Page 5 of 27
PA27.{11,15} | Vascular Diseases & Thrombotic Microangiopathies — SDL Guide
Learning Objectives
- Classify the vascular diseases of the kidney and outline the role of hypertension in benign and malignant nephrosclerosis.
- Describe the pathological lesions of benign nephrosclerosis (hyaline arteriolosclerosis, fibroelastic hyperplasia) and their gross and microscopic consequences.
- Distinguish the morphological hallmarks of malignant hypertension — fibrinoid necrosis, hyperplastic onion-skin arteriolitis, and the flea-bitten kidney.
- Explain the mechanism of renovascular hypertension in renal artery stenosis and differentiate atherosclerotic from fibromuscular dysplasia causes.
- Define thrombotic microangiopathy (TMA) and describe the shared pathological substrate of endothelial injury, microthrombi, MAHA, and thrombocytopenia.
- Compare and contrast HUS (typical Shiga-toxin vs atypical complement-mediated) and TTP (ADAMTS13 deficiency) using clinical, laboratory, and morphological features.
- Recognise the renal lesions of DIC, scleroderma renal crisis, cortical necrosis, and renal infarction.
INSTRUCTIONS
The kidney sits at the crossroads of systemic haemodynamics and microvascular biology. Sustained hypertension remodels renal vessels across a spectrum — from the silent scarring of benign nephrosclerosis to the catastrophic fibrinoid necrosis of malignant hypertension. At the other extreme, the thrombotic microangiopathies demonstrate how a single pathological theme — endothelial injury with microvascular thrombosis — can arise from a toxin (HUS), an enzyme deficiency (TTP), complement dysregulation, or immune activation, yet converge on the same triad of haemolytic anaemia, thrombocytopenia, and acute kidney injury. Mastering this module gives you a unifying vascular lens for interpreting renal biopsies, clinical syndromes, and laboratory results that will recur throughout medicine.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 20 (The Kidney) (textbook)
- Harsh Mohan: Textbook of Pathology, 8th ed., Ch 22 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man with a 15-year history of poorly controlled hypertension is found on autopsy to have bilaterally shrunken kidneys with finely granular surfaces. His 32-year-old niece is admitted with sudden headache, oliguria, microangiopathic haemolytic anaemia, and a platelet count of 18,000/μL — three days after a bloody diarrhoeal illness. Same organ, utterly different vascular catastrophes. By the end of this module, you will read both scenarios from the morphology up.
WHY THIS MATTERS
Hypertension affects 30% of Indian adults. Malignant hypertension — though less common — remains a preventable cause of acute renal failure. Thrombotic microangiopathies are under-recognised emergencies where early diagnosis (blood film, ADAMTS13 assay, Shiga-toxin PCR) is life-saving. In postgraduate entrance examinations, the onion-skin arteriolitis of malignant hypertension and the HUS/TTP distinction are perennially high-yield topics.
RECALL
Before proceeding, consolidate your Year-1 foundations:
- Arterioles — structure: intima (endothelium + IEL), media (1-2 smooth muscle layers), adventitia.
- Hyaline change in vessels — amorphous eosinophilic protein deposition (plasma protein insudation + basement membrane thickening) seen in diabetes and age.
- Renin-angiotensin-aldosterone system (RAAS) — juxtaglomerular cells release renin → angiotensinogen → Ang I → ACE → Ang II → vasoconstriction + aldosterone → sodium retention → raised BP.
- Haemolytic anaemia — extravascular (splenomegaly, elevated indirect bilirubin) vs intravascular (haemoglobinaemia, haemoglobinuria, low haptoglobin).
- Schistocytes — fragmented red blood cells produced when RBCs are sheared by fibrin strands in small vessels.
If any of these are unclear, revisit them before continuing.
Overview: Vascular Diseases of the Kidney
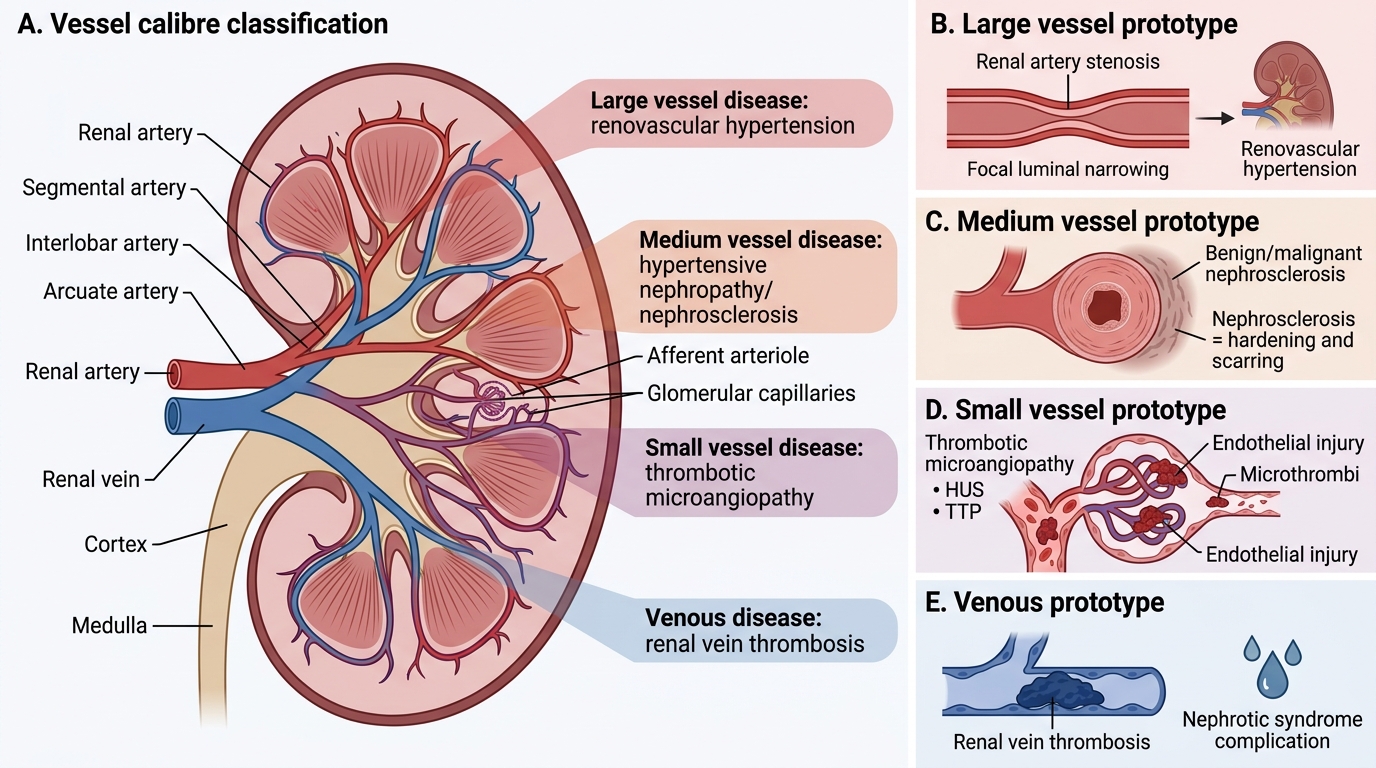
Vascular Diseases of the Kidney by Vessel Calibre
Vascular diseases of the kidney can be classified by the calibre of vessels affected:
| Vessel level | Disease | Prototype |
|---|---|---|
| Large (renal artery) | Renovascular hypertension | Renal artery stenosis |
| Medium (interlobular arteries) | Hypertensive nephropathy | Benign/malignant nephrosclerosis |
| Small (arterioles, glomerular capillaries) | Thrombotic microangiopathy | HUS, TTP |
| Renal vein | Renal vein thrombosis | Nephrotic syndrome complication |
Nephrosclerosis refers to the hardening and scarring of the kidney as a consequence of vascular disease. Two distinct forms are recognised based on the severity and acuity of hypertension: benign and malignant (accelerated) nephrosclerosis.
PA27.11 covers both hypertensive forms and renovascular disease; PA27.15 covers thrombotic angiopathies.
Benign Nephrosclerosis: Pathogenesis and Morphology
Benign Nephrosclerosis: Pathogenesis and Morphology
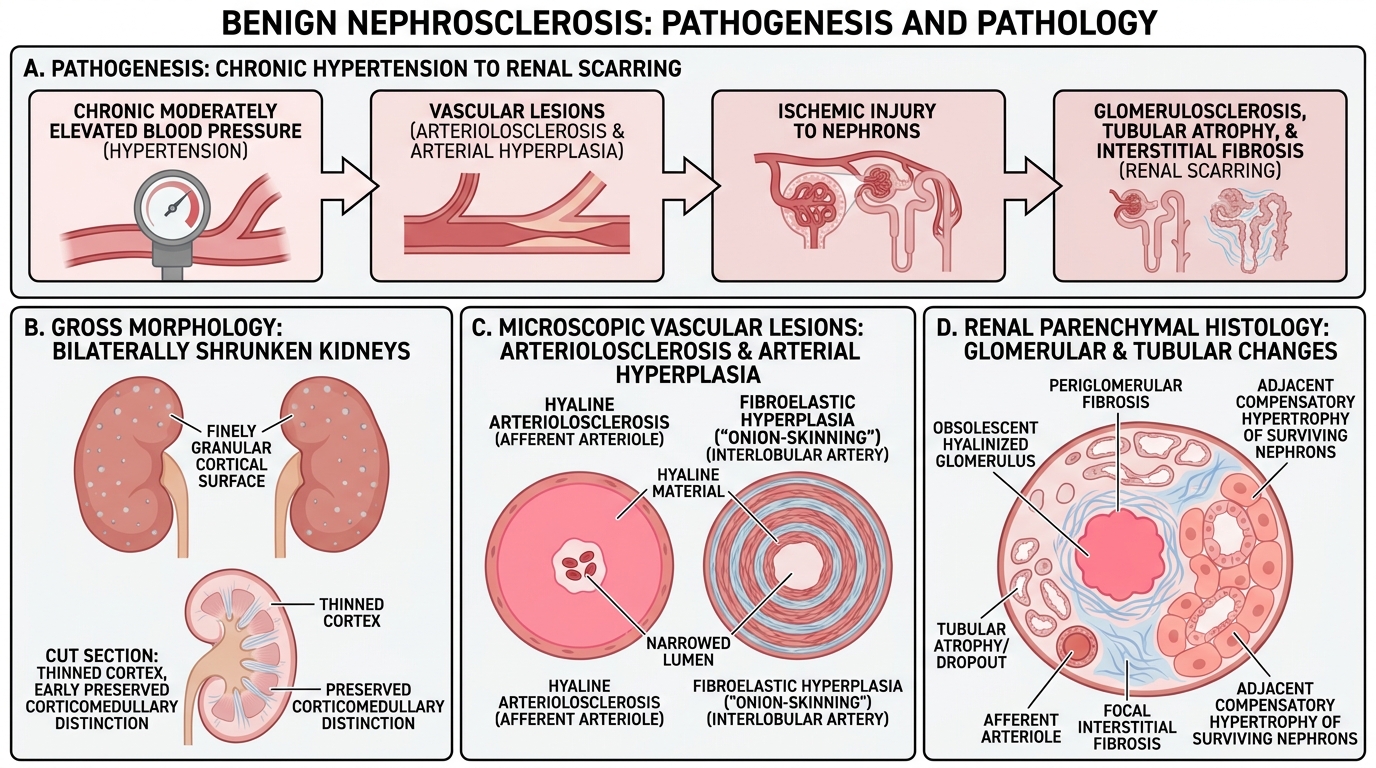
Benign nephrosclerosis is the renal manifestation of long-standing, moderately elevated blood pressure. It is the commonest form of hypertensive renal disease.
Pathogenesis:
Chronic pressure overload → two sequential arteriolar lesions:
1. Hyaline arteriolosclerosis — plasma proteins insudated into the arteriolar wall; PAS-positive homogeneous pink material replaces the media; smooth muscle cells are lost. Seen in afferent arterioles.
2. Fibroelastic hyperplasia (intimal thickening) — smooth muscle cells and collagen proliferate in the intima of interlobular arteries; lumen narrows progressively.
Both lesions narrow the lumen → patchy ischaemia → glomerular ischaemia → periglomerular fibrosis → tubular atrophy → interstitial fibrosis.
Gross morphology:
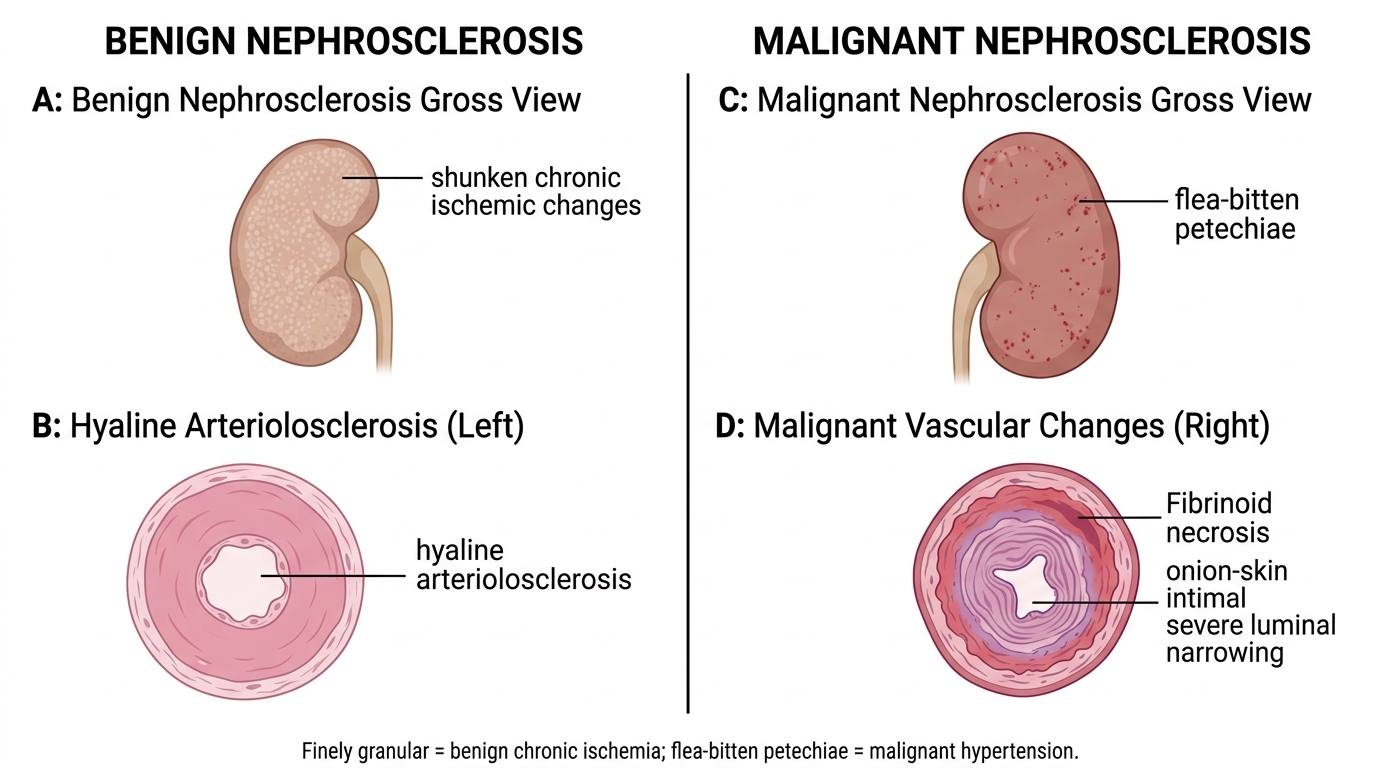
• Bilateral shrunken kidneys (each ~110-130 g vs normal 150 g)
• Finely granular cortical surface — each granule = a surviving nephron tuft surrounded by fibrosis; depressed areas = scarred, ischaemic nephrons
• Cortex thinned; corticomedullary distinction preserved early
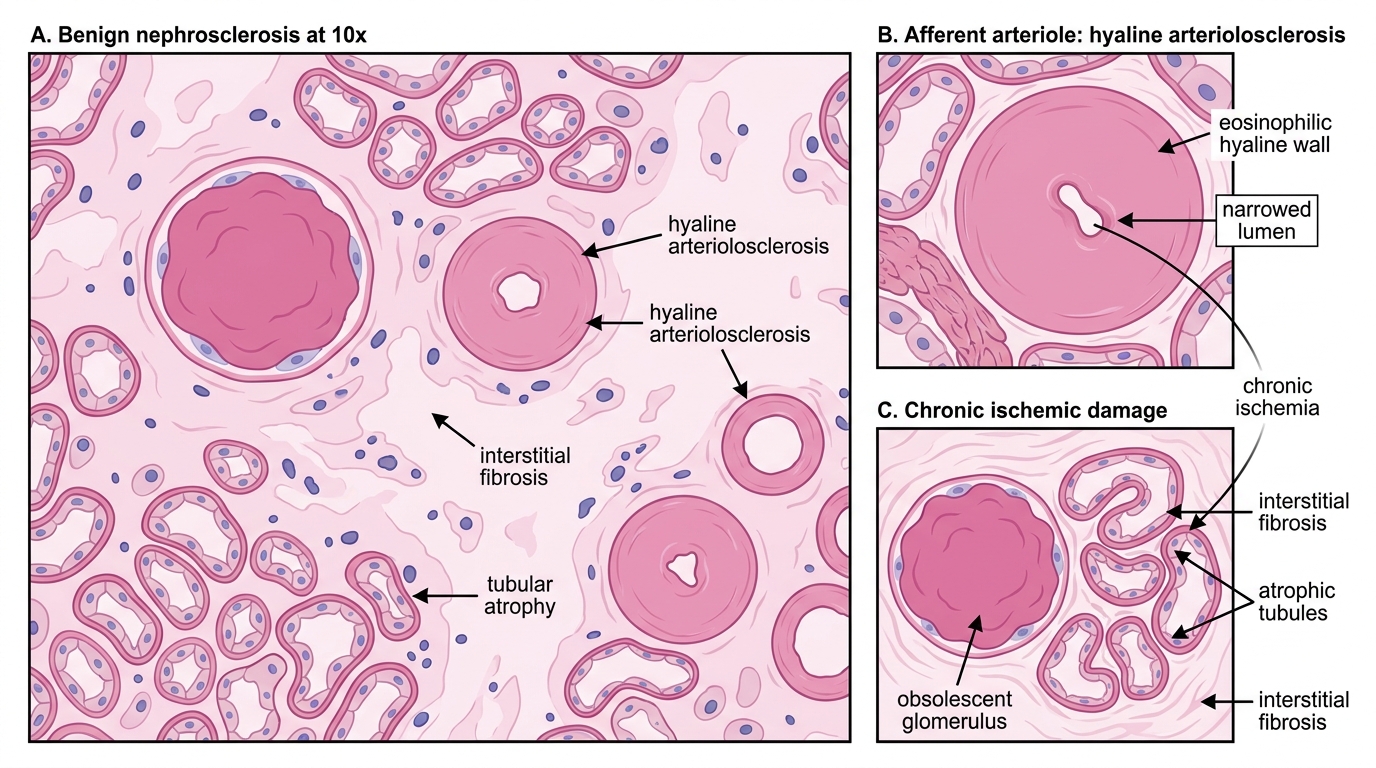
Microscopic:
• Hyalinised afferent arterioles (eosinophilic, thickened wall, slit-like lumen)
• Obsolescent (hyalinised) glomeruli — ghost glomeruli with washed-out appearance
• Tubular atrophy and dropout
• Focal interstitial fibrosis
• Surviving nephrons undergo compensatory hypertrophy (large tubules, enlarged glomeruli)
Clinical: proteinuria is mild; renal failure is slow (decades); BP control slows progression.
Benign Nephrosclerosis: Microscopic Features
SELF-CHECK
Which microscopic lesion in benign nephrosclerosis directly explains the finely granular surface seen on gross examination?
A. Fibrinoid necrosis of arterioles causing acute haemorrhage
B. Deposition of immune complexes in glomerular capillary walls
C. Hyperplastic onion-skin intimal thickening
D. Focal ischaemic scarring alternating with surviving hypertrophied nephrons
Reveal Answer
Answer: D. Focal ischaemic scarring alternating with surviving hypertrophied nephrons
The finely granular surface of benign nephrosclerosis reflects patches of ischaemic scar (depressed granules) alternating with relatively preserved, compensatorily hypertrophied surviving nephrons (raised granules). The vessel lesions (hyaline arteriolosclerosis, fibroelastic hyperplasia) cause the ischaemia, but it is this focal pattern of dropout-and-survival that creates the macroscopic granularity. Fibrinoid necrosis and onion-skin changes are features of malignant hypertension.
Malignant Hypertension / Accelerated Nephrosclerosis
Malignant Hypertension: Accelerated Nephrosclerosis
Malignant hypertension (diastolic BP >120 mmHg, rising acutely, with end-organ damage) produces a distinct and rapidly destructive renal syndrome — malignant nephrosclerosis (also called accelerated nephrosclerosis).
Key vessel lesions (the two diagnostic hallmarks):
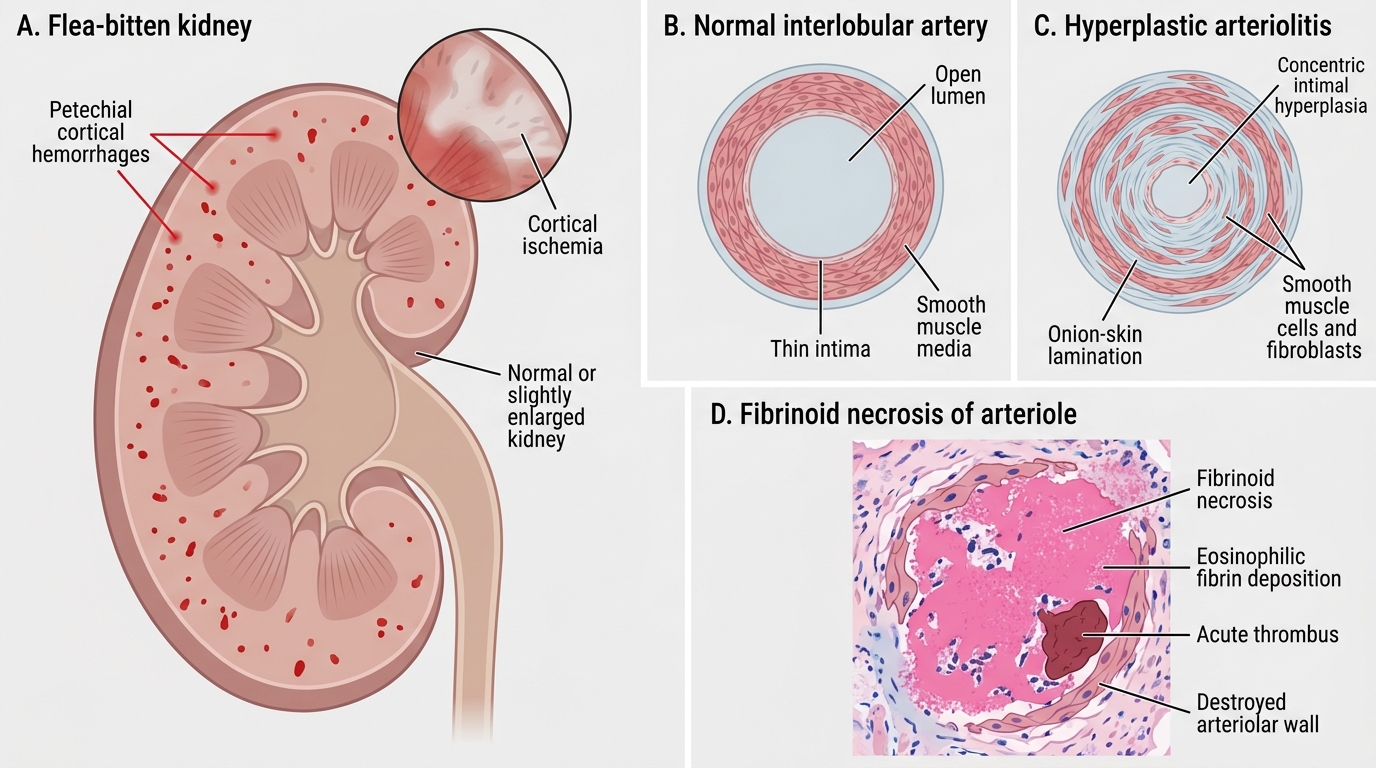
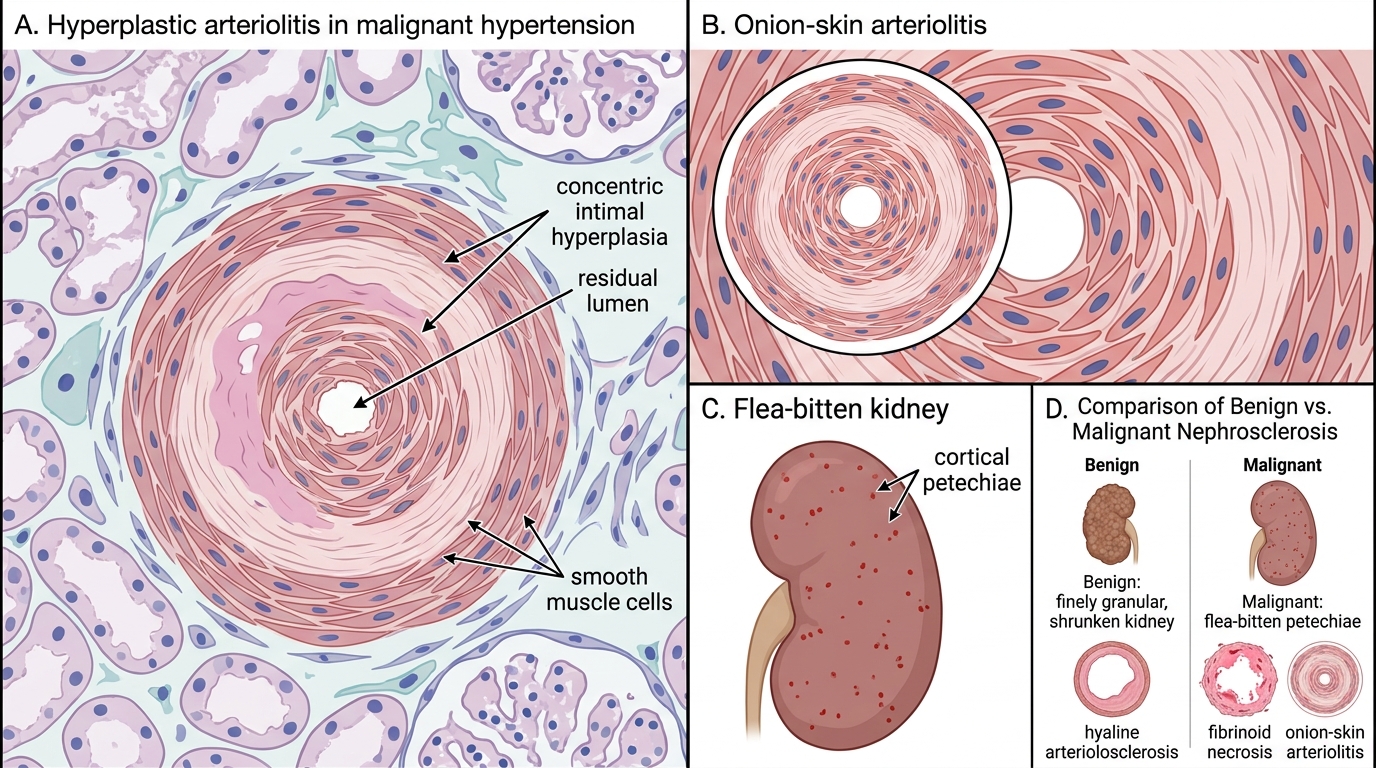
- Fibrinoid necrosis of arterioles — the acutely injured arteriole undergoes necrosis; plasma proteins (including fibrin) flood the wall → intensely eosinophilic, granular, smudgy appearance on H&E. The entire wall is destroyed. Associated with acute thrombosis → sudden cortical ischaemia.
- Hyperplastic arteriolitis (onion-skin lesion) — in interlobular arteries, smooth muscle cells and fibroblasts proliferate concentrically in the intima; each successive layer of cells and collagen resembles the layers of an onion in cross-section. Lumen is severely reduced. This is the classic histological hallmark of malignant hypertension.
Malignant Hypertension: Hyperplastic Arteriolitis and Flea-Bitten Kidney
Gross morphology — the flea-bitten kidney:
• Kidneys may be normal size or slightly enlarged (acute, not yet atrophic)
• Multiple petechial haemorrhages on the cortical surface → flea-bitten appearance (haemorrhages from necrotic arterioles and damaged glomerular capillaries)
Microscopic:
• Fibrinoid necrosis of afferent arterioles
• Onion-skin arteriolitis of interlobular arteries
• Necrotising glomerulitis — mesangiolysis, capillary wall necrosis, crescent formation (in severe cases)
• Interstitial haemorrhage
Clinical: acute renal failure, haematuria, red cell casts, heavy proteinuria, hypertensive encephalopathy, papilloedema. Medical emergency.
Benign vs Malignant Nephrosclerosis
CLINICAL PEARL
The flea-bitten kidney is not finely granular — this distinction catches candidates out. Benign nephrosclerosis = shrunken, finely granular (chronic ischaemia, cortical loss). Malignant hypertension = petechial haemorrhages on a relatively normal-sized kidney (acute arteriolar blowouts). The granules in benign disease are structural (hypertrophied nephrons); the haemorrhages in malignant disease are vascular (fibrinoid necrosis). Get these two gross appearances locked before the exam.