Page 13 of 27
PA27.{14,16} | Renal & Urothelial Tumours — SDL Guide
Learning Objectives
- Classify renal tumours into benign and malignant, with key examples of each
- Describe the epidemiology, risk factors, molecular genetics, and pathological features of renal cell carcinoma (RCC) and its major subtypes
- Explain the classic clinical triad, paraneoplastic syndromes, and spread pattern of RCC
- Outline the pathological features and clinical behaviour of Wilms tumour (nephroblastoma)
- Describe the risk factors, morphology, grading, staging, and clinical features of urothelial (transitional cell) carcinoma of the bladder
INSTRUCTIONS
Tumours of the kidney and urothelium together account for a significant slice of adult and paediatric oncology practice. For a Year-2 student, mastering this topic means being able to differentiate pathological subtypes, correlate molecular drivers with morphology, and recognise the hallmark clinical presentations—skills you will use in clinical postings, OSCEs, and long-case examinations. This module takes you systematically from benign renal lesions through the three RCC subtypes, into the unique childhood tumour Wilms, and finally into the bladder.
References
- Robbins & Kumar Basic Pathology, 11th ed., Ch 13 (Kidney and Its Collecting System) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 25 (Urinary Tract) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old male smoker presents to the casualty with a single episode of painless blood in his urine. Examination reveals a palpable flank mass. His haemoglobin is elevated at 19 g/dL, and calcium is 3.1 mmol/L. A CT scan shows a large upper-pole renal mass with extension into the renal vein and a 'cannonball' shadow in the right lung field.
This one patient captures three of the most testable concepts in renal oncology: the classical triad of renal cell carcinoma, its paraneoplastic syndromes, and its characteristic route of spread. By the end of this module you will be able to explain exactly why each of these findings occurs.
WHY THIS MATTERS
Renal cell carcinoma is the commonest malignant tumour of the kidney in adults, accounting for ~85% of primary renal malignancies. Bladder carcinoma is the second most common urological malignancy worldwide. Together, renal and urothelial tumours are tested repeatedly in theory papers, OSCE stations, and clinical long cases. The molecular genetics of RCC (VHL gene, chromosome 3p) represents a model example of the two-hit tumour suppressor hypothesis you studied in General Pathology.
RECALL
Before you proceed, quickly recall:
- What is the two-hit hypothesis for tumour suppressor genes? (You studied this with retinoblastoma in General Pathology.)
- What is the embryological origin of the kidney? Which cell layer gives rise to the renal tubular epithelium?
- What does the term transitional epithelium (urothelium) mean, and where does it line?
- What is the classical histological description of clear cell change — what does lipid-laden cytoplasm look like under the microscope?
Benign Renal Tumours — Overview
Benign Renal Tumours: Key Differentiating Features
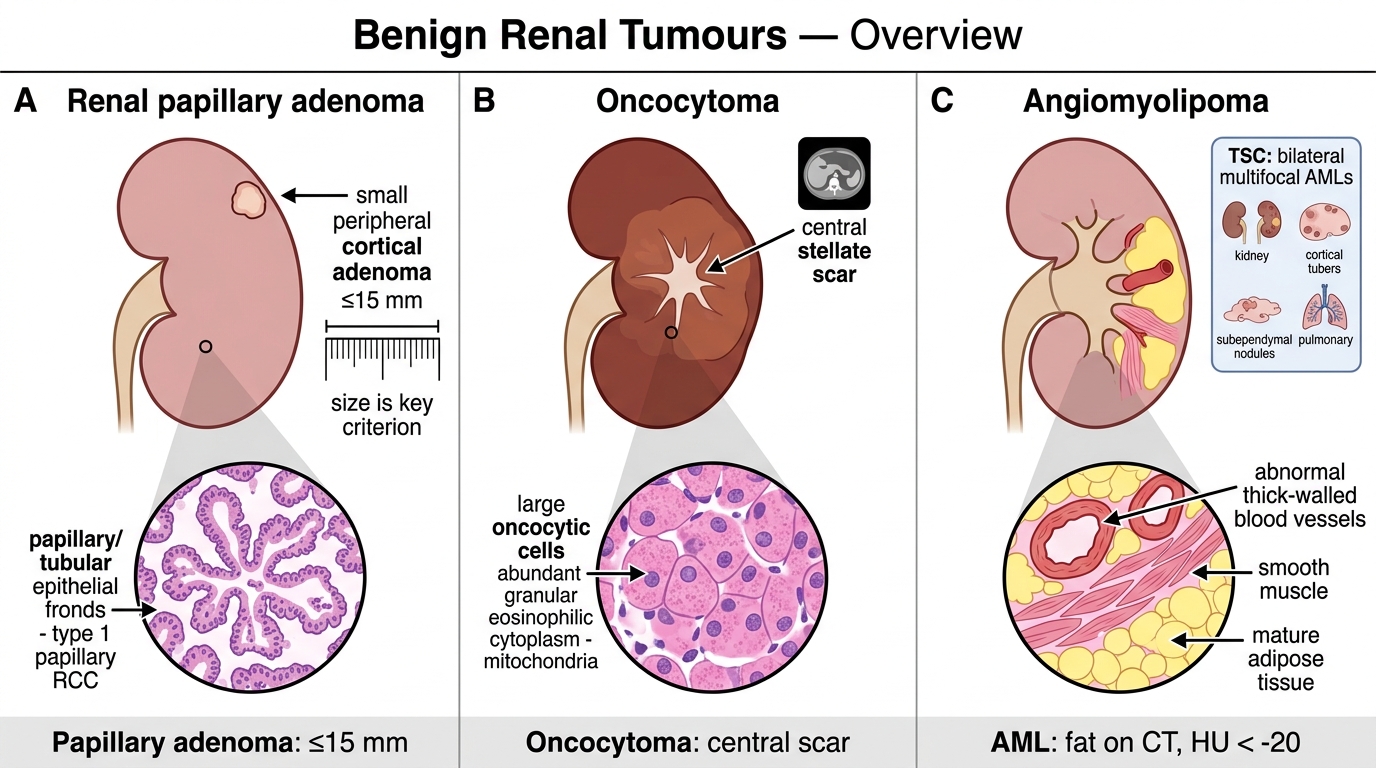
Although most clinically significant renal tumours are malignant, three benign entities deserve mention because they enter the differential of a renal mass on imaging.
Renal papillary adenoma is the commonest benign epithelial lesion, found incidentally at autopsy. It is defined by size (≤15 mm) and papillary or tubular architecture; lesions larger than this are considered potentially malignant. Histologically it resembles papillary RCC (type 1), making size the key distinguishing criterion.
Oncocytoma accounts for ~5% of renal epithelial neoplasms. It arises from intercalated cells of the collecting duct. Gross appearance is characteristic: a large, mahogany-brown tumour with a central stellate scar. Histologically the tumour is composed of large cells with abundant, finely granular eosinophilic cytoplasm packed with mitochondria. On CT the central scar is a useful imaging feature, but tissue diagnosis is required for certainty.
Angiomyolipoma (AML) is a hamartomatous lesion composed of three elements: abnormal thick-walled blood vessels, smooth muscle, and mature adipose tissue — hence the name. Solitary AMLs occur sporadically. However, ~80% of patients with tuberous sclerosis complex (TSC) develop bilateral, multifocal AMLs; TSC is also associated with cortical tubers, subependymal nodules, and pulmonary lymphangioleiomyomatosis. The fat component is visible on CT (Hounsfield units <−20), allowing confident non-invasive diagnosis.
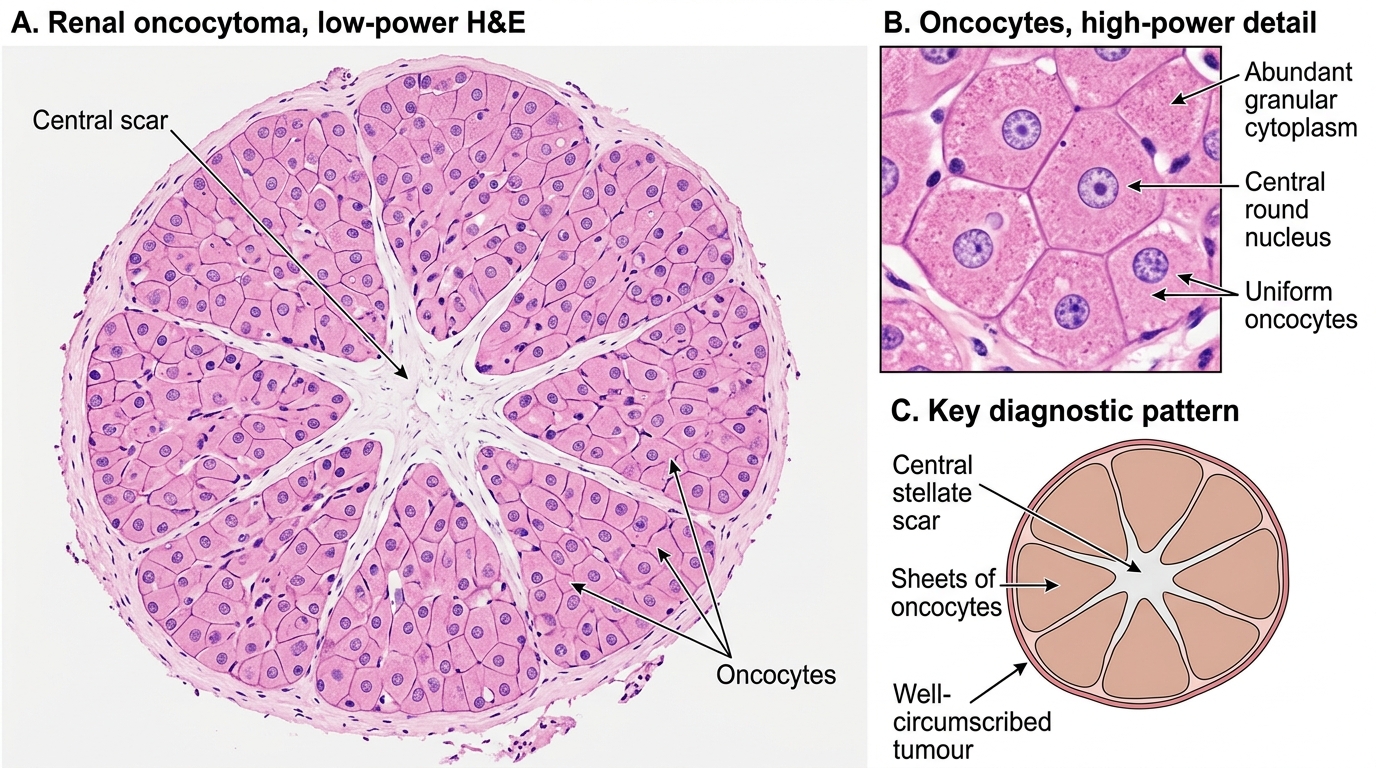
Renal Oncocytoma: Microscopic Features
Renal Cell Carcinoma — Epidemiology and Risk Factors
Renal Cell Carcinoma: Epidemiology and Risk Factors
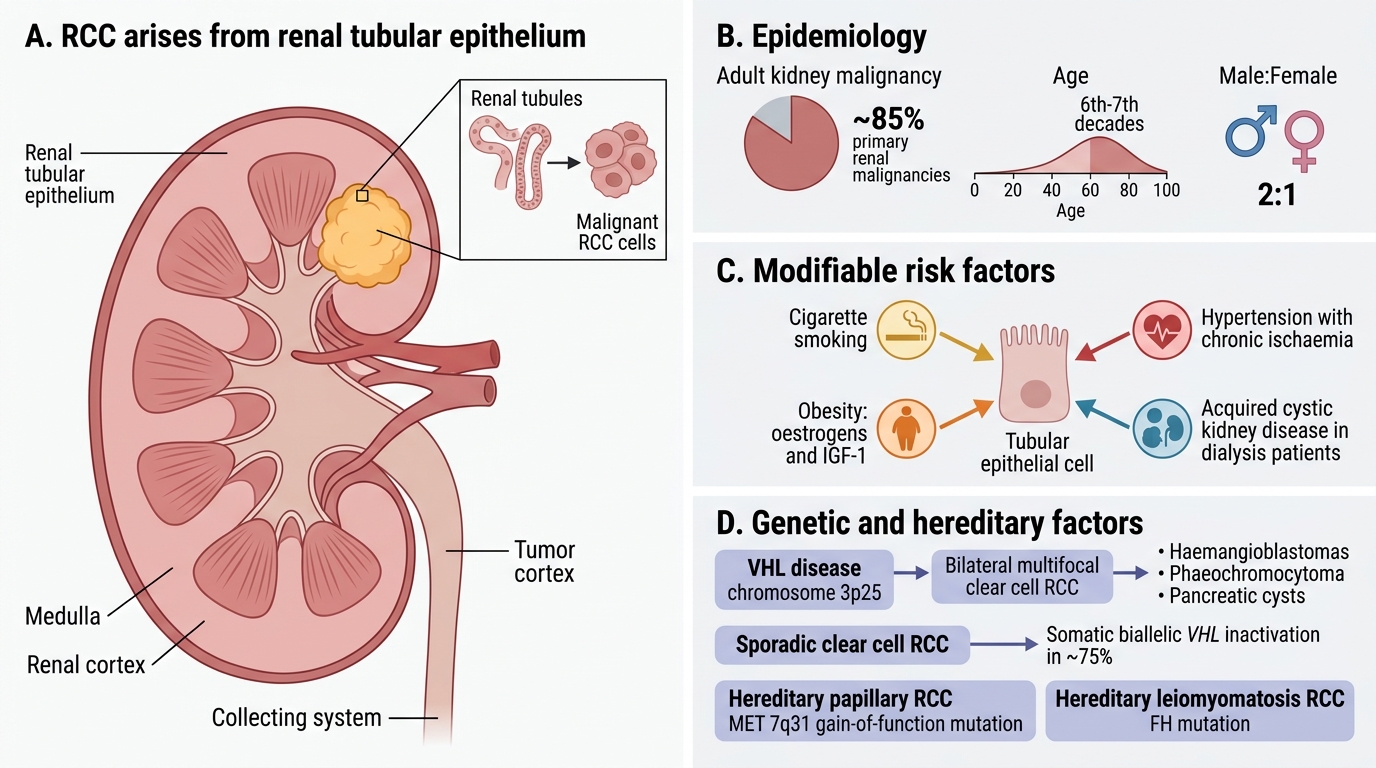
Renal cell carcinoma (RCC) arises from the renal tubular epithelium. It accounts for ~85% of primary renal malignancies in adults, with a peak incidence in the 6th–7th decades and a male:female ratio of approximately 2:1.
Modifiable risk factors:
• Cigarette smoking — strongest environmental risk factor; doubles the risk; dose-dependent
• Obesity — adipose tissue produces oestrogens and IGF-1, promoting tubular cell proliferation
• Hypertension — independent risk, possibly mediated by chronic ischaemia
• Acquired cystic kidney disease in dialysis patients — markedly elevated risk
Genetic/hereditary factors:
• Von Hippel–Lindau (VHL) disease — autosomal dominant; germline VHL mutation on chromosome 3p25; bilateral, multifocal clear cell RCC, haemangioblastomas (cerebellum, retina), phaeochromocytoma, pancreatic cysts
• Sporadic clear cell RCC: somatic biallelic VHL inactivation in ~75% of cases
• Hereditary papillary RCC: germline MET (7q31) gain-of-function mutations
• Hereditary leiomyomatosis RCC: germline FH (fumarate hydratase) mutations
RCC Subtypes — Molecular Genetics and Histology
Renal Cell Carcinoma Subtypes: Genetics and Histology
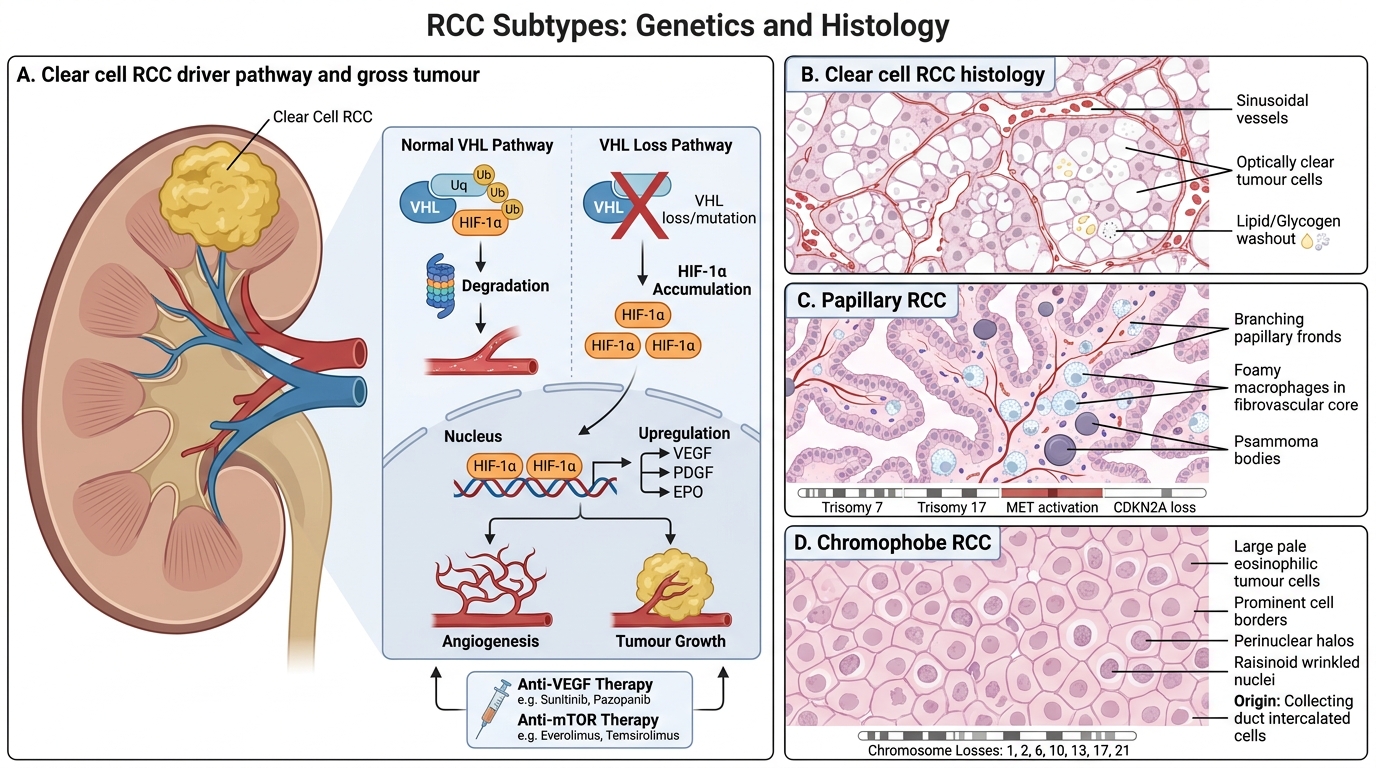
Three major subtypes of RCC are recognised. Each has a distinct genetic driver, morphology, and prognosis.
1. Clear cell RCC (ccRCC) — commonest, ~75%
Genetics: Biallelic loss of the VHL tumour suppressor gene (chromosome 3p25). Normally, the VHL protein targets HIF-1α (hypoxia-inducible factor) for proteasomal degradation. Loss of VHL → HIF-1α accumulates → upregulation of VEGF, PDGF, and EPO → pseudo-hypoxic angiogenesis and tumour growth. This is why RCC responds to anti-VEGF/anti-mTOR targeted therapy.
Morphology: Tumour cells have optically clear cytoplasm due to dissolved lipid and glycogen (washed out in routine H&E processing). Cells are arranged in nests and cords separated by delicate, thin-walled sinusoidal vessels. Nuclei show a spectrum of atypia (WHO/ISUP grading 1–4).
Gross: Bright yellow-golden colour (lipid), often with areas of haemorrhage and necrosis, giving a variegated cut surface. Characteristically arises in the upper pole. A pseudocapsule may be present.
2. Papillary RCC — ~15%
Genetics: Trisomy 7 and 17; MET activation (type 1) or CDKN2A loss (type 2). Not associated with VHL loss.
Morphology: Papillary fronds lined by tumour cells with foamy macrophages in the stalks. Type 1 (low-grade, favourable) vs. type 2 (high-grade, aggressive). Psammoma bodies may be present.
3. Chromophobe RCC — ~5%
Genetics: Multiple chromosome losses (1, 2, 6, 10, 13, 17, 21); arises from intercalated cells (like oncocytoma). Excellent prognosis.
Morphology: Large cells with pale, flocculent (web-like) cytoplasm and prominent cell borders (plant-cell-like). Hale's colloidal iron stain: diffuse cytoplasmic positivity (distinguishes from oncocytoma).
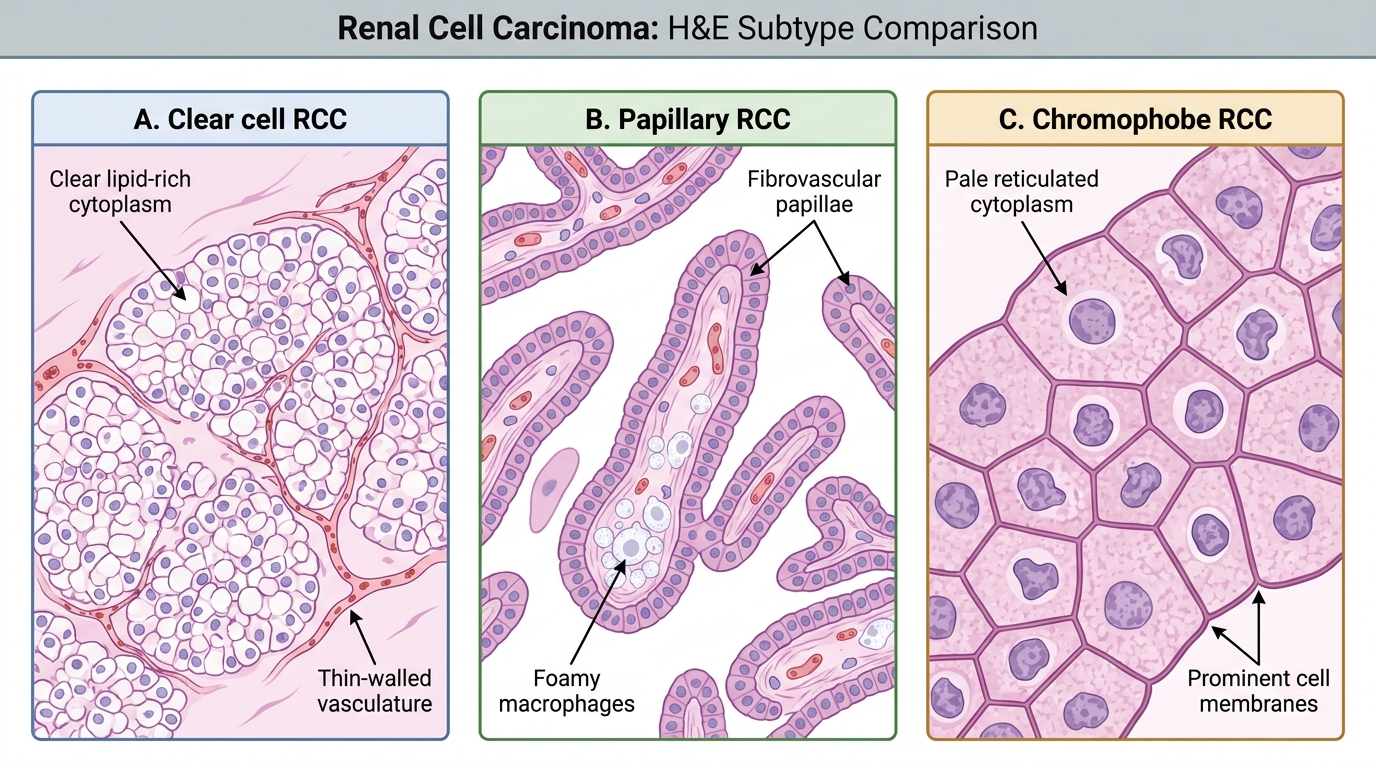
Renal Cell Carcinoma Subtypes on H&E