Page 20 of 27
PA27.17 | Kidney Disease & Tumour Morphology — Practical — SDL Guide (Part 4)
Integrative Pattern Recognition: Putting It All Together
Renal Pathology Pattern Recognition Matrix
Use this decision matrix at the bench:
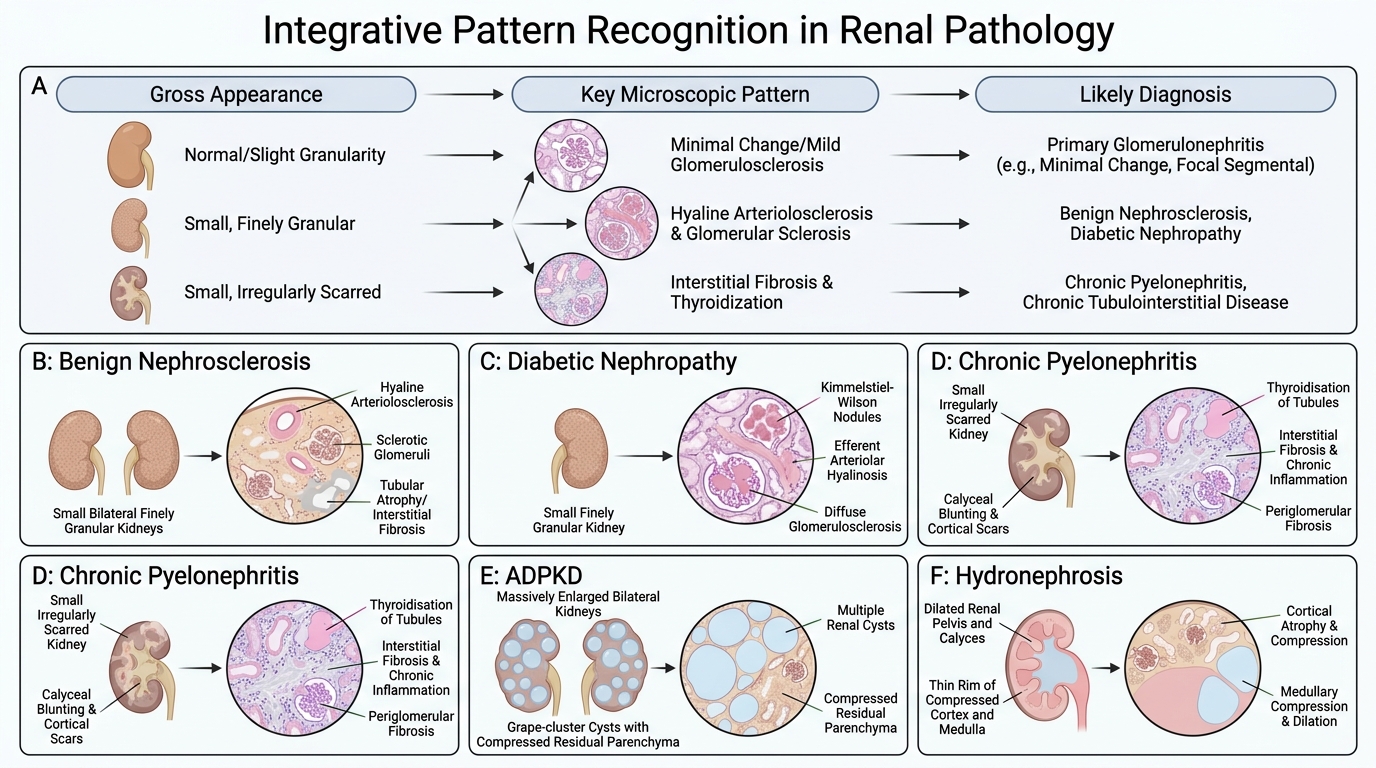
| Gross appearance | Key micro pattern | Diagnosis |
|---|---|---|
| Finely granular, small, bilateral | Hyaline arteriolosclerosis | Benign nephrosclerosis |
| Finely granular, small, bilateral | KW nodules + efferent hyalinosis | Diabetic nephropathy |
| Finely granular, small, bilateral | Thyroidisation + calyceal blunting | Chronic pyelonephritis |
| Massively enlarged, bilateral cysts | Grape-cluster cysts, compressed parenchyma | ADPKD |
| Dilated calyces, thin rim | Thinned cortex + medulla | Hydronephrosis |
| Cortical abscess, yellow streaks | WBC casts + microabscesses | Acute pyelonephritis |
| Pale, swollen, cortex widened | Focal tubular necrosis, muddy-brown casts | ATN |
| Petechial 'flea-bitten' surface | Onion-skin + fibrinoid necrosis | Malignant nephrosclerosis |
| Golden-yellow cortical mass | Clear cells + chicken-wire vessels | Clear-cell RCC |
| Large child's mass, pseudocapsule | Triphasic: blastema + stroma + epithelium | Wilms tumour |
| Papillary pelvic mass | Transitional epithelium, papillary cores | Urothelial carcinoma |
Special stain summary for examiners:
• PAS: best for GBM thickening, KW nodules, mesangial matrix
• Silver (Jones): spike-and-dome of membranous nephropathy
• H&E: all routine tissue patterns
• Congo red: amyloid (apple-green birefringence)
CLINICAL PEARL
The three 'finely granular, small kidney' mimics always trip students in viva:
- Benign nephrosclerosis: hyaline arteriolosclerosis (afferent ± efferent), ischaemic glomerular obsolescence
- Diabetic nephropathy: KW nodules, efferent arteriolar hyalinosis (not seen in any other condition)
- Chronic GN (end-stage): glomeruli show global or segmental sclerosis corresponding to the original GN type; no hyaline arteriolosclerosis unless hypertension co-exists
When the gross alone cannot distinguish them, look for:
• Hyaline in arterioles → nephrosclerosis or diabetes
• KW nodules → diabetes only
• Glomerular residua (mesangial hypercellularity, membranous deposits) → chronic GN
If you can confidently say 'efferent hyalinosis present' → the examiner nods and moves on.