Page 3 of 27
PA27.8-10 | Tubulointerstitial Diseases, ATN & Pyelonephritis — SDL Guide (Part 3)
Chronic Pyelonephritis and Reflux Nephropathy
Chronic Pyelonephritis and Reflux Nephropathy
Chronic pyelonephritis (CPN) is the result of repeated or persistent bacterial infections producing progressive renal scarring, tubular atrophy, and interstitial fibrosis. It is a morphological diagnosis — scarring is the defining feature, not bacterial cultures.
Two types:
1. Reflux nephropathy (most common form of CPN):
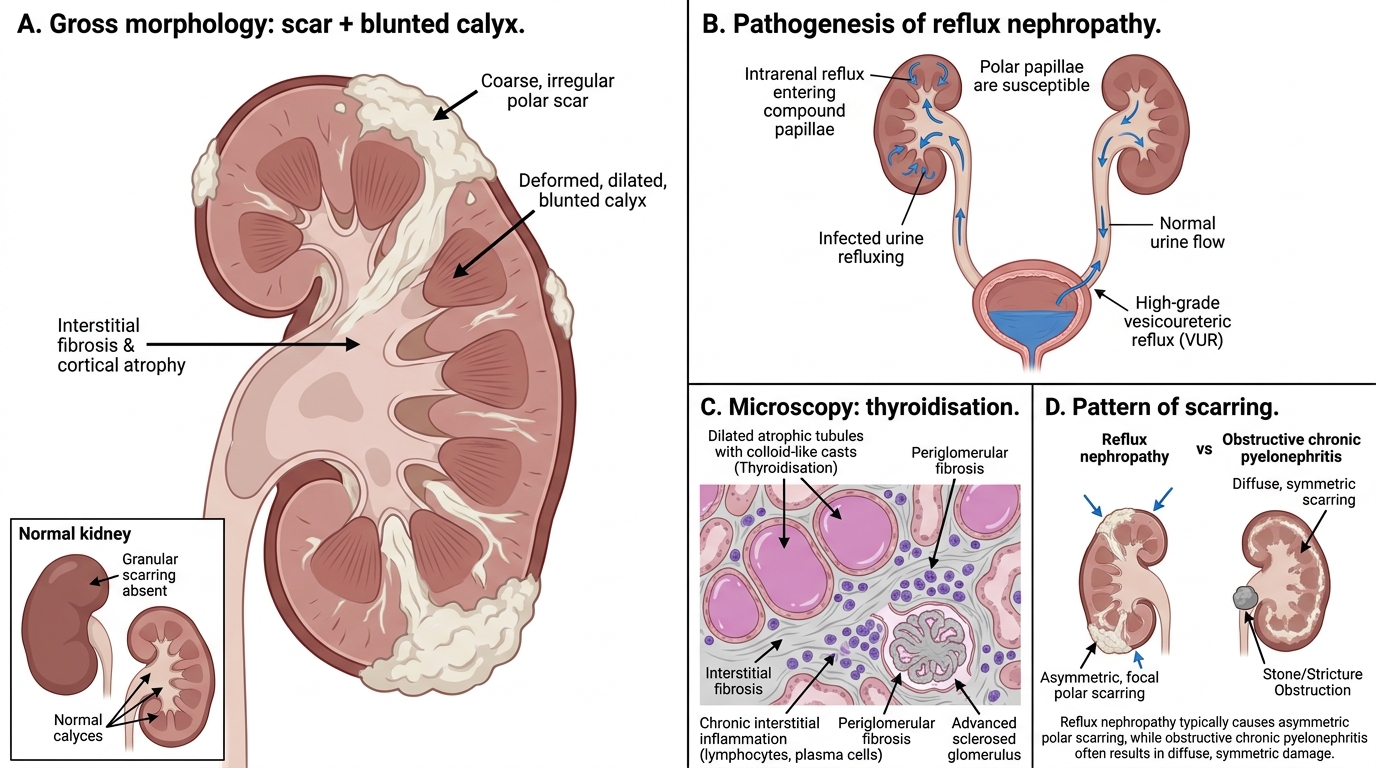
High-grade vesicoureteric reflux allows infected urine to enter the collecting system under pressure. Intrarenal reflux (compound papillae at the poles allow urine to enter collecting ducts) generates polar scars disproportionately affecting the upper and lower poles. Even sterile reflux in children can cause progressive scarring.
2. Obstructive CPN:
Repeated infections in the context of fixed obstruction (stones, strictures) cause diffuse symmetric scarring.
Gross morphology (hallmark):
- Coarse, irregular, corticomedullary scars overlying deformed, dilated, blunted calyces. This calyceal blunting distinguishes CPN from other causes of renal scarring (glomerulosclerosis produces a granular contracted surface without calyceal change).
- Polar distribution in reflux nephropathy.
Microscopic morphology:
- Tubular atrophy with inspissated colloid casts — thyroidisation (the dilated tubules filled with homogeneous eosinophilic material resemble thyroid follicles).
- Periglomerular fibrosis; glomerulosclerosis in advanced cases.
- Chronic interstitial inflammation (lymphocytes, plasma cells).
Clinical consequence: hypertension (RAAS activation from scars) and proteinuria; may progress to ESRD.
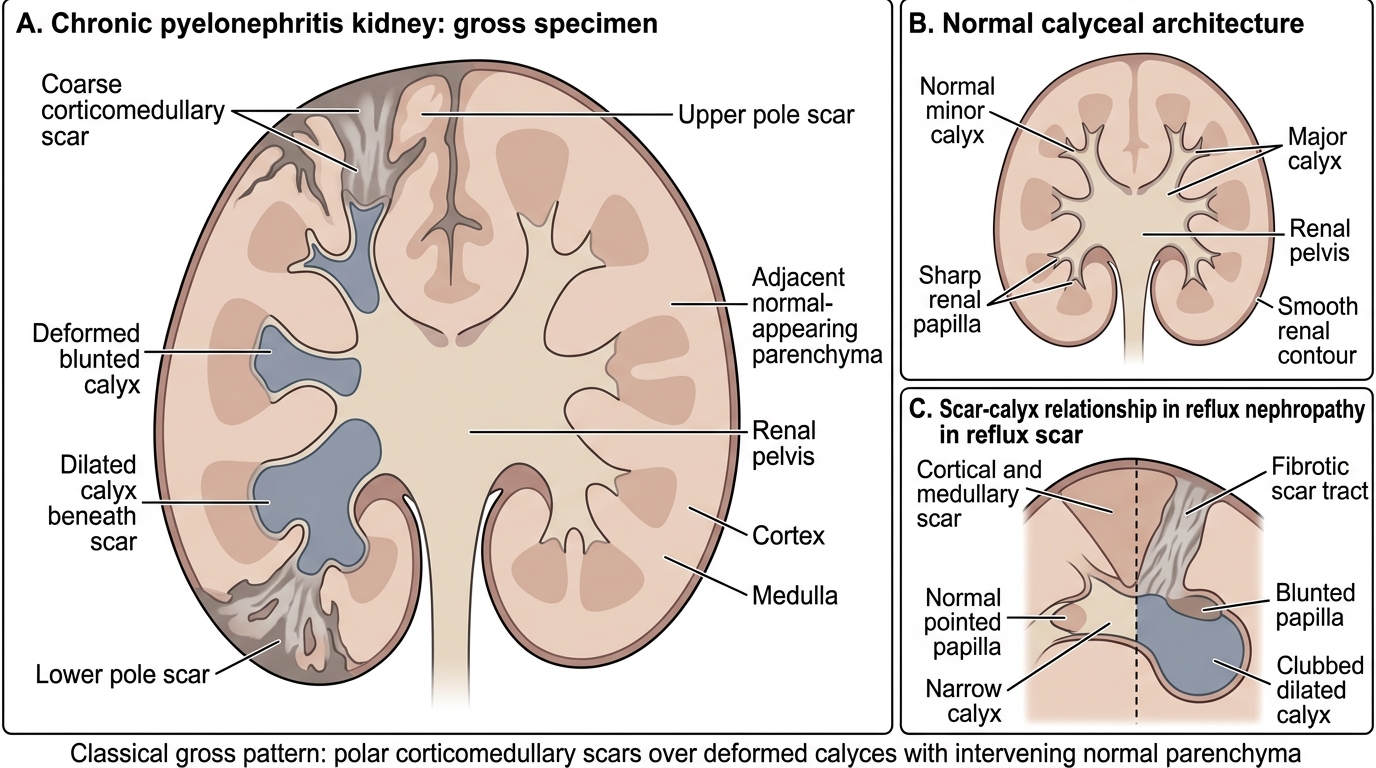
Gross Chronic Pyelonephritis: Polar Scars and Blunted Calyces
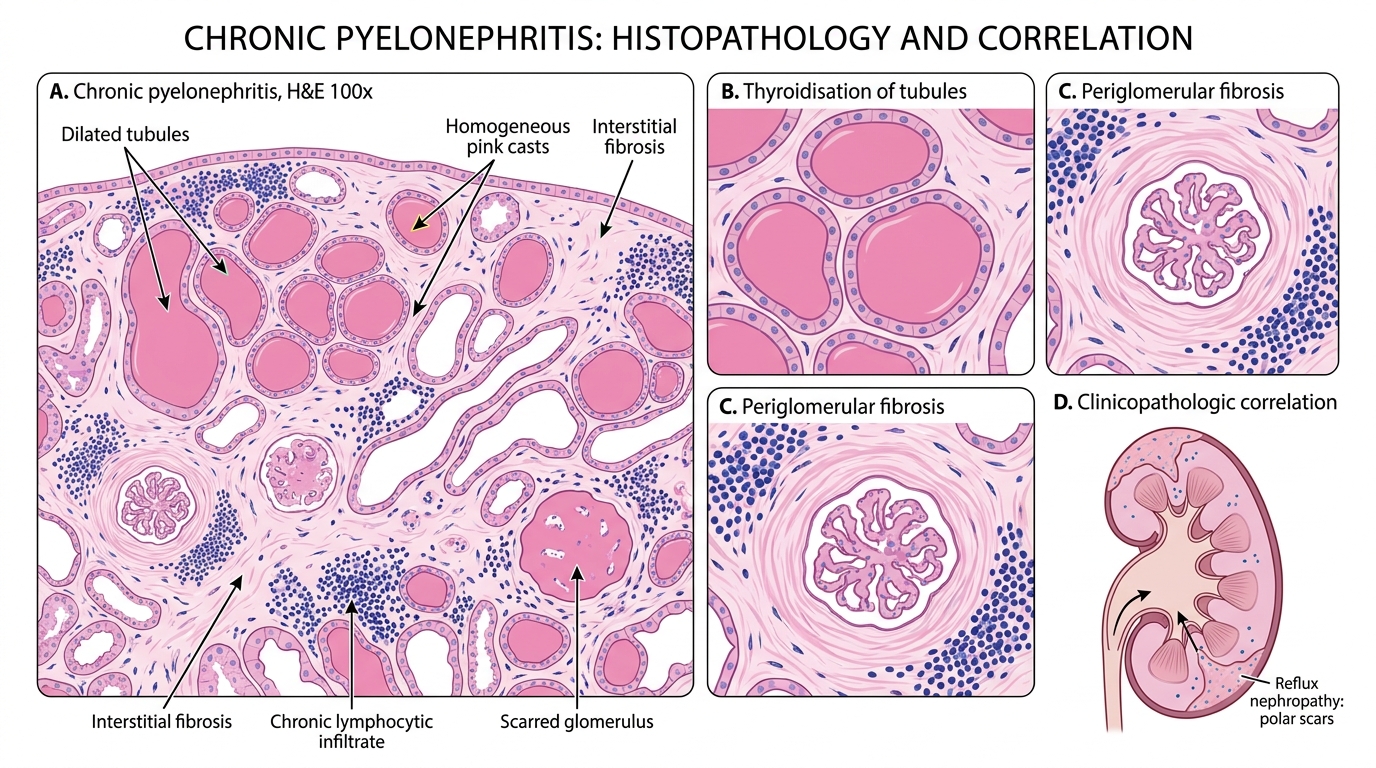
Chronic Pyelonephritis: Thyroidisation and Scarring
SELF-CHECK
A 35-year-old woman with a childhood history of recurrent UTIs presents with hypertension. Renal ultrasound shows asymmetric kidneys with focal corticomedullary scars at both poles and dilated calyces underneath the scars. Renal biopsy shows dilated tubules filled with homogeneous eosinophilic material. What is the most likely diagnosis?
A. Focal segmental glomerulosclerosis
B. Chronic obstructive pyelonephritis
C. Reflux nephropathy (chronic pyelonephritis)
D. Analgesic nephropathy with papillary necrosis
Reveal Answer
Answer: C. Reflux nephropathy (chronic pyelonephritis)
The polar distribution of coarse corticomedullary scars overlying deformed blunted calyces, combined with a history of childhood UTIs and thyroidisation on biopsy, is the classical picture of reflux nephropathy (the commonest form of chronic pyelonephritis). Obstructive CPN produces diffuse symmetric scarring, not polar. FSGS causes nephrotic syndrome without calyceal change. Analgesic nephropathy targets papillae and presents with papillary necrosis.
Drug-Induced Allergic Interstitial Nephritis
Drug-Induced Allergic Interstitial Nephritis
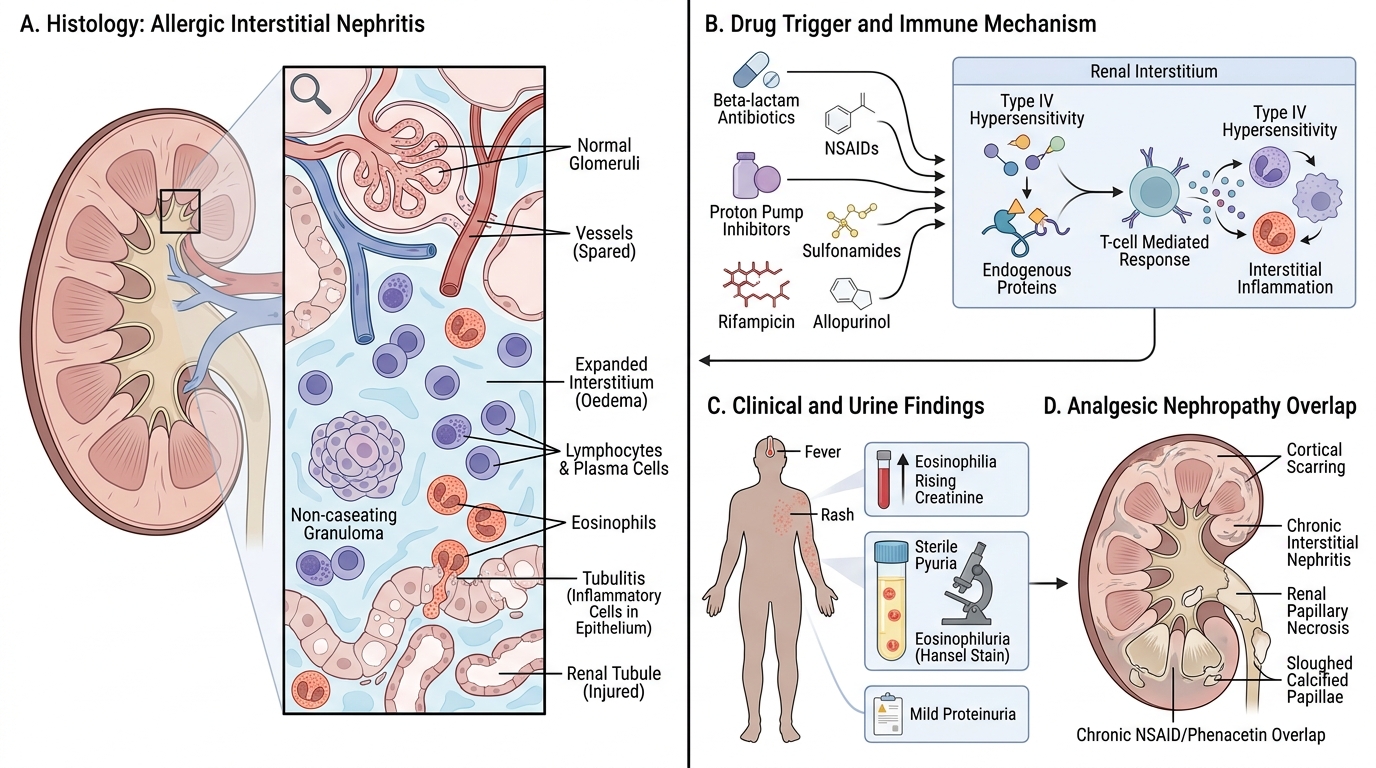
Drug-induced (allergic) interstitial nephritis represents a type-IV hypersensitivity reaction in the renal interstitium, most commonly triggered by:
- β-lactam antibiotics (methicillin — classic teaching example; ampicillin, amoxicillin)
- NSAIDs (especially with concurrent minimal change disease)
- Proton pump inhibitors (a growing cause in clinical practice)
- Sulfonamides, rifampicin, allopurinol
Onset: typically 2 weeks after exposure (range days to months); may recur on re-exposure.
Morphology:
- Diffuse interstitial oedema and infiltration by lymphocytes, plasma cells, and — characteristically — eosinophils.
- Tubulitis (inflammatory cells between tubular epithelial cells).
- Non-caseating interstitial granulomas in some cases (methicillin, sarcoidosis-like).
- Glomeruli and vessels: spared in most cases.
Clinically: fever, rash, eosinophilia (the classic allergy triad) + rising creatinine. Urine shows sterile pyuria, eosinophiluria (Hansel stain), mild proteinuria. Responds to withdrawal of offending drug ± short-course corticosteroids.
Analgesic nephropathy (mention here as a metabolic/toxic overlap): chronic NSAID/phenacetin use causes papillary necrosis + CPN-like cortical scarring. Classic triad: bilateral papillary necrosis + interstitial nephritis + cortical scarring. Sloughed papillae may calcify.
Papillary Necrosis — A Unifying Lesion
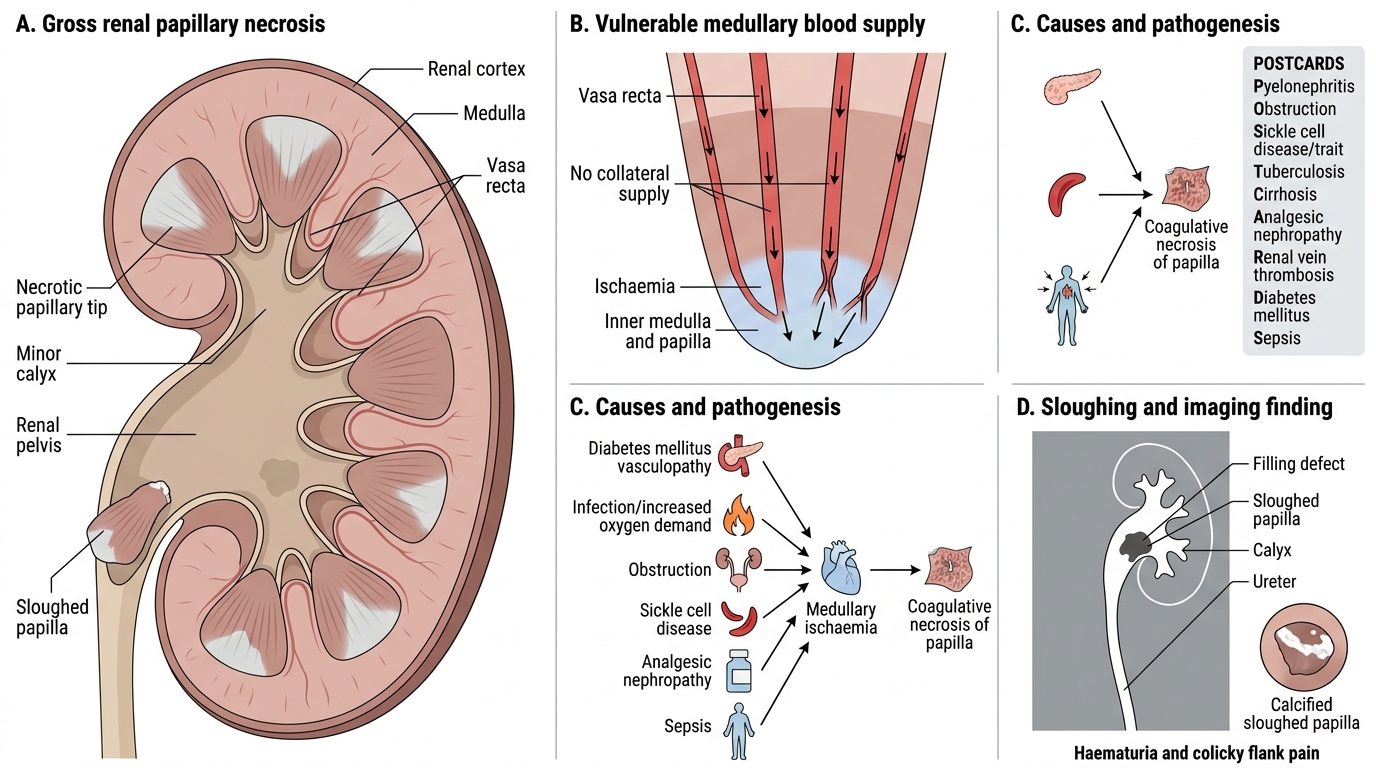
Renal Papillary Necrosis: Causes, Pathogenesis, and Clinical Consequences
Renal papillary necrosis (RPN) is ischaemic coagulative necrosis of the inner medulla and papillae. It deserves a dedicated section because it cuts across multiple tubulointerstitial diseases as a life-threatening complication.
Causes — the mnemonic POSTCARDS:
- Pyelonephritis (diabetics especially)
- Obstruction
- Sickle cell disease/trait
- Tuberculosis (less common)
- Cirrhosis
- Analgesic nephropathy (NSAIDs, phenacetin)
- Renal vein thrombosis
- Diabetes mellitus
- Sepsis
Pathogenesis: the vasa recta supplying the medulla and papillae are the only blood supply — there is no collateral. Any condition that reduces medullary blood flow (DM vasculopathy) or increases oxygen demand (infection) can trigger ischaemic papillary necrosis.
Gross: grey-white wedge-shaped area of necrosis at papillary tips; may slough and appear as a filling defect on IVU/CT urogram.
Clinical:
- Acute: colicky flank pain (sloughed papilla in ureter), haematuria, fever
- Chronic: slowly progressive CKD
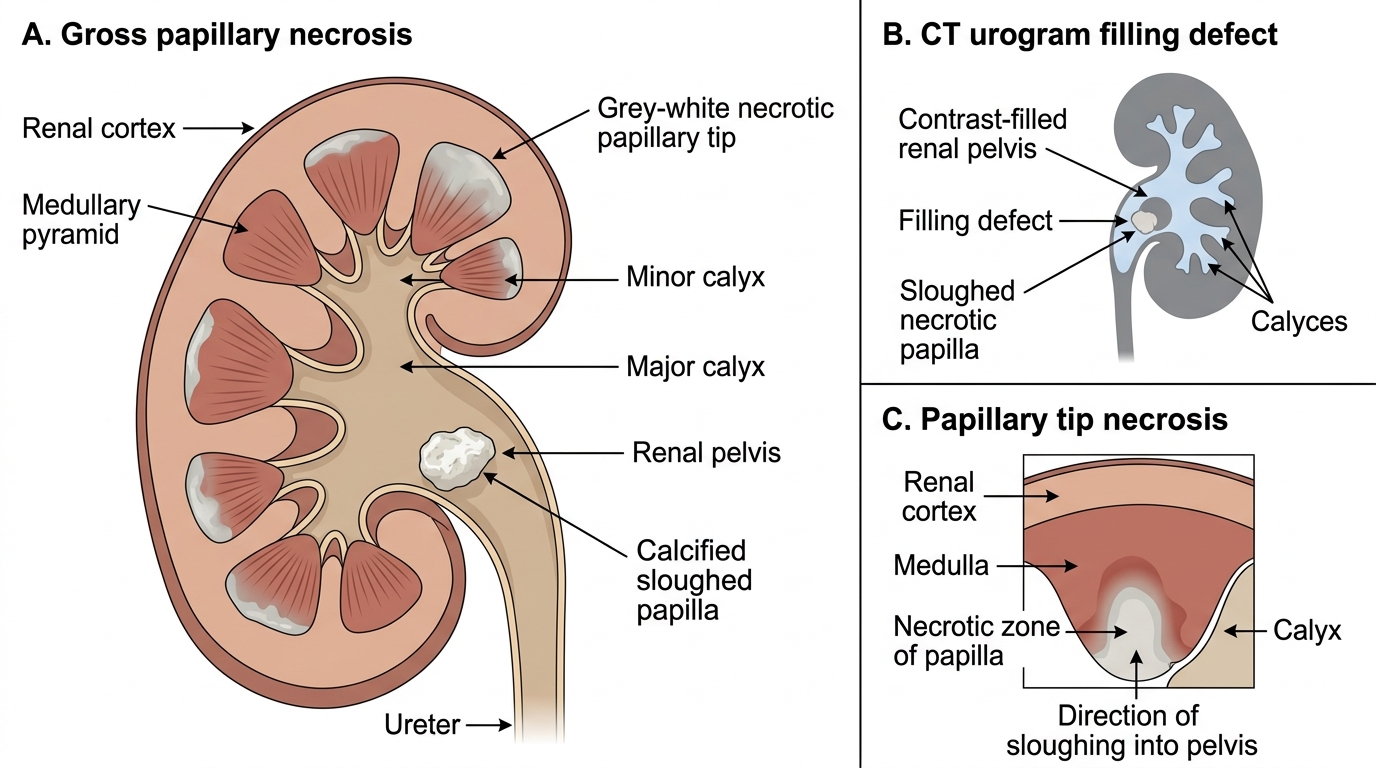
Renal Papillary Necrosis
SELF-CHECK
A 55-year-old woman with poorly controlled diabetes presents with sudden right-flank pain and haematuria. CT urogram shows a filling defect in the right renal pelvis. Which pathological mechanism best explains this finding?
A. Clot formation from glomerular haematuria due to IgA nephropathy
B. Sloughed necrotic papilla causing a filling defect in the pelvis
C. Transitional cell carcinoma arising in the renal pelvis
D. Uric acid stone formed secondary to chronic dehydration
Reveal Answer
Answer: B. Sloughed necrotic papilla causing a filling defect in the pelvis
Papillary necrosis in a diabetic patient produces ischaemic coagulative necrosis of the medullary papillae. The necrotic papillary tip detaches and passes into the renal pelvis, creating a 'ring shadow' or filling defect on imaging — classically described on IVU. The diabetes predisposes via medullary ischaemia (vasculopathy) and impaired neutrophil function (coexistent pyelonephritis). IgA nephropathy causes haematuria but not a filling defect; TCC and uric acid stones are possible differentials but the diabetic context strongly favours papillary necrosis.
Distinguishing Features at a Glance
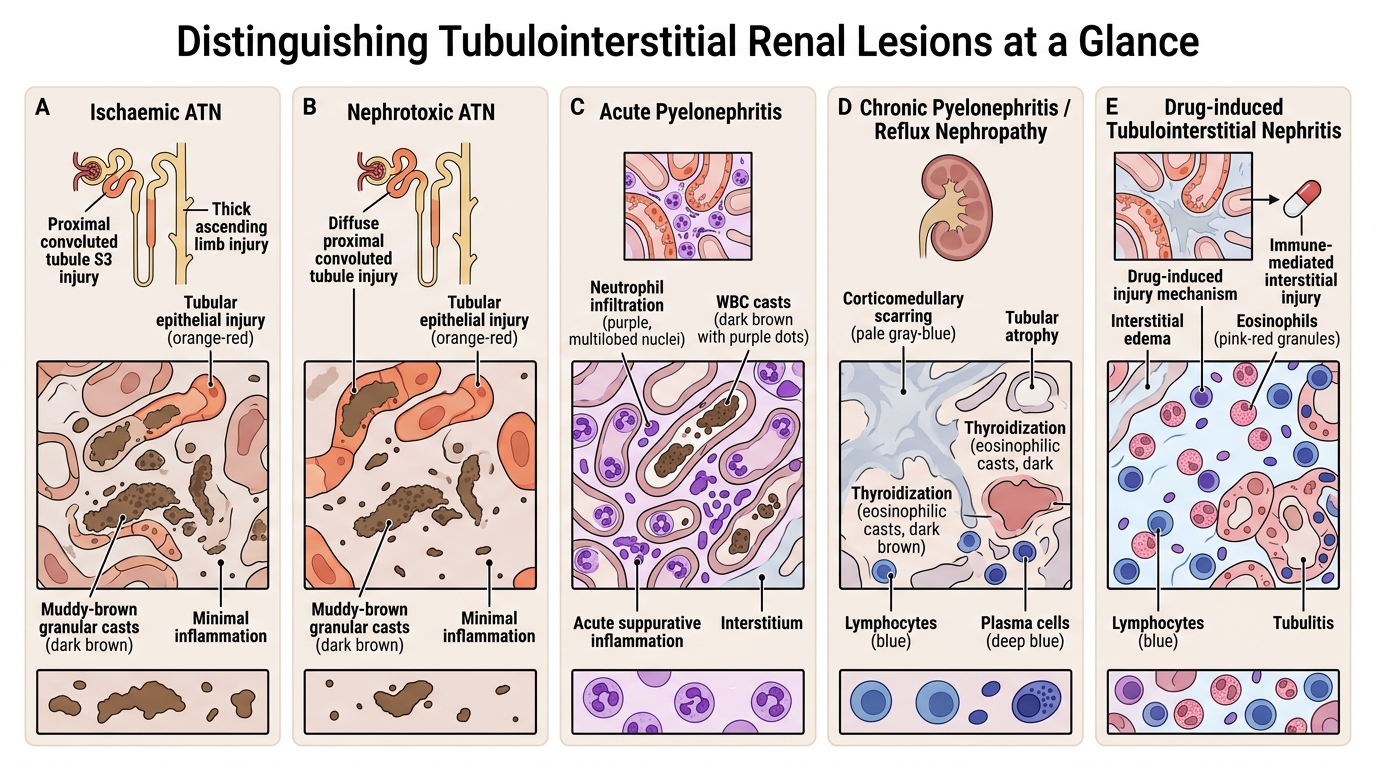
Distinguishing Renal Tubulointerstitial Lesions
This comparison table consolidates the key discriminating features examined most often in MBBS theory and OSPE:
| Feature | Ischaemic ATN | Nephrotoxic ATN | Acute PN | Chronic PN / Reflux | Drug-induced TIN |
|---|---|---|---|---|---|
| Primary injury site | PCT (S3) + thick asc. limb | Entire PCT | Tubules + interstitium | Corticomedullary | Interstitium |
| Inflammatory cells | None significant | None significant | Neutrophils | Lymphocytes + PC | Eosinophils + lymphocytes |
| Casts | Granular (muddy-brown) | Granular (muddy-brown) | WBC casts | Colloid / hyaline | Sterile pyuria (no casts) |
| Basement membrane | Ruptured (tubulorrhexis) | Intact | Intact | Thickened/fibrosed | Intact |
| Reversibility | Yes (if insult removed) | Yes (if insult removed) | Yes (antibiotics) | Partial (fibrosis) | Yes (withdraw drug ± steroids) |
| Gross kidney | Normal/slightly swollen | Normal/slightly swollen | Enlarged, abscesses | Small, scarred | Normal/slightly swollen |
| Key hallmark | Patchy tubular necrosis | Diffuse PCT necrosis | Microabscesses + WBC casts | Thyroidisation + calyceal blunting | Eosinophilic interstitial infiltrate |