Page 1 of 27
PA27.8-10 | Tubulointerstitial Diseases, ATN & Pyelonephritis — SDL Guide
Learning Objectives
- Classify diseases affecting the tubular interstitium using a clinically useful framework (ischaemic, toxic, infective, immune/allergic, metabolic, obstructive).
- Describe the pathogenesis, morphology, and three clinical phases of acute tubular necrosis (ATN).
- Compare ischaemic and nephrotoxic ATN with respect to tubular injury pattern and causative agents.
- Outline the etiology, predisposing factors, pathology, and complications of acute pyelonephritis, including the significance of WBC casts.
- Distinguish chronic pyelonephritis from reflux nephropathy and recognise thyroidisation as a morphological hallmark.
- Identify the distinctive histological features of drug-induced allergic interstitial nephritis and analgesic nephropathy.
INSTRUCTIONS
Tubulointerstitial diseases account for the majority of cases of acute kidney injury seen in hospital settings, yet they are frequently overshadowed by glomerular pathology in teaching. This module builds directly on your Year-1 renal physiology and the renal-I block: understanding how tubular epithelia respond to ischaemia and toxins — and how the interstitium reacts to infection and drugs — gives you a mechanistic framework for managing AKI and UTI complications in clinical postings. Work through each section actively, pausing at the micro-quizzes to test your reasoning before reading the explanations.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 20 — The Kidney (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 22 — The Kidney and Lower Urinary Tract (textbook)
- NMC CBUC 2024, Competencies PA27.8–PA27.10 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man with type-2 diabetes develops fever, rigors, and right-flank pain three days after an elective coronary angiogram. His serum creatinine — normal at admission — has risen sharply. Urine microscopy shows neutrophils and WBC casts. Is this contrast-induced acute tubular necrosis? Ascending pyelonephritis? Could it be both? By the end of this module you will have the pathological tools to answer this — and to explain why his diabetes makes him especially vulnerable.
WHY THIS MATTERS
Tubulointerstitial diseases are the single most common cause of acute kidney injury (AKI) in hospitalised patients. ATN alone accounts for roughly 75 % of intrinsic AKI in ICUs. Pyelonephritis is one of the most frequent serious bacterial infections encountered in clinical practice, and its complications — papillary necrosis, pyonephrosis — are life-threatening. Recognising the urine sediment patterns (granular casts in ATN, WBC casts in pyelonephritis) guides immediate management decisions you will make in medicine and surgery postings.
RECALL
Before proceeding, revisit these Year-1 concepts:
- Tubular anatomy: proximal convoluted tubule (PCT), loop of Henle, distal convoluted tubule — which segment is most energy-dependent and therefore most vulnerable to ischaemia?
- GFR determinants: hydrostatic and oncotic forces; how does tubular obstruction (cast formation) reduce GFR?
- Urine sediment: what distinguishes granular casts from cellular casts?
- Vesicoureteric reflux (VUR): grading I–V; how does high-grade reflux predispose to renal scarring?
- Normal urothelial defence: urine flow, Tamm-Horsfall protein, bladder mucosal defences against ascending infection.
Classification of Tubulointerstitial Diseases
Classification of Tubulointerstitial Diseases
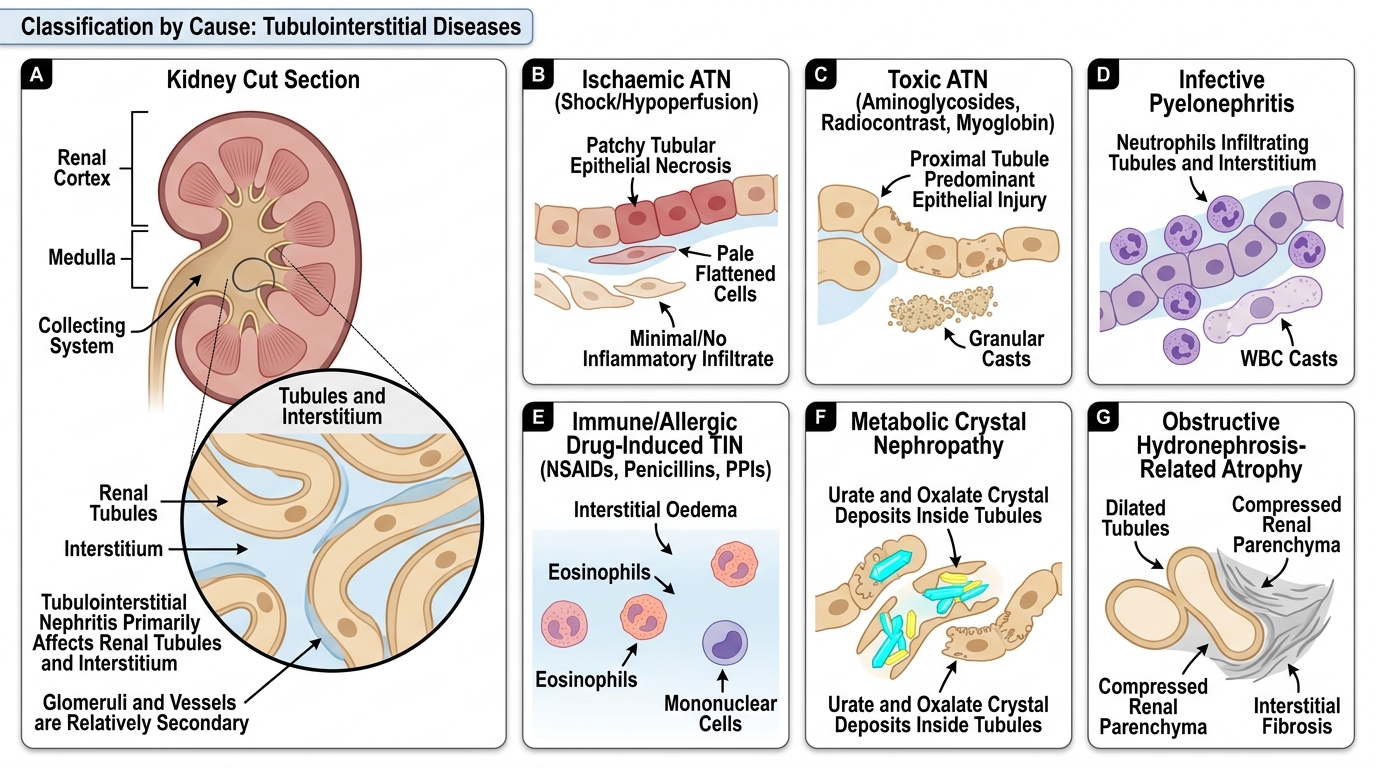
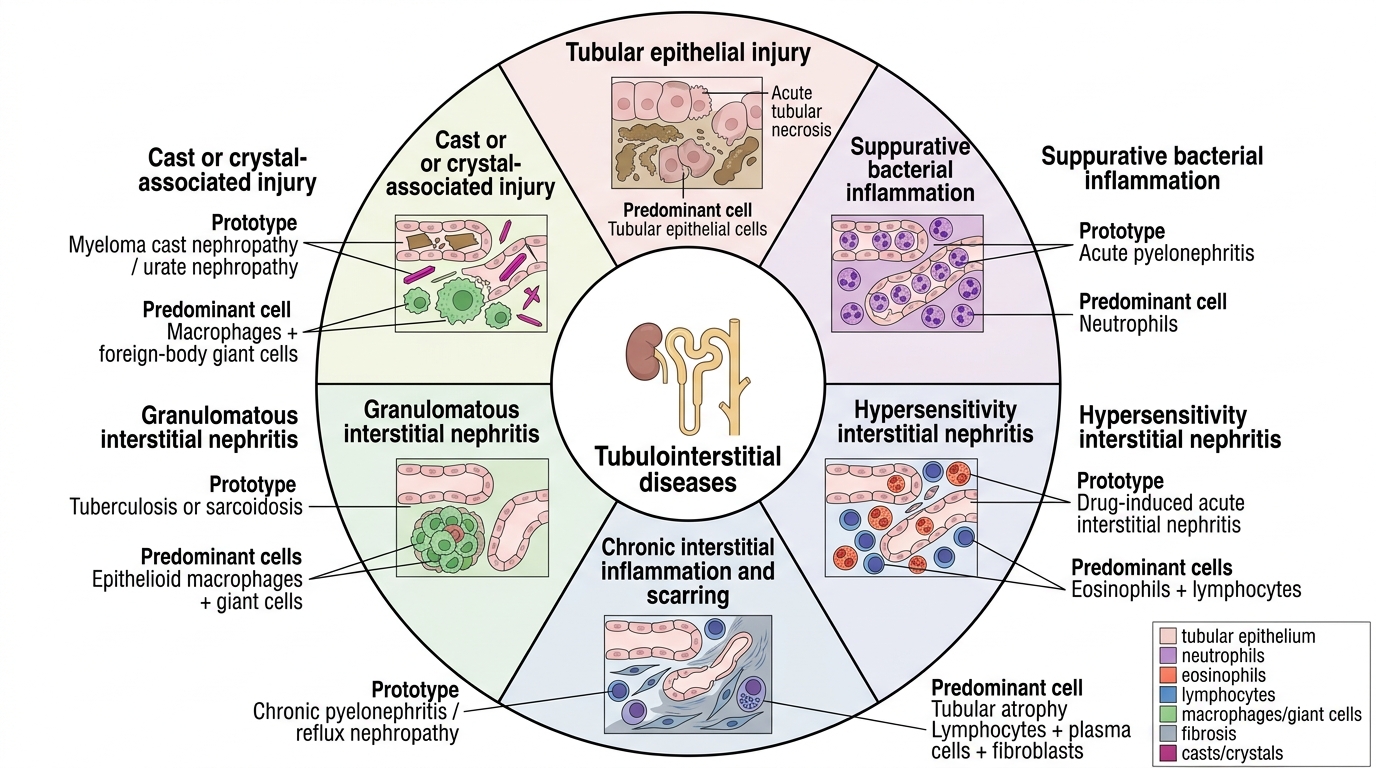
Tubulointerstitial nephritis (TIN) encompasses a heterogeneous group of disorders that primarily injure the renal tubules and interstitium rather than glomeruli or vasculature. A clinically anchored classification uses the cause:
| Category | Prototype | Key Feature |
|---|---|---|
| Ischaemic | ATN (shock, hypoperfusion) | Patchy tubular necrosis, no inflammation |
| Toxic | ATN (aminoglycosides, contrast, myoglobin) | Proximal tubule predominant |
| Infective | Acute / chronic pyelonephritis | Neutrophilic, WBC casts |
| Immune / allergic | Drug-induced TIN (NSAIDs, penicillins, PPIs) | Eosinophils, mononuclear cells |
| Metabolic | Urate nephropathy, oxalate nephropathy | Crystal deposits |
| Obstructive | Hydronephrosis-related atrophy | Tubular dilation, interstitial fibrosis |
The distinction between acute and chronic TIN rests on reversibility and on whether interstitial fibrosis has supervened. Acute TIN recovers if the insult is removed; chronic TIN leaves permanent nephron loss.
Classification of Tubulointerstitial Diseases
Acute Tubular Necrosis — Pathogenesis
Acute Tubular Necrosis: Pathogenesis
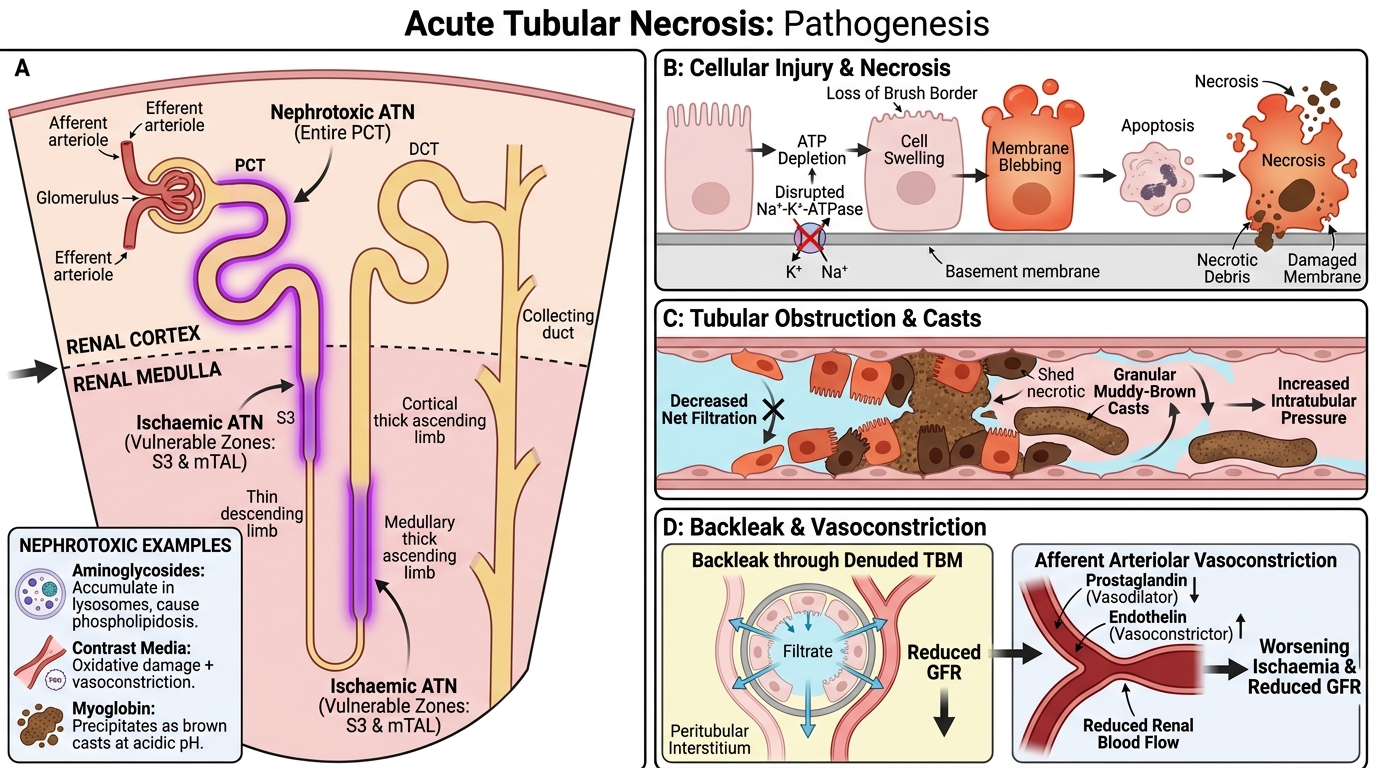
Acute tubular necrosis (ATN) is the most important cause of intrinsic AKI and follows either severe ischaemia or direct nephrotoxic injury to tubular epithelial cells. Four interdependent mechanisms drive the fall in GFR:
- Tubular cell injury and death — ischaemia depletes ATP, disrupting Na⁺-K⁺-ATPase and causing cell swelling, blebbing of brush border, and apoptosis or necrosis of epithelial cells.
- Tubular obstruction — shed necrotic cells and precipitated Tamm-Horsfall protein form granular (muddy-brown) casts that physically block tubular lumens, raising intratubular pressure and reducing net filtration.
- Backleak — the denuded basement membrane allows filtered glomerular fluid to leak back into the peritubular interstitium, further reducing effective GFR.
- Vasoconstriction — local prostaglandin and endothelin imbalance produces persistent afferent arteriolar constriction, compounding ischaemia.
Ischaemic ATN preferentially injures the straight segment of the PCT (S3) and the medullary thick ascending limb — two segments with high metabolic demand and low collateral oxygen supply.
Nephrotoxic ATN concentrates injury in the entire PCT because toxins are actively transported or concentrated here. Aminoglycosides accumulate in lysosomes and trigger phospholipidosis; contrast media cause direct oxidative damage and vasoconstriction; myoglobin (released in rhabdomyolysis) is directly toxic and precipitates as brown casts at acidic pH.
SELF-CHECK
In ATN, which mechanism directly reduces the net filtration pressure even when glomerular blood flow is partially maintained?
A. Eosinophilic infiltration of the interstitium
B. Backleak of filtrate through the denuded tubular basement membrane
C. Fusion of podocyte foot processes reducing Kf
D. Deposition of immune complexes in the mesangium
Reveal Answer
Answer: B. Backleak of filtrate through the denuded tubular basement membrane
Backleak — movement of glomerular filtrate back into the peritubular capillaries through damaged, denuded basement membrane — is unique to ATN. It raises intratubular pressure and reduces the effective GFR even without further reduction in renal blood flow. Eosinophilic interstitial infiltration characterises drug-induced TIN, not ATN. Podocyte fusion and mesangial immune complexes are glomerular mechanisms.
Acute Tubular Necrosis — Morphology
Acute Tubular Necrosis: Morphology
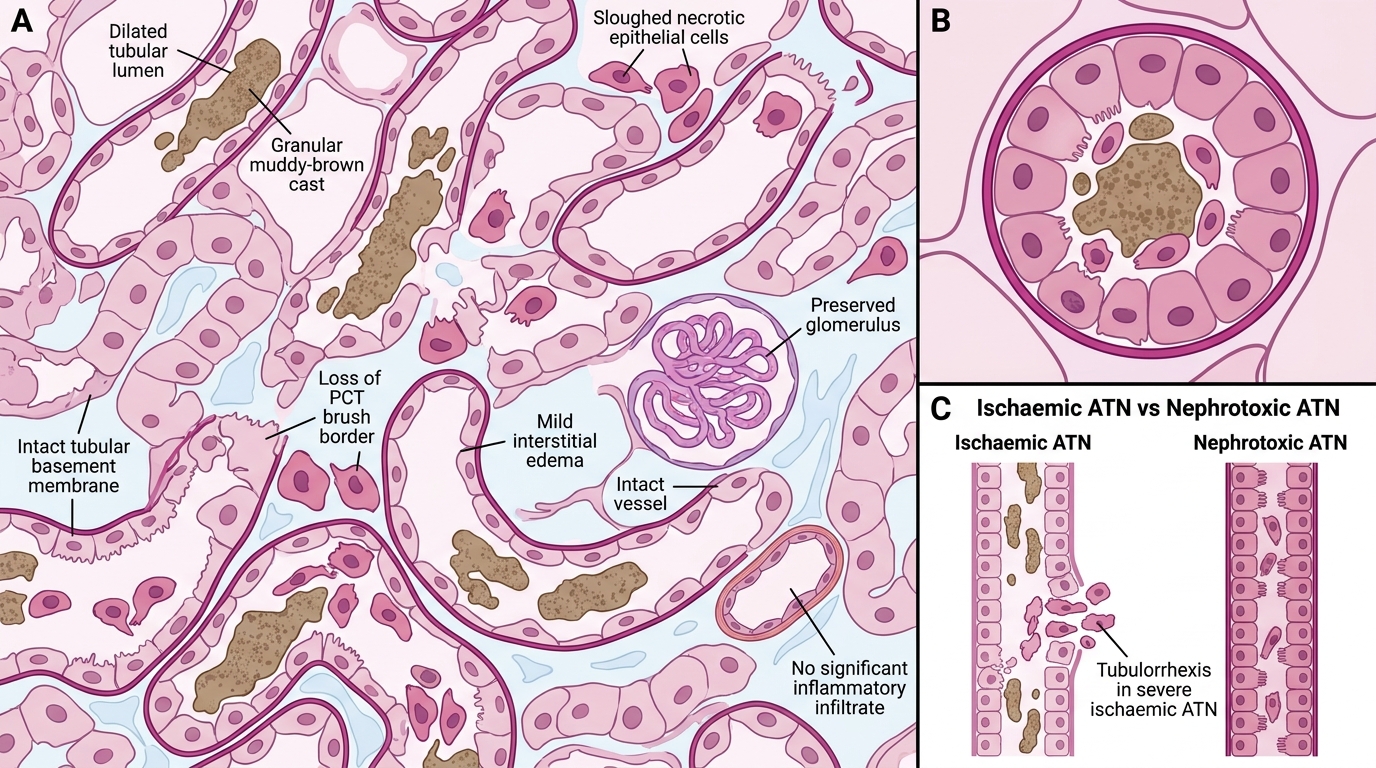
On light microscopy the cardinal features are:
- Tubular epithelial necrosis and sloughing — necrotic cells lose their polarity, detach from the basement membrane, and lie free in the lumen. The PCT shows loss of brush border.
- Dilated tubular lumens — segments downstream of the obstruction dilate as casts accumulate.
- Granular (muddy-brown) casts — composed of necrotic cell debris, Tamm-Horsfall protein, and (in rhabdomyolysis) myoglobin. These are the morphological hallmark.
- Tubular basement membrane rupture (tubulorrhexis) — seen in severe ischaemic ATN; absent in nephrotoxic ATN, where basement membrane integrity is preserved despite necrosis.
- Interstitium — mild oedema but NO significant inflammatory infiltrate (this distinguishes ATN from pyelonephritis).
- Glomeruli and vessels — intact (important negative finding).
Ischaemic vs. nephrotoxic: Ischaemic ATN shows patchy, skip-lesion necrosis along the tubule; nephrotoxic ATN shows diffuse, uniform necrosis confined to the PCT.
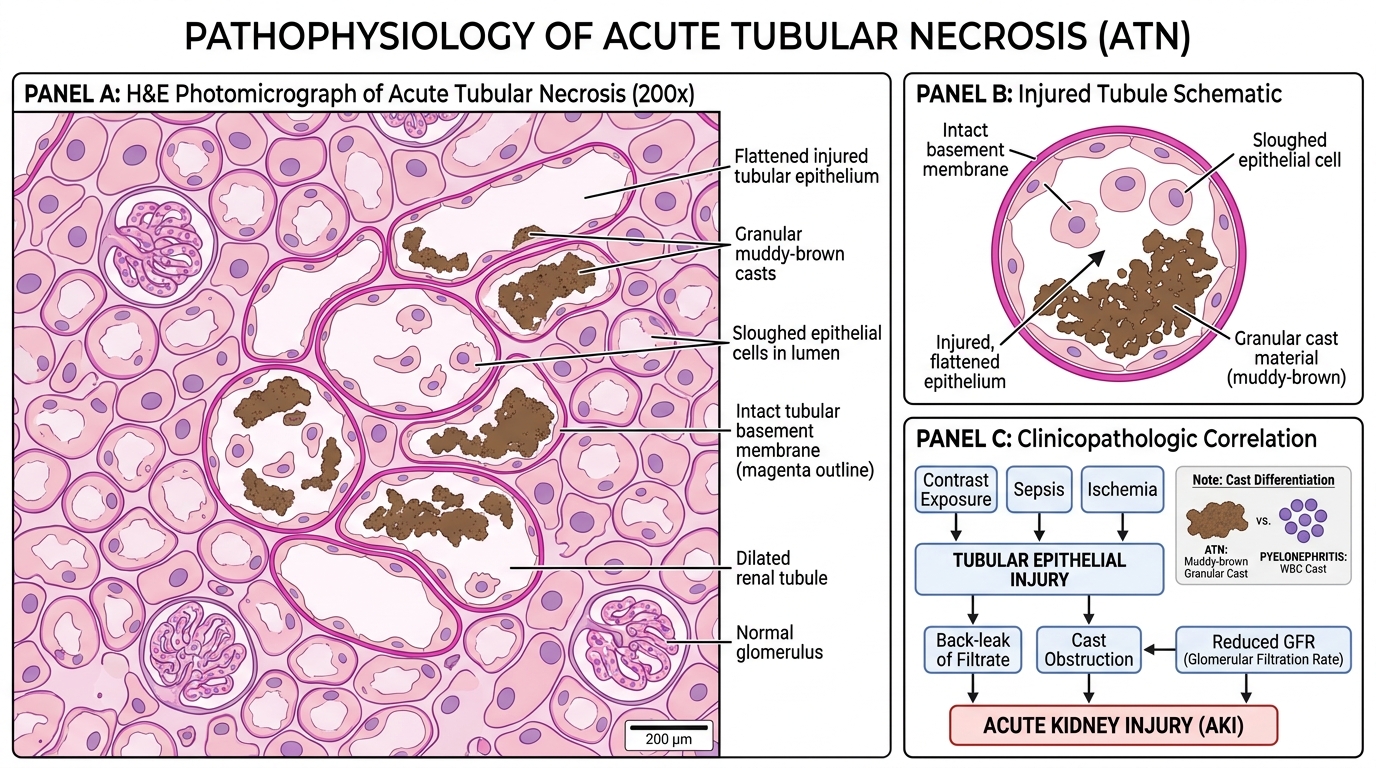
Acute Tubular Necrosis: Histology and Clinical Correlation