Page 19 of 27
PA27.17 | Kidney Disease & Tumour Morphology — Practical — SDL Guide (Part 3)
Vascular Disease: Benign and Malignant Nephrosclerosis
Benign vs Malignant Nephrosclerosis
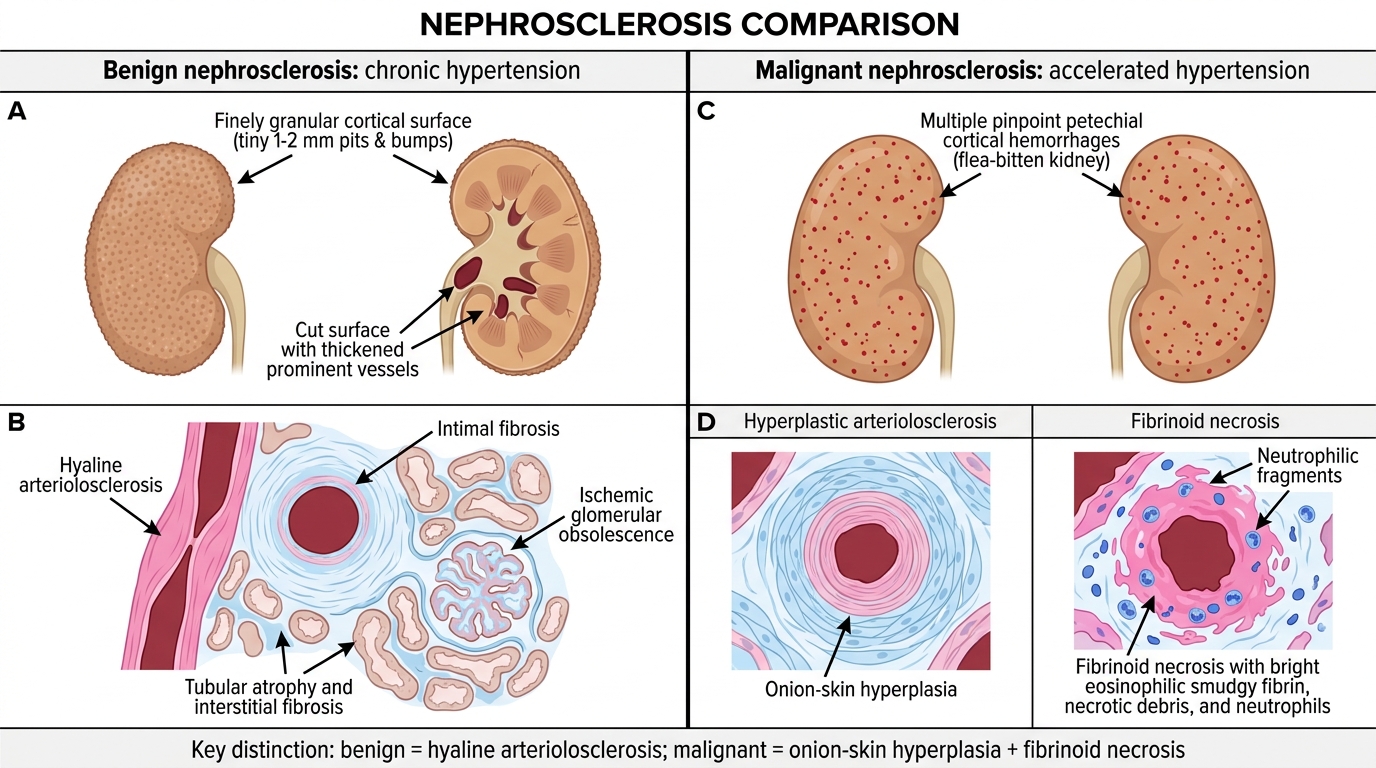
Benign Nephrosclerosis (Hypertensive nephrosclerosis, chronic)
Gross:
• Both kidneys symmetrically reduced in size
• Surface is finely granular — tiny (1-2 mm) pits and bumps corresponding to ischaemic nephron loss alternating with hypertrophied surviving nephrons
• Vessels on cut surface appear thickened and prominent
Micro:
• Hyaline arteriolosclerosis: homogeneous, eosinophilic (pink) material replacing the vessel wall of small arteries and arterioles — the morphological signature of chronic hypertension
• Intimal fibrosis of interlobular arteries (concentric, cellular proliferation)
• Downstream: ischaemic glomerular changes — wrinkling/retraction of capillary tuft, periglomerular fibrosis, eventual obsolescence (ischaemic obsolescence)
• Tubular atrophy + interstitial fibrosis in areas of nephron loss
Malignant Nephrosclerosis (Accelerated/malignant hypertension)
Gross: kidneys may be normal or enlarged; petechial haemorrhages on cortical surface ("flea-bitten" kidney)
Micro — two key patterns:
• Hyperplastic arteriolosclerosis (onion-skin lesion): concentric layers of proliferating smooth muscle cells and collagen in the arteriolar wall, giving an onion-skin appearance — this is the hallmark of malignant hypertension
• Fibrinoid necrosis of arterioles: eosinophilic smudgy material (fibrin + necrotic debris) replacing the vessel wall, often with neutrophilic infiltration
Key distinction: benign → hyaline (homogeneous) / malignant → onion-skin + fibrinoid (cellular, with necrosis)
SELF-CHECK
A 35-year-old woman presents with sudden BP of 230/140 mmHg, acute kidney injury, and retinal haemorrhages. Her renal biopsy arterioles show concentric layers of proliferating smooth muscle cells and collagen within the vessel wall, and one arteriole shows replacement of the wall by smudgy eosinophilic material. What are these two findings respectively?
A. Hyaline arteriolosclerosis and fibrinoid necrosis
B. Onion-skin hyperplastic arteriolosclerosis and fibrinoid necrosis
C. Amyloid angiopathy and thrombotic microangiopathy
D. Hyaline arteriolosclerosis and onion-skin arteriolosclerosis
Reveal Answer
Answer: B. Onion-skin hyperplastic arteriolosclerosis and fibrinoid necrosis
Malignant hypertension produces two arteriolar lesions: (1) onion-skin hyperplastic arteriolosclerosis — concentric smooth muscle + collagen lamellae; and (2) fibrinoid necrosis — smudgy eosinophilic fibrin replaces/destroys the wall. Hyaline arteriolosclerosis (A/D) is the benign form. Amyloid (C) would show Congo red positivity.
Gross Kidneys at a Glance: End-Stage, PKD, Hydronephrosis, RCC
Gross Kidney Patterns at a Glance
Four gross patterns you must instantly recognise:
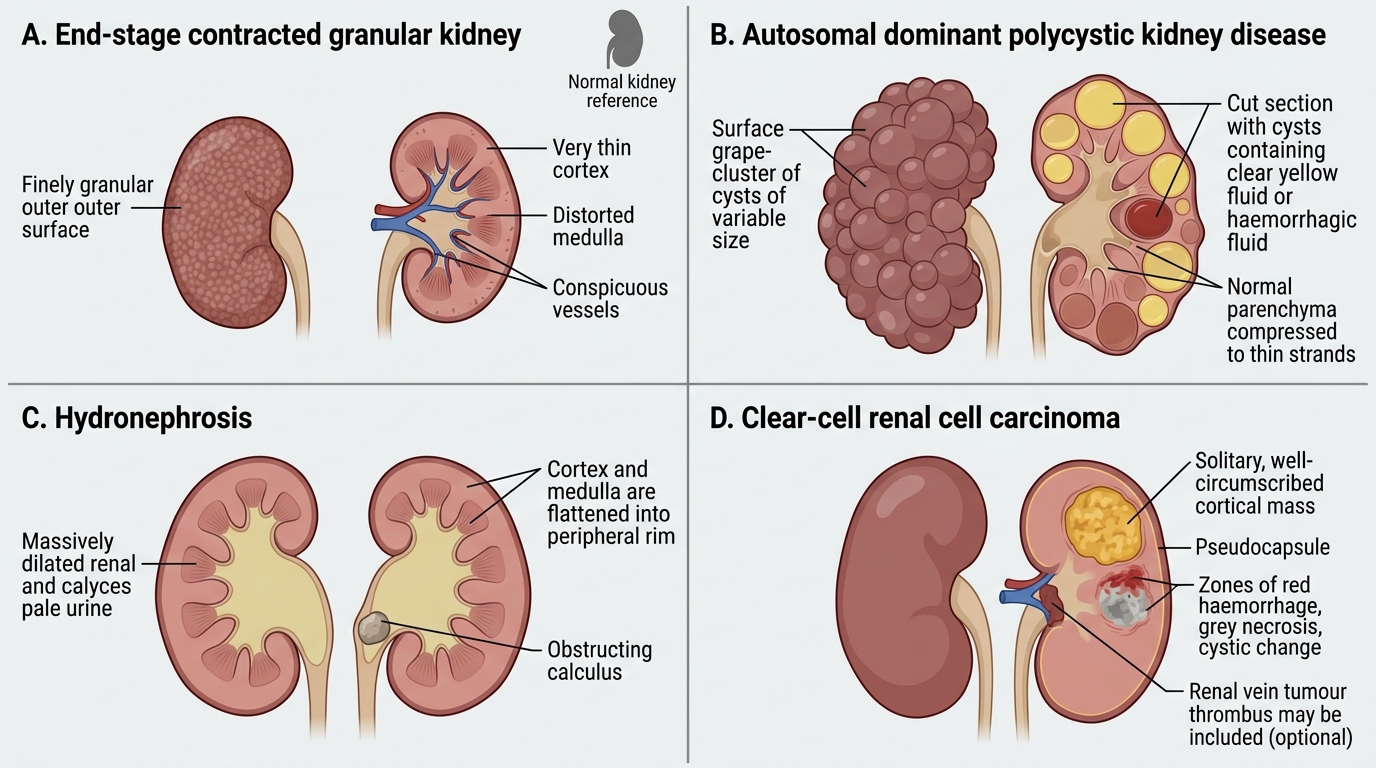
End-Stage (contracted granular) Kidney
• Small (often < 100 g), finely granular surface
• Cortex severely thinned, medulla distorted
• Vessels prominent on cut surface
• Arises from: benign nephrosclerosis, diabetic nephropathy, chronic GN (any)
• The gross cannot tell you the aetiology — micro (or history) does
Autosomal Dominant Polycystic Kidney Disease (ADPKD)
• Dramatically enlarged kidneys (can reach 40 cm, 4 kg each)
• Replaced by multiple bilateral cysts of varying sizes (grape-cluster appearance)
• Normal parenchyma is compressed and almost absent
• Cyst fluid: clear, yellow, or haemorrhagic
• Associated: berry aneurysms, hepatic cysts, mitral valve prolapse
Hydronephrosis
• Kidney enlarged; cut surface reveals massively dilated pelvis and calyces filled with urine
• Parenchyma is compressed to a thin rim — cortex + medulla flattened
• Cause: any obstruction (calculus, BPH, tumour, stricture) must be sought at the ureter/pelvis junction
Clear-Cell Renal Cell Carcinoma (RCC)
• Solitary cortical mass, well circumscribed, may have a pseudocapsule
• Cut surface: golden yellow (lipid + glycogen in tumour cells) with zones of haemorrhage and necrosis
• Cystic areas common
• Occasionally invades renal vein as a tumour thrombus
Renal Tumours: RCC, Wilms, and Urothelial Carcinoma
Renal Tumours: RCC, Wilms Tumour, and Urothelial Carcinoma
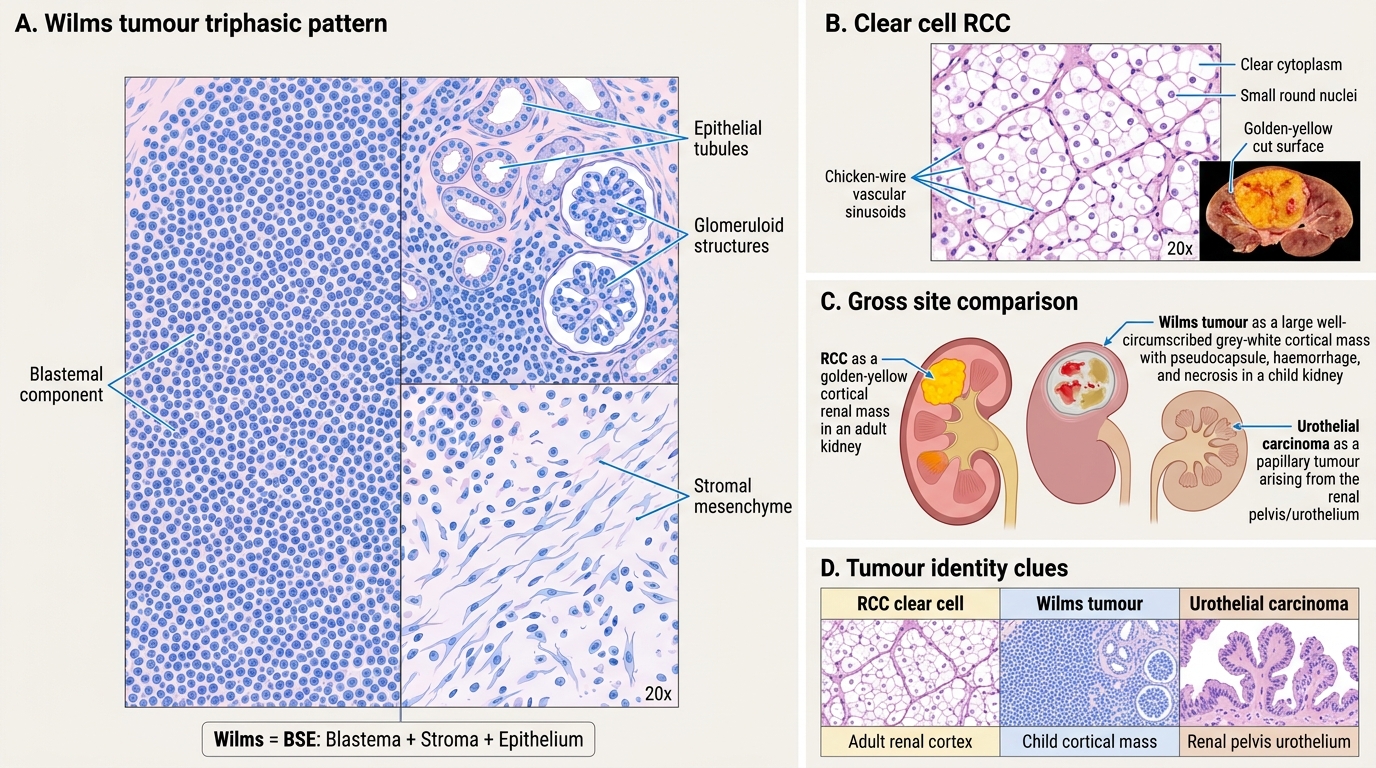
Renal Cell Carcinoma (RCC) — Clear Cell Type
Micro:
• Sheets and nests of cells with abundant clear cytoplasm (dissolved lipid + glycogen on routine processing) and small, round nuclei
• Delicate thin-walled vascular sinusoids between nests (chicken-wire vascular pattern)
• Fuhrman nuclear grade reflects prognosis (Grade 1 = small uniform nuclei; Grade 4 = pleomorphic, prominent nucleoli)
Gross correlate: golden-yellow on cut surface = cleared cytoplasm
Wilms Tumour (Nephroblastoma)
Gross: large, well-circumscribed cortical mass in a child; soft grey-white with haemorrhage/necrosis; pseudocapsule present
Micro: the classic triphasic pattern:
1. Blastemal component: sheets of small, round, primitive blue cells (high N:C ratio, hyperchromatic — looks like small blue cell tumour)
2. Stromal component: loose, undifferentiated mesenchyme, may show heterologous differentiation (skeletal muscle, cartilage)
3. Epithelial component: primitive tubules and glomeruloid structures (abortive attempt at nephrogenesis)
Mnemonic: Wilms = Blue Stroma Epithelium (BSE — all three components)
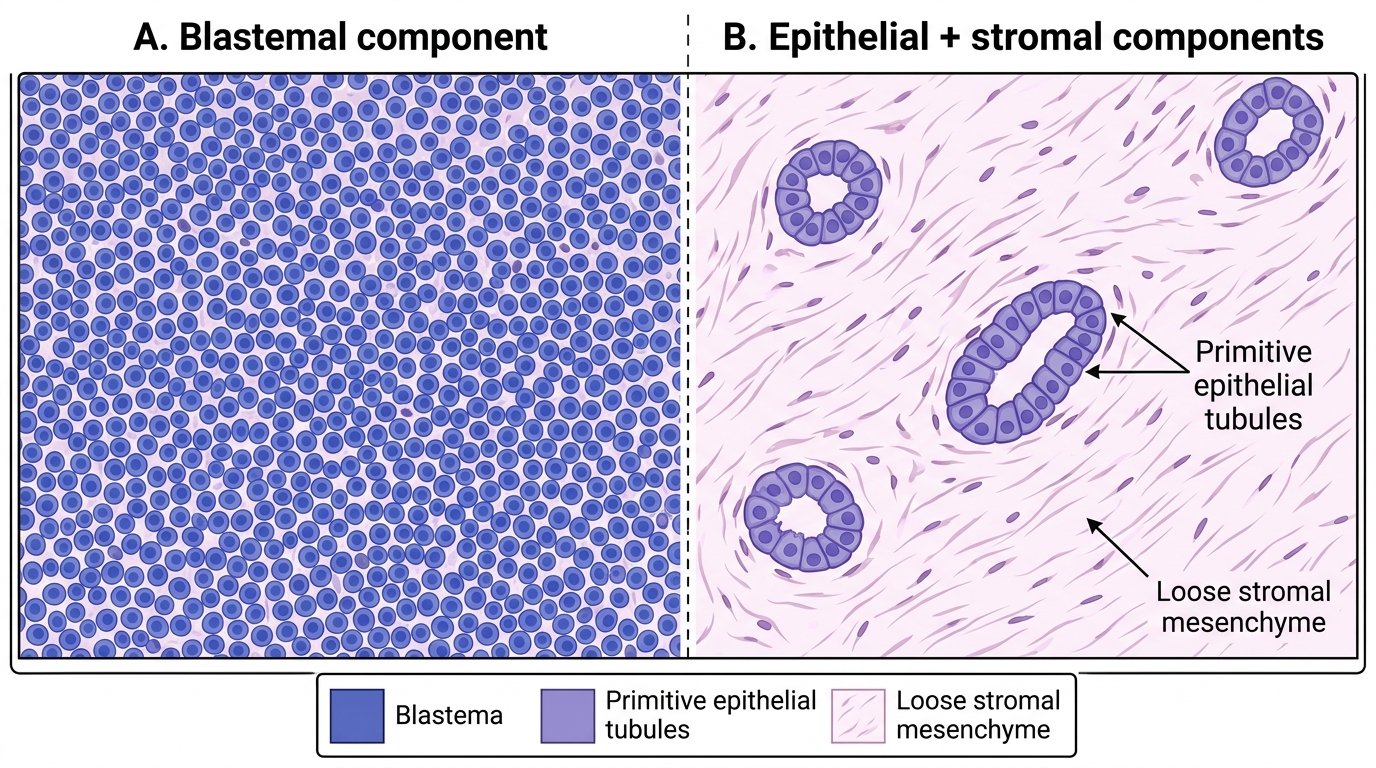
Wilms Tumour Triphasic Pattern on H&E
Urothelial (Transitional Cell) Carcinoma
Site: renal pelvis (urothelium-lined), not renal parenchyma
Gross: papillary, frond-like mass projecting into the pelvic lumen; may obstruct and cause hydronephrosis
Micro: multilayered transitional epithelium on fibrovascular cores (papillary architecture); cytological atypia graded low vs. high grade; invasion of lamina propria = invasive carcinoma
Key distinction from RCC: location (pelvis not cortex), papillary not solid sheets, transitional not clear-cell cytology
SELF-CHECK
A 4-year-old child is found to have a large abdominal mass. Biopsy shows three components: (1) sheets of small, round, hyperchromatic blue cells with scant cytoplasm; (2) loose spindle-cell stroma with heterologous muscle differentiation; (3) primitive tubular and glomeruloid structures. Which is the most likely diagnosis?
A. Clear-cell renal cell carcinoma
B. Neuroblastoma
C. Wilms tumour (Nephroblastoma)
D. Ewing sarcoma
Reveal Answer
Answer: C. Wilms tumour (Nephroblastoma)
The triphasic pattern — blastemal (small round blue cells) + stromal + epithelial (tubular/glomeruloid) components — is pathognomonic of Wilms tumour (nephroblastoma). Clear-cell RCC (A) occurs in adults and shows clear cytoplasm without triphasic pattern. Neuroblastoma (B) lacks epithelial/stromal components and arises from adrenal/retroperitoneum. Ewing sarcoma (D) is monophasic (all blastemal) and shows CD99 positivity.