Page 15 of 27
PA27.{14,16} | Renal & Urothelial Tumours — SDL Guide (Part 3)
Urothelial (Transitional Cell) Carcinoma — Introduction and Risk Factors
Urothelial Carcinoma: Sites and Risk Factors
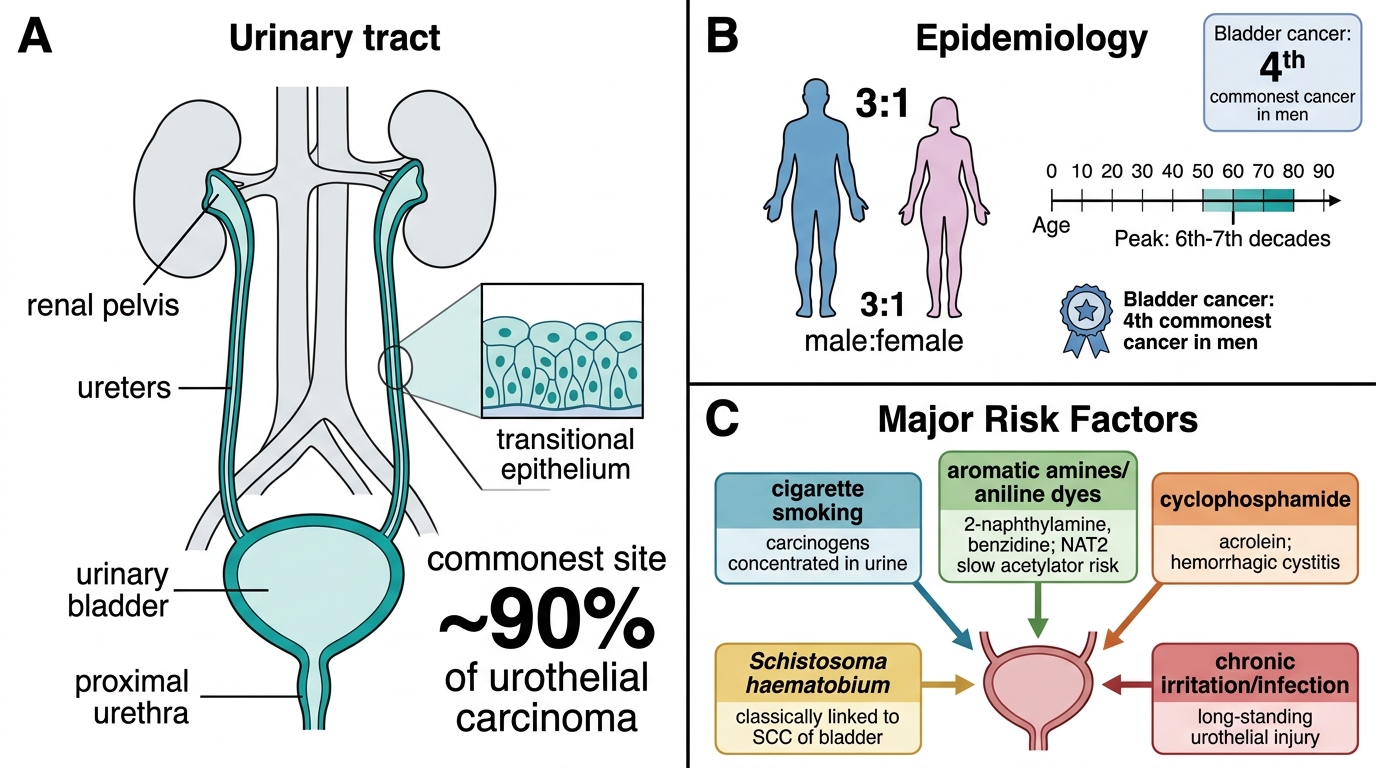
Urothelial carcinoma (UC) arises from the transitional epithelium (urothelium) lining the renal pelvis, ureters, bladder, and proximal urethra. The bladder is by far the commonest site (~90% of UC), followed by the renal pelvis, ureter, and urethra.
Bladder cancer is the 4th most common cancer in men in India and worldwide. The male:female ratio is ~3:1; peak incidence is in the 6th–7th decades.
Risk factors — the most important examination topic in urothelial carcinoma:
| Risk factor | Comment |
|---|---|
| Cigarette smoking | Single most important risk factor; 2–4× increased risk; carcinogens excreted in urine concentrate in the bladder |
| Aromatic amines / aniline dyes | Occupational exposure (textile workers, rubber industry, leather, printing); 2-naphthylamine and benzidine are classic carcinogens; urinary NAT2 slow-acetylator phenotype increases susceptibility |
| Cyclophosphamide | Metabolite acrolein is directly urotheliotoxic; haemorrhagic cystitis precedes malignancy |
| Schistosoma haematobium | Associated specifically with squamous cell carcinoma (SCC) of the bladder (not UC); eggs deposited in bladder wall → chronic inflammation → squamous metaplasia → SCC; endemic in Egypt and sub-Saharan Africa |
| Phenacetin abuse | Renal pelvis UC (analgesic nephropathy) |
| Pelvic irradiation | Long-term risk of UC |
Key teaching point: Schistosomiasis → SCC (not UC). This distinction appears regularly in MCQs.
Urothelial Carcinoma — Morphology, Grading, and Staging
Urothelial Carcinoma: Growth Pattern, Grade, and Stage
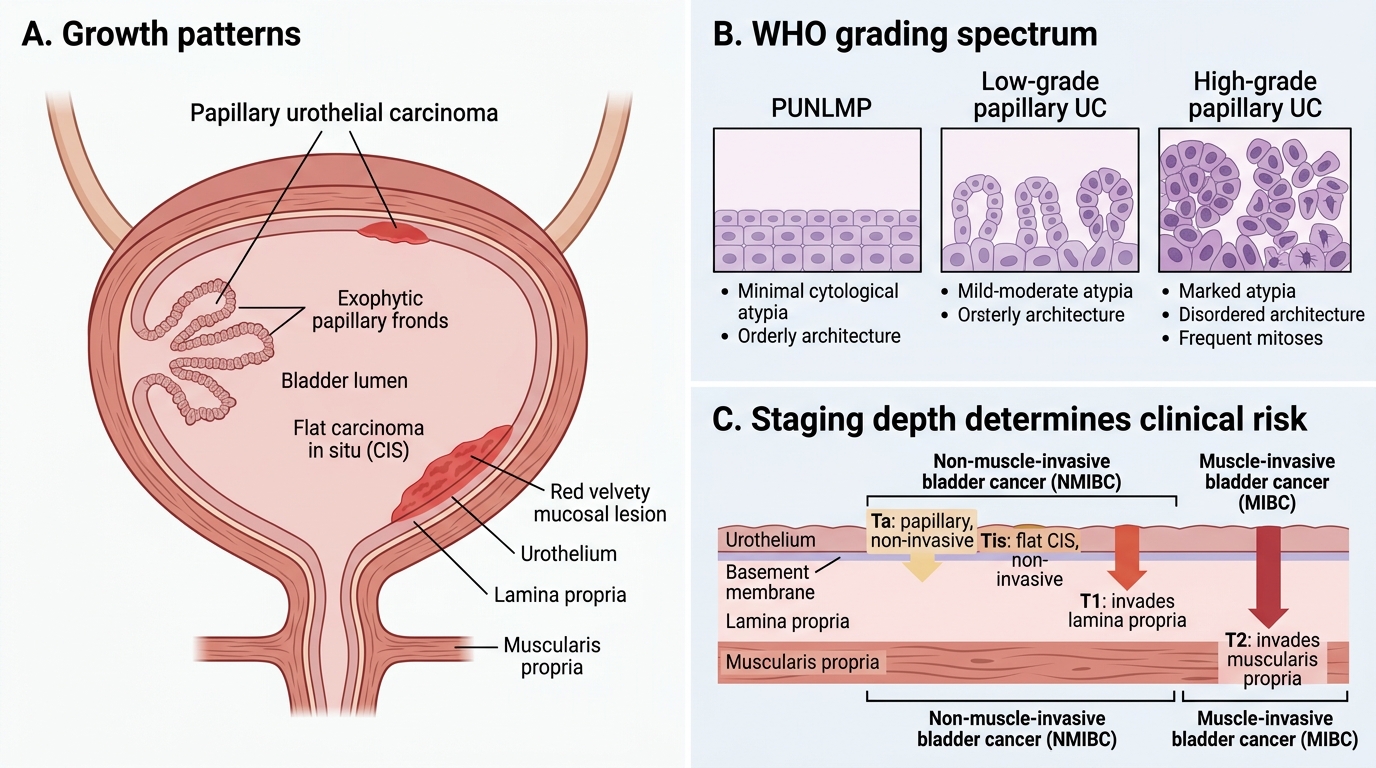
UC exists in two broad growth patterns with fundamentally different biology:
1. Papillary carcinoma
• Exophytic papillary fronds projecting into the bladder lumen
• Most common pattern; often low-grade
• Presents as painless haematuria; diagnosed on cystoscopy + biopsy
2. Flat carcinoma in situ (CIS)
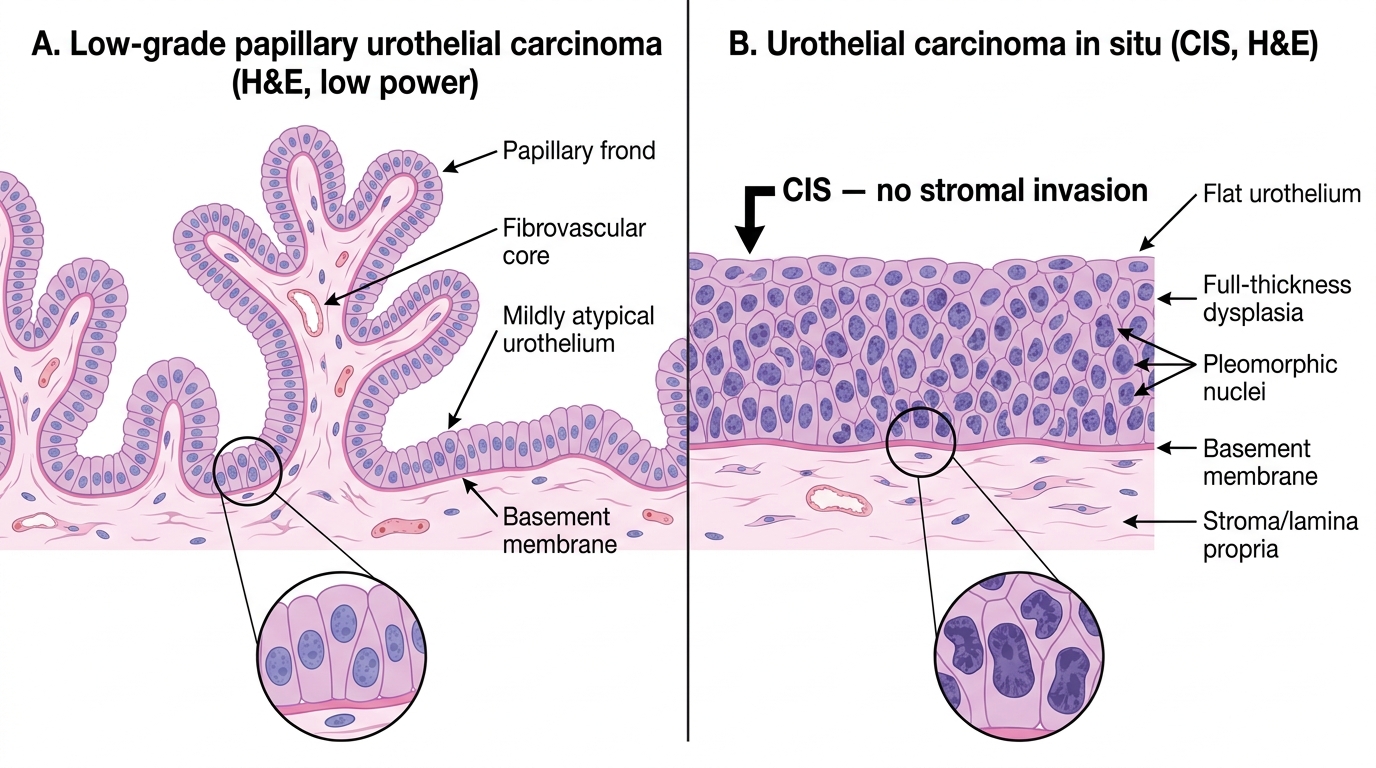
• Carcinoma in situ (CIS): flat, high-grade dysplastic urothelium confined to the mucosa; no exophytic growth
• Appears as red, velvety, ill-defined mucosal lesion on cystoscopy
• Despite being non-invasive by definition, CIS is high-grade and carries a significant risk of progression to muscle-invasive disease
Grading (WHO 2004/2016):
• PUNLMP (papillary urothelial neoplasm of low malignant potential): papillary lesion, minimal cytological atypia
• Low-grade papillary UC: mild-moderate atypia, orderly architecture
• High-grade papillary UC: marked atypia, disordered architecture, frequent mitoses
Staging — the critical clinical division:
| Stage | Description | Clinical term |
|---|---|---|
| Ta | Papillary, non-invasive (above basement membrane) | Non-muscle-invasive (NMIBC) |
| Tis (CIS) | Flat CIS, non-invasive | Non-muscle-invasive |
| T1 | Invades lamina propria (subepithelial connective tissue) | Non-muscle-invasive |
| T2 | Invades muscularis propria (detrusor) | Muscle-invasive (MIBC) |
| T3 | Invades perivesical fat | Muscle-invasive |
| T4 | Invades adjacent organs | Muscle-invasive |
The T2 boundary (muscularis propria invasion) is the critical threshold: NMIBC is managed with transurethral resection ± intravesical BCG; MIBC requires radical cystectomy ± systemic chemotherapy.
Papillary Urothelial Carcinoma vs Carcinoma in Situ
Urothelial Carcinoma — Clinical Features and Field Effect
Urothelial Carcinoma: Clinical Features and Field Effect
Presentation:
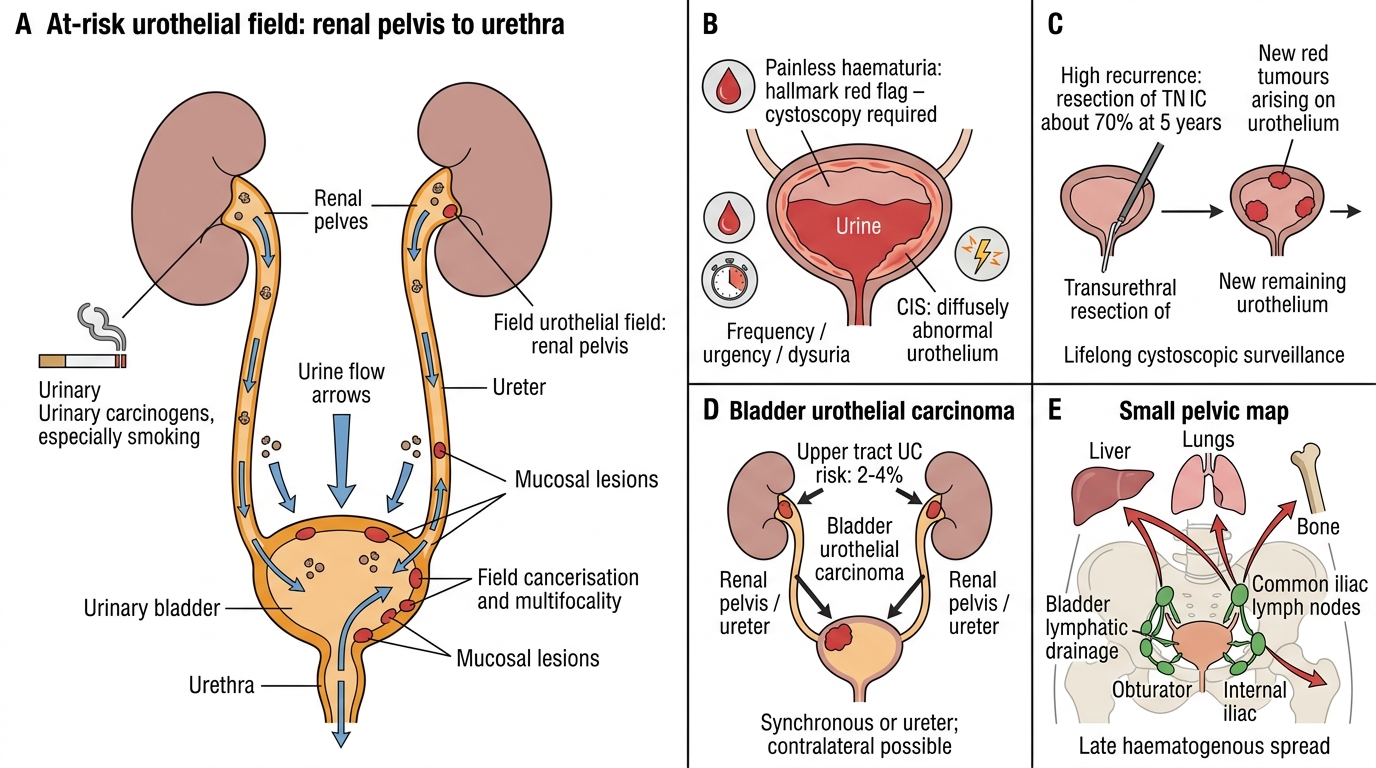
• Painless haematuria — the hallmark symptom; any age, any sex; blood in urine is a red-flag symptom that mandates cystoscopy
• Irritative symptoms — frequency, urgency, dysuria: especially with CIS (the urothelium is diffusely abnormal)
• Obstructive symptoms and hydronephrosis with ureteric involvement
The field effect and its clinical consequences:
The field effect (field cancerisation) describes the tendency of the entire urothelium — from renal pelvis to urethra — to undergo malignant transformation when exposed to carcinogens excreted in urine. Consequences:
- Multifocality: multiple synchronous tumours at different urothelial sites at presentation
- High recurrence rate: even after complete resection of a NMIBC, carcinogens bathing residual urothelium drive new tumours; recurrence rate ~70% at 5 years
- Surveillance by cystoscopy: mandatory lifelong follow-up
- Upper tract UC: patients with bladder UC have a 2–4% risk of synchronous or metachronous renal pelvis / ureter tumours (contralateral involvement possible)
This field effect concept explains why bladder cancer behaves so differently from solid organ tumours where surgical excision is often curative: the at-risk surface is vast, and the carcinogen exposure is continuous as long as the patient smokes.
Lymphatic spread: to obturator, internal iliac, and common iliac nodes.
Haematogenous spread: liver, lungs, bone (late).
SELF-CHECK
A 62-year-old male textile dye worker presents with three separate episodes of painless haematuria over 6 months. Cystoscopy reveals two papillary lesions and one red velvety mucosal area. Biopsy of the velvety area shows full-thickness urothelial atypia without stromal invasion. Which statement about his disease is MOST accurate?
A. The velvety lesion (CIS) is low-grade and unlikely to progress to muscle-invasive disease
B. The most probable occupational carcinogen is acrolein from cyclophosphamide metabolism
C. The multifocal pattern reflects field cancerisation from carcinogens excreted in urine
D. Schistosoma haematobium is the most likely aetiological agent in this case
Reveal Answer
Answer: C. The multifocal pattern reflects field cancerisation from carcinogens excreted in urine
Multifocal synchronous tumours (papillary + CIS) in a patient with occupational aromatic amine exposure perfectly illustrate field cancerisation — the entire urothelium is at risk because carcinogens concentrate in urine and bathe the whole surface. CIS is high-grade (not low-grade) and carries significant progression risk. Acrolein is a cyclophosphamide metabolite; aromatic amines (2-naphthylamine, benzidine) are the relevant dye-industry carcinogens. Schistosomiasis causes SCC, not UC.
CLINICAL PEARL
Occupation → carcinogen → tumour type: the exam matrix
| Exposure | Carcinogen | Tumour |
|---|---|---|
| Textile / dye workers | 2-naphthylamine, benzidine (aromatic amines) | Urothelial carcinoma |
| Smoking | β-naphthylamine + polycyclic aromatic hydrocarbons | Urothelial carcinoma |
| Cyclophosphamide therapy | Acrolein | Urothelial carcinoma |
| Schistosoma haematobium | Chronic mucosal injury → squamous metaplasia | Squamous cell carcinoma |
Note that schistosomiasis → SCC, not UC. This distinction is reliably tested. Also remember: painless haematuria in any adult = cystoscopy mandatory until proven otherwise — bladder cancer is too important to miss.
Summary Table — Comparing the Major Renal Tumours
Comparison of Major Renal and Urinary Tract Tumours
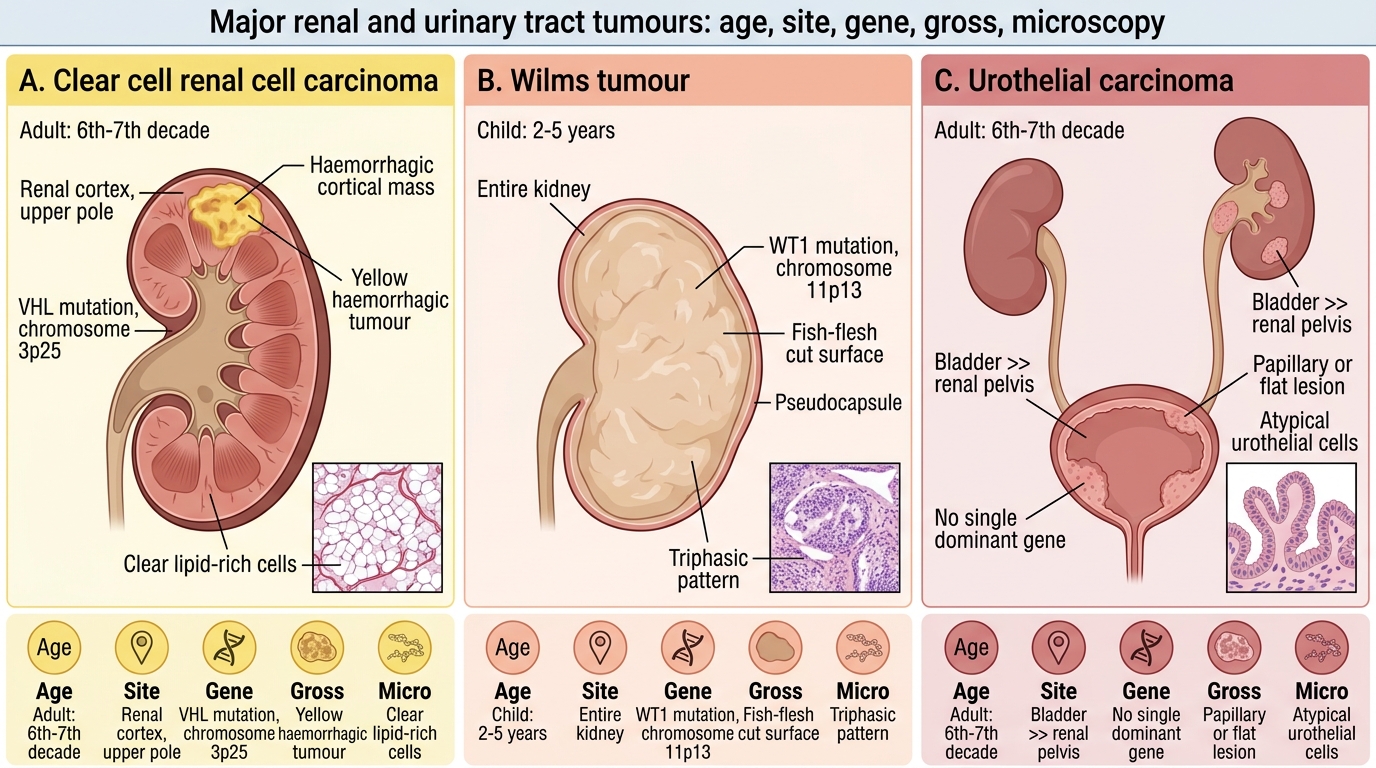
| Feature | Clear cell RCC | Wilms tumour | Urothelial carcinoma |
|---|---|---|---|
| Age group | Adults (6th–7th decade) | Children (2–5 years) | Adults (6th–7th decade) |
| Site | Renal cortex (upper pole) | Entire kidney | Bladder >> renal pelvis |
| Key gene | VHL (3p25) | WT1 (11p13) | None single dominant |
| Gross | Yellow, haemorrhagic | Fish-flesh, pseudocapsule | Papillary or flat |
| Micro | Clear lipid-rich cells, sinusoidal vasculature | Triphasic (blast/epi/stroma) | Papillary fronds or flat CIS |
| Hallmark symptom | Haematuria + flank mass | Painless abdominal mass | Painless haematuria |
| Spread | Renal vein/IVC; cannonball lungs | Lymph nodes; haematogenous | Lymphatic; field recurrence |
| Key risk factor | Smoking, VHL mutation, obesity | WT1 germline loss | Smoking, aromatic amines |