Page 2 of 27
PA27.8-10 | Tubulointerstitial Diseases, ATN & Pyelonephritis — SDL Guide (Part 2)
Three Clinical Phases of ATN
Three Clinical Phases of Acute Tubular Necrosis
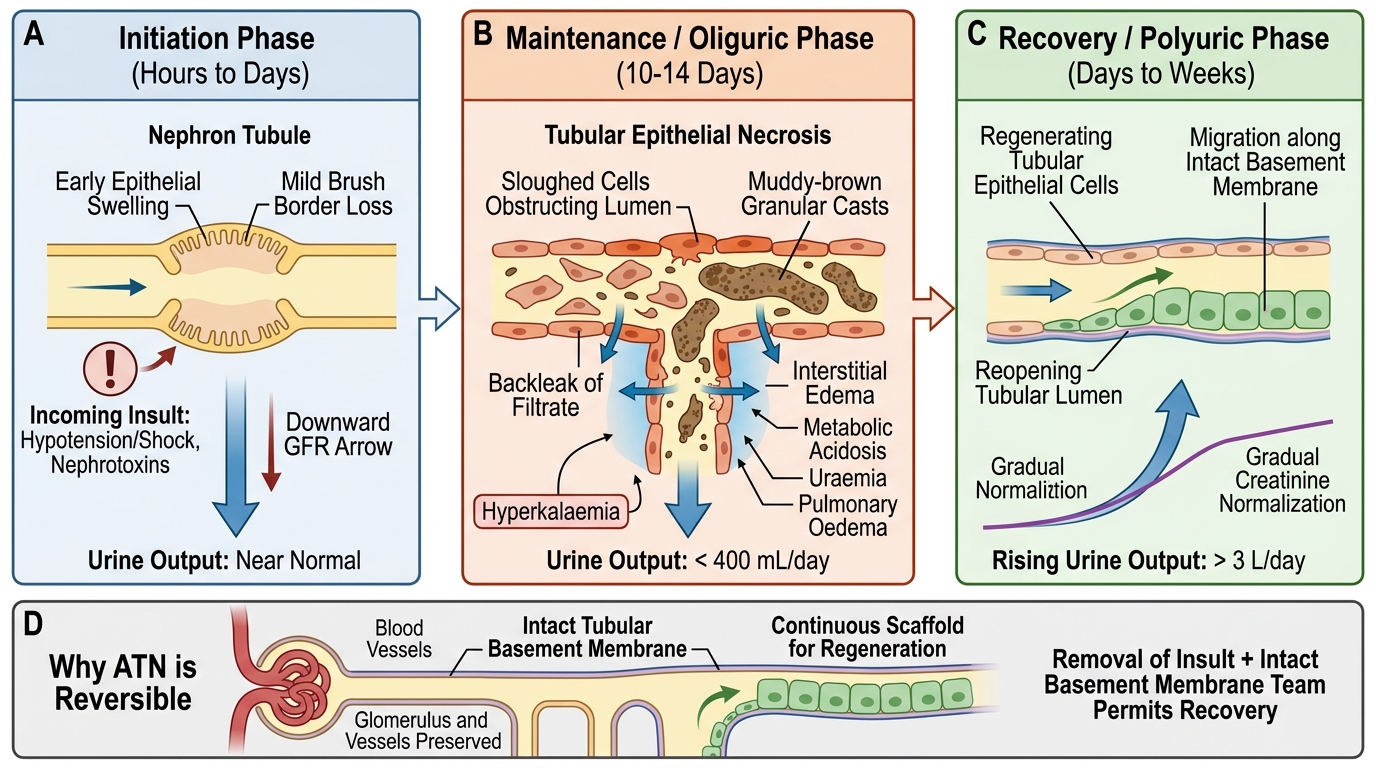
ATN runs a stereotyped triphasic course that directly reflects the underlying tubular biology:
1. Initiation phase (hours to days)
The triggering insult (shock episode, nephrotoxin exposure) is ongoing or just-resolved. GFR begins to fall but urine output may still be near-normal. Clinically subtle — easy to miss without serial creatinine monitoring.
2. Maintenance / oliguric phase (typically 10–14 days)
Established tubular injury. Urine output falls to <400 mL/day (oliguria) in about 50 % of cases; non-oliguric ATN (urine output preserved but GFR still low) carries a better prognosis. Complications: hyperkalaemia, metabolic acidosis, uraemia, pulmonary oedema. The muddy-brown casts are most abundant here. This phase is NOT shortened by diuretics — forced diuresis does not accelerate tubular repair.
3. Recovery / polyuric phase (days to weeks)
Tubular epithelial regeneration begins. Surviving cells dedifferentiate, proliferate, and migrate along the basement membrane. As tubular function recovers before tubular concentration capacity normalises, a polyuric phase supervenes — urine output can exceed 3 L/day, risking hypokalaemia and dehydration. Creatinine gradually normalises over weeks.
Key point on reversibility: The intact tubular basement membrane (especially in nephrotoxic ATN) acts as a scaffold for regeneration. As long as glomeruli and vessels are unaffected and the insult is removed, full recovery is expected — this is what distinguishes ATN from chronic intrinsic renal failure.
SELF-CHECK
A patient in the maintenance phase of ATN has urine output of 600 mL/day. Which of the following urine findings is most characteristic?
A. Red cell casts and proteinuria >3.5 g/day
B. WBC casts and pyuria with bacteriuria
C. Granular muddy-brown casts with epithelial cell casts
D. Waxy casts and broad casts suggesting chronic disease
Reveal Answer
Answer: C. Granular muddy-brown casts with epithelial cell casts
Granular (muddy-brown) casts composed of necrotic tubular epithelial cells and Tamm-Horsfall protein are the hallmark of ATN and are most abundant during the maintenance phase. Red cell casts with heavy proteinuria point to glomerulonephritis (nephritic syndrome). WBC casts and pyuria indicate pyelonephritis. Waxy and broad casts indicate chronic renal failure with wide, atrophic tubules.
CLINICAL PEARL
Rhabdomyolysis-induced ATN deserves special mention for MBBS exams and clinical practice. Crush injuries, prolonged immobilisation, statin toxicity, and extreme exertion release myoglobin into the blood. Myoglobin is freely filtered at the glomerulus and reaches the tubule in high concentration. At the low pH typical of ischaemic or dehydrated tubular fluid, myoglobin co-precipitates with Tamm-Horsfall protein to form pigmented casts. The clinical triad: muscle pain/weakness + cola-coloured urine + AKI. Urine dipstick tests positive for blood (myoglobin cross-reacts) but microscopy shows no red cells — this discrepancy is a key diagnostic clue. Treatment: aggressive IV fluid hydration to alkalinise urine and flush casts.
Acute Pyelonephritis — Etiology and Pathogenesis
Acute Pyelonephritis: Routes and Risk Factors
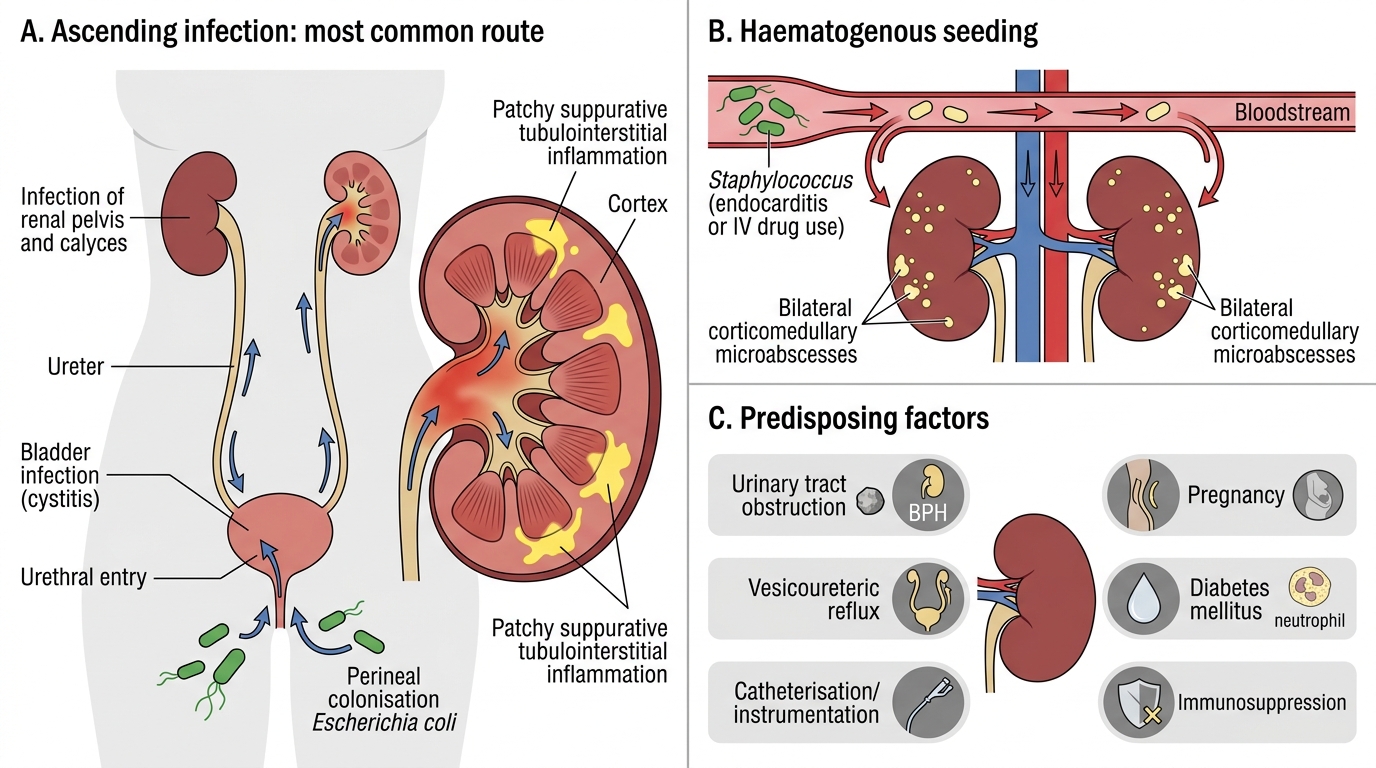
Acute pyelonephritis (APN) is a bacterial infection of the renal pelvis, calyces, and parenchyma, causing suppurative tubulointerstitial inflammation.
Route of infection:
- Ascending (most common, ~85 %) — perineal colonisation → urethral entry → bladder → ureter → kidney. Escherichia coli accounts for 80 % of community-acquired APN; other Gram-negatives: Klebsiella, Proteus, Enterobacter.
- Haematogenous — bacteraemic seeding, typically Staphylococcus aureus (endocarditis, IV drug use). Produces bilateral corticomedullary microabscesses.
Predisposing factors (important for exam):
| Factor | Mechanism |
|---|---|
| Urinary tract obstruction (stones, BPH) | Urine stasis, impaired washout |
| Vesicoureteric reflux (VUR) | Retrograde pressure and bacteria |
| Urinary instrumentation / catheterisation | Breaks urothelial barrier |
| Pregnancy | Ureteric compression, bladder hypomotility |
| Diabetes mellitus | Impaired neutrophil function, glycosuria |
| Immunosuppression | Reduced host defence |
Bacterial virulence: uropathogenic E. coli possesses P fimbriae (bind uroepithelium), α-haemolysin, and aerobactin (iron acquisition).
Acute Pyelonephritis — Morphology and Complications
Acute Pyelonephritis: Morphology and Complications
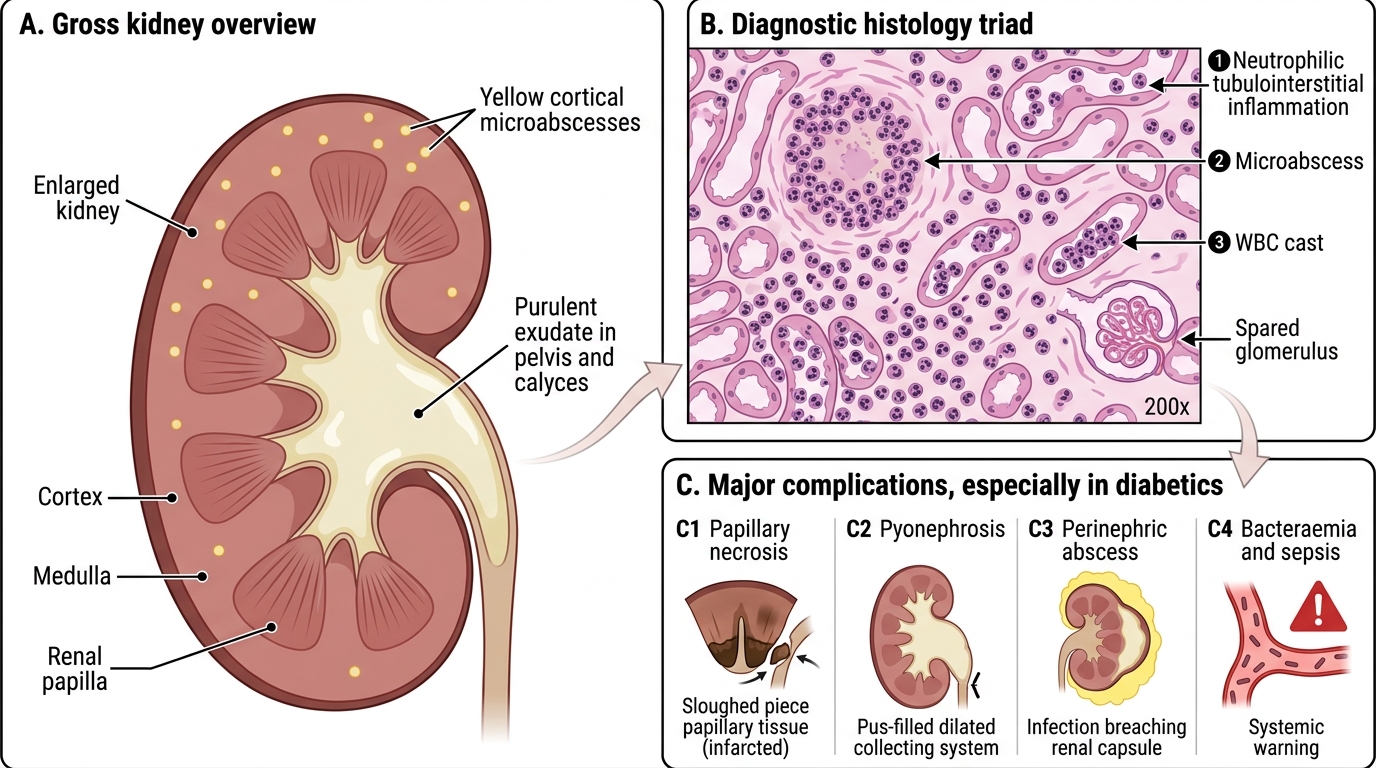
Gross appearance: kidney enlarged; cortical surface shows yellowish microabscesses. Pelvis and calyces contain purulent exudate.
Histology (the diagnostic triad):
1. Neutrophilic tubulointerstitial inflammation — tubules filled with neutrophils; interstitial oedema and neutrophil exudate.
2. Microabscesses — focal areas of tubular destruction with central necrosis and neutrophil accumulation.
3. WBC (neutrophil) casts — neutrophils aggregate in tubular lumens and are shed as casts in urine. Their presence proves renal parenchymal infection (not mere bladder infection).
Glomeruli are usually spared in typical APN (important contrast with glomerulonephritis).
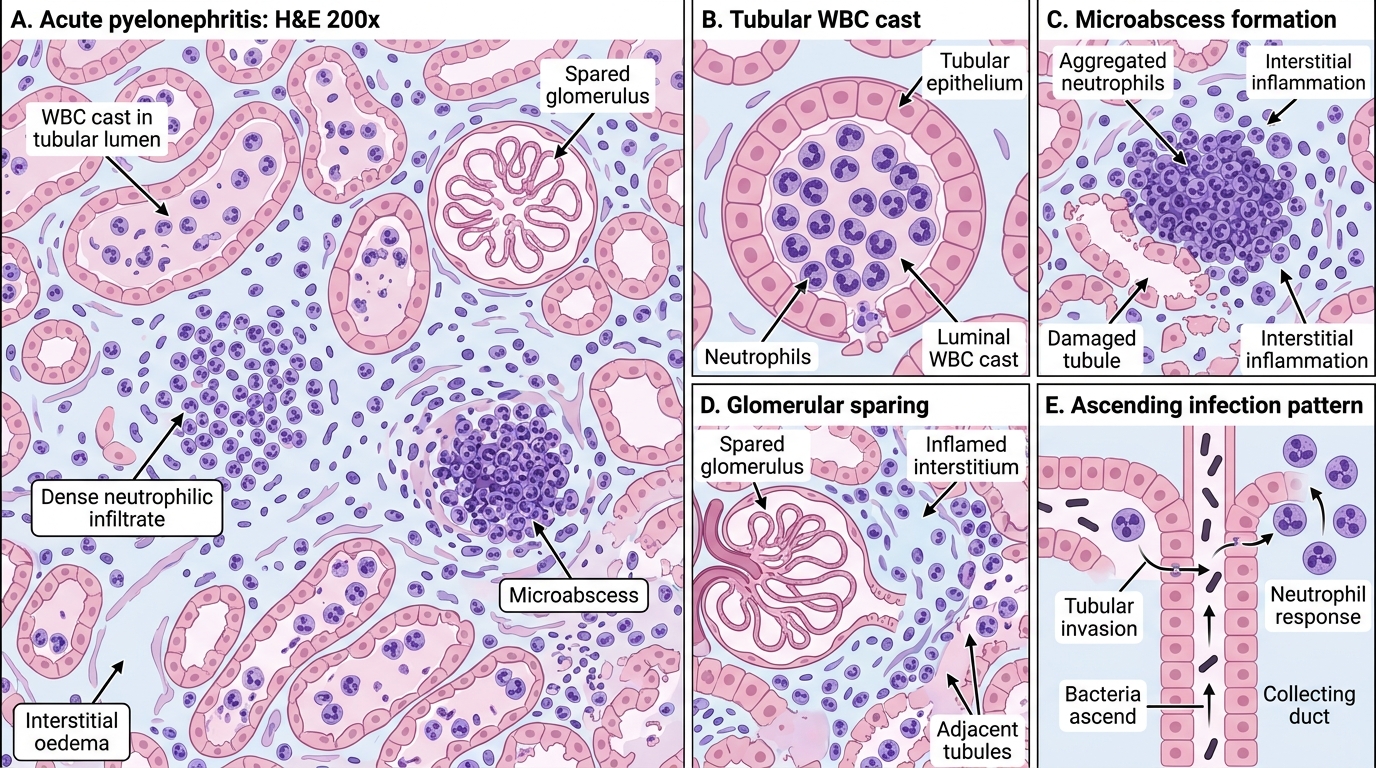
Acute Pyelonephritis: Tubulointerstitial Suppurative Inflammation
Complications (especially in diabetics):
- Papillary necrosis — ischaemic infarction of renal papillae (tips of pyramids) due to combined vascular disease, infection, and analgesic use. Sloughed papilla can obstruct ureter → colic + worsening AKI.
- Pyonephrosis — when complete obstruction exists above an infected kidney; the entire collecting system fills with pus.
- Perinephric abscess — infection breaks through the renal capsule into perirenal fat; requires drainage.
- Bacteraemia and sepsis — particularly in elderly and diabetic patients.
SELF-CHECK
Which finding on urine microscopy is pathognomonic of renal parenchymal infection (pyelonephritis) rather than lower urinary tract infection (cystitis)?
A. Pyuria (>5 WBCs per HPF)
B. Bacteriuria on Gram stain
C. WBC (neutrophil) casts
D. Granular casts
Reveal Answer
Answer: C. WBC (neutrophil) casts
WBC casts form when neutrophils aggregate inside renal tubules — this can only happen in the kidney, not the bladder or urethra. Their presence is therefore pathognomonic of renal parenchymal involvement. Pyuria and bacteriuria occur in both upper and lower UTI. Granular (muddy-brown) casts are the hallmark of ATN, not infection.