large, pale, flabby kidneys — so pale they are called 'flea-bitten' in the acute phase if petechiae are present
• Micro: the hallmark is a cellular crescent — a proliferation of parietal epithelial cells + monocytes filling Bowman's space, compressing the tuft. Fibrin is present in early crescents (fibrocellular); fibrosis replaces cells in old crescents (fibrous).
• IF: three patterns — linear IgG (anti-GBM/Goodpasture), granular (immune complex GN), pauci-immune (ANCA vasculitis — negative IF)
• Outcome: rapid progression to renal failure if untreated
Membranous Nephropathy
• Pure nephrotic syndrome in adults; most common cause of adult idiopathic nephrotic syndrome
• Micro: glomeruli appear normal on H&E. Silver (Jones methenamine) stain is essential: reveals spike-and-dome pattern — silver-positive GBM spikes projecting between electron-dense subepithelial deposits
• IF: granular IgG + C3 along GBM
• EM: subepithelial electron-dense deposits
Minimal Change Disease (MCD)
• Most common nephrotic syndrome in children; also called lipoid nephrosis
• Light microscopy (H&E): glomeruli appear completely normal — this is the key diagnostic clue
• IF: negative
• EM: diffuse effacement of podocyte foot processes — the only diagnostic abnormality; LM is normal
Pattern summary: Crescent → rapid renal failure / Spike-and-dome (silver) → membranous / Normal LM + foot process effacement (EM) → MCD
SELF-CHECK
A 6-year-old boy presents with periorbital oedema and heavy proteinuria. His renal biopsy on H&E shows completely normal-looking glomeruli. Which investigation will show the diagnostic abnormality?
A. Immunofluorescence — granular IgG along GBM
B. Silver (Jones) stain — spike-and-dome pattern
C. Electron microscopy — diffuse podocyte foot process effacement
D. PAS stain — Kimmelstiel-Wilson mesangial nodules
Reveal Answer
Answer: C. Electron microscopy — diffuse podocyte foot process effacement
Minimal change disease (MCD) has a normal light microscopy picture. The diagnostic finding is on EM: diffuse effacement (fusion) of podocyte foot processes. IF is negative. Silver stain spike-and-dome (B) = membranous nephropathy. KW nodules (D) = diabetic nephropathy.
Tubulointerstitial Disease: Acute Tubular Necrosis
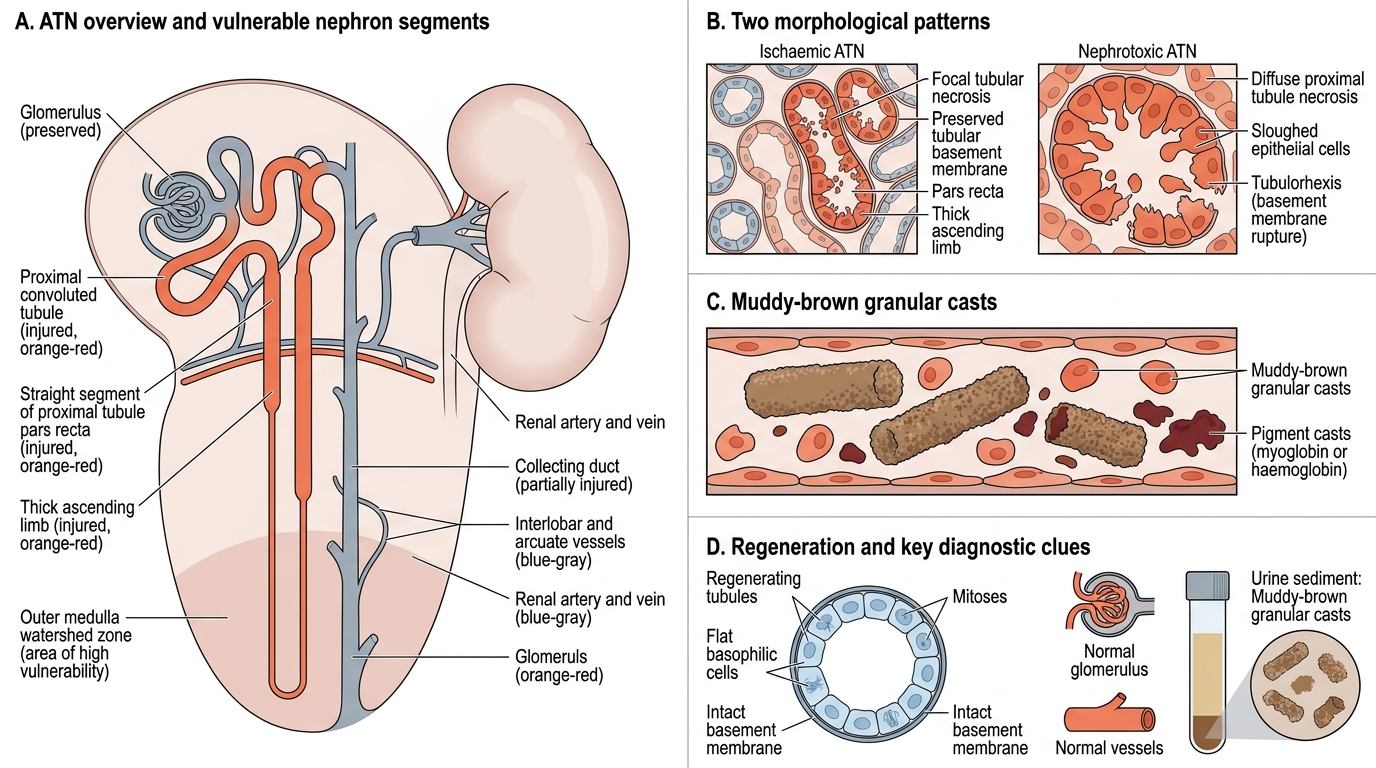
Acute Tubular Necrosis: Morphology and Diagnostic Clues
Acute tubular necrosis (ATN) is the most common cause of acute kidney injury in hospitalised patients.
Two morphological patterns correspond to two aetiologies:
1. Ischaemic ATN (shock, hypotension, sepsis)
• Gross: kidneys pale, swollen, cortex widened
• Micro: focal necrosis of tubular epithelium with preserved basement membrane (tubular BM intact = potential for regeneration). Necrosis predominates at the straight segment of the proximal tubule (pars recta) and the thick ascending limb in the outer medulla (watershed zone)
• Regenerating tubules show flat, basophilic cells with mitoses
2. Nephrotoxic ATN (aminoglycosides, heavy metals, myoglobin/haemoglobin)
• Micro: diffuse necrosis of the entire proximal convoluted tubule (most active reabsorbers, most drug-concentrated)
• Muddy-brown granular casts in tubular lumens (myoglobin/haemoglobin pigment) — pathognomonic of myoglobinuric/haemoglobinuric ATN
• Basement membrane may be disrupted (tubulorhexis) in severe nephrotoxic ATN
Key shared feature: the glomeruli and vessels are NORMAL — distinguishing ATN from glomerulonephritis.
Urine sediment correlation: granular casts (muddy brown) are the urinalysis correlate of ATN on biopsy.
Tubulointerstitial Disease: Acute and Chronic Pyelonephritis
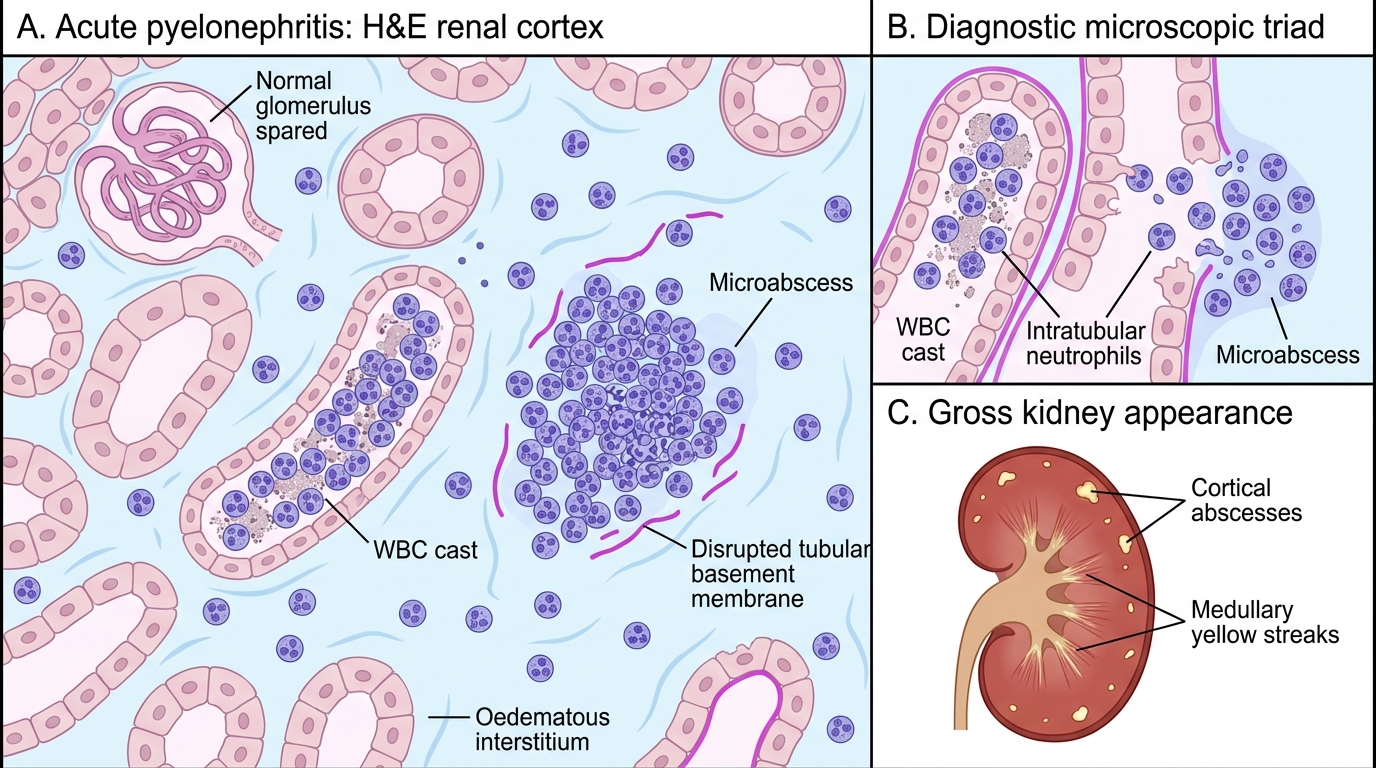
Acute Pyelonephritis: WBC Casts and Microabscesses
Acute Pyelonephritis (APN)
Gross:
• Kidneys enlarged, congested
• Cortical surface shows small yellow-white cortical abscesses (suppurative foci)
• Cut surface: linear yellowish streaks in medulla extending to the cortex
Micro (the diagnostic triad):
1. Intratubular neutrophilic infiltrate (tubular lumens stuffed with PMNs)
2. WBC casts (casts composed of neutrophils) — pathognomonic on urine microscopy AND on biopsy sections of tubular lumens
3. Microabscesses — clusters of neutrophils destroying tubular BM, creating sharply demarcated foci of suppurative necrosis
• Interstitium is oedematous and neutrophil-infiltrated
• Glomeruli typically SPARED (unlike GN)
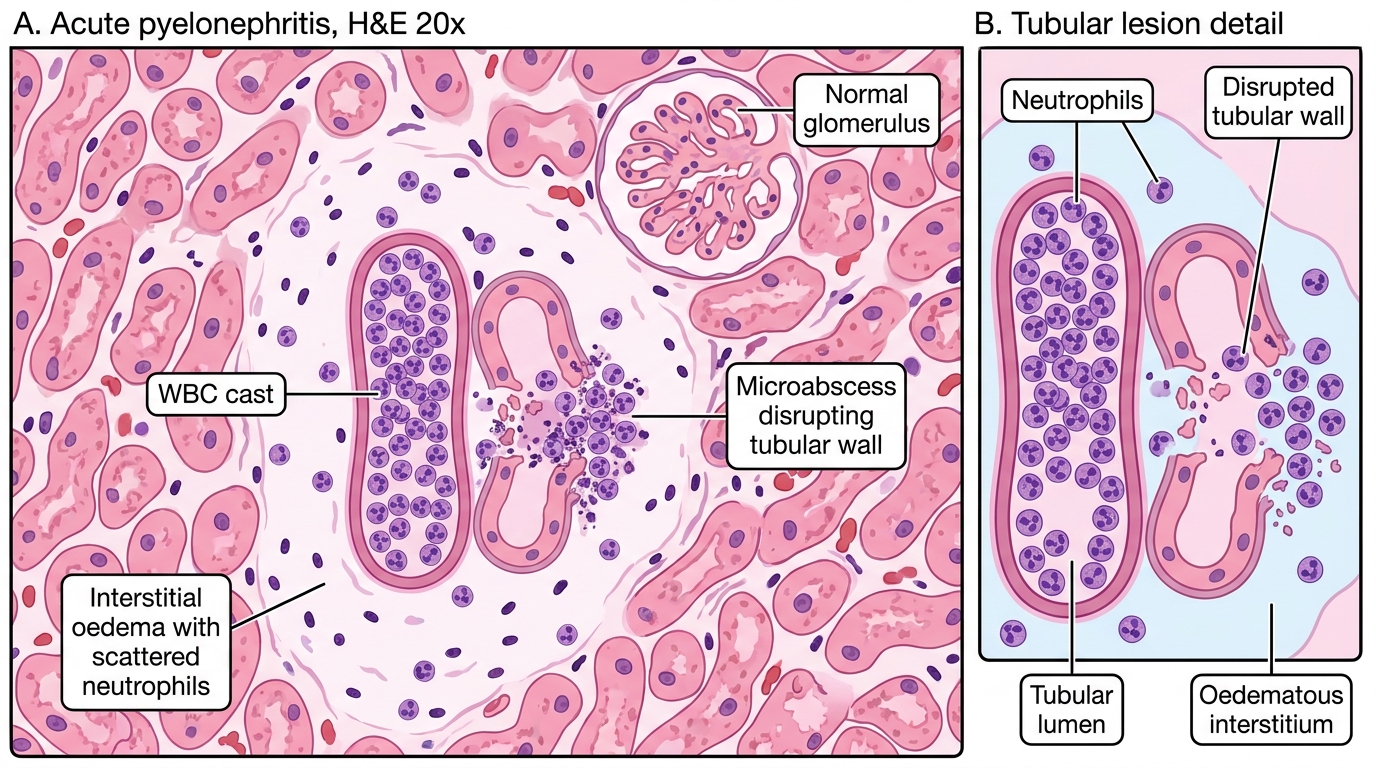
Acute Pyelonephritis: WBC Cast and Microabscess
Chronic Pyelonephritis (CPN)
Gross (distinctive and examinable):
• Coarse, irregular scars that overlie a dilated, blunted calyx — the calyceal blunting + cortical scar combination is unique to CPN (not seen in other scarring diseases)
• The cortex between scars can appear almost normal or slightly thinned
• The kidney is asymmetrically scarred, shrunken, and distorted
Micro:
• Thyroidisation of tubules: dilated tubules packed with homogeneous, eosinophilic, colloid-like casts — resembles thyroid follicles; a distinctive and frequently asked feature
• Periglomerular fibrosis (concentric collagen rings around glomeruli) — distinguishes CPN from glomerulonephritis-related scarring
• Chronic inflammatory infiltrate (lymphocytes, plasma cells) in interstitium
• Fibrosis and tubular atrophy
• Arterial wall thickening in advanced disease
SELF-CHECK
A museum specimen shows a kidney with coarse, irregular scars overlying blunted, dilated calyces. Microscopy reveals dilated tubules packed with homogeneous eosinophilic casts resembling thyroid follicles, and concentric periglomerular fibrosis. What is the diagnosis?
A. Benign nephrosclerosis
B. Chronic pyelonephritis
C. Focal segmental glomerulosclerosis
D. Membranoproliferative GN
Reveal Answer
Answer: B. Chronic pyelonephritis
The combination of coarse scars + calyceal blunting (gross) + thyroidisation of tubules + periglomerular fibrosis (micro) is pathognomonic of chronic pyelonephritis. Benign nephrosclerosis (A) causes fine granular scarring without calyceal change. FSGS (C) and MPGN (D) are primarily glomerular diseases without the tubular or calyceal pattern.