Page 23 of 32
PA25.7 | Lung Disease & Tumour Morphology — Practical — SDL Guide
Learning Objectives
- Identify and describe the gross and microscopic features of lobar pneumonia and bronchopneumonia
- Recognise the morphological stages of tuberculosis including caseating granuloma, Ghon complex, and cavitation
- Describe the gross and microscopic appearances of emphysema and major pneumoconioses
- Identify and classify primary lung carcinomas — SCLC, squamous cell, adenocarcinoma — by their histological hallmarks
- Apply a systematic gross-to-micro reading strategy to unknown respiratory specimens
INSTRUCTIONS
Lung practical specimens span the full spectrum of pulmonary disease — infection, obstruction, environmental injury, and neoplasia. Pattern recognition at the bench depends on reading gross architecture first, then zooming into the microscopic signature. This module walks you through each category with the same systematic framework you will use in the histopathology practical hall and in clinical case discussions. Mastering these patterns now will pay dividends in medicine, surgery, and oncology postings.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 15 (The Lung) (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 16 (Pathology of Lung) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are handed a glass slide and told: 'Tell me what you see.' The section shows sheets of small hyperchromatic cells with virtually no cytoplasm, nuclei moulding against each other, and scattered crush artefact. Is this infection? Inflammation? Or one of the most aggressive lung cancers? The answer lives in pattern — gross shape, microscopic architecture, cellular detail. This module gives you the reading framework to crack every lung specimen in 60 seconds.
WHY THIS MATTERS
Lung pathology is one of the highest-yield practical topics in Year-2 PA examinations. Spotters routinely include pneumonia, TB, emphysema, and carcinoma. Clinicians who trained in pathology labs are measurably faster at interpreting chest CT reports and histopathology results. The patterns you learn today translate directly into understanding radiological terms like 'consolidation', 'cavitation', and 'mass lesion' that you will encounter daily on wards.
RECALL
Before we start, activate what you already know:
- What are the two arms of the innate immune response to bacterial infection — cellular and humoral?
- Describe a granuloma in one sentence from your Year-1 general pathology.
- Name three cell types in normal alveolar walls (you covered lung histology in AN).
- What is the difference between a consolidation and a cavity on a chest X-ray?
Keep these answers in mind — they are the scaffolding for every block that follows.
The Systematic Reading Framework
Systematic Reading Framework for Lung Specimens
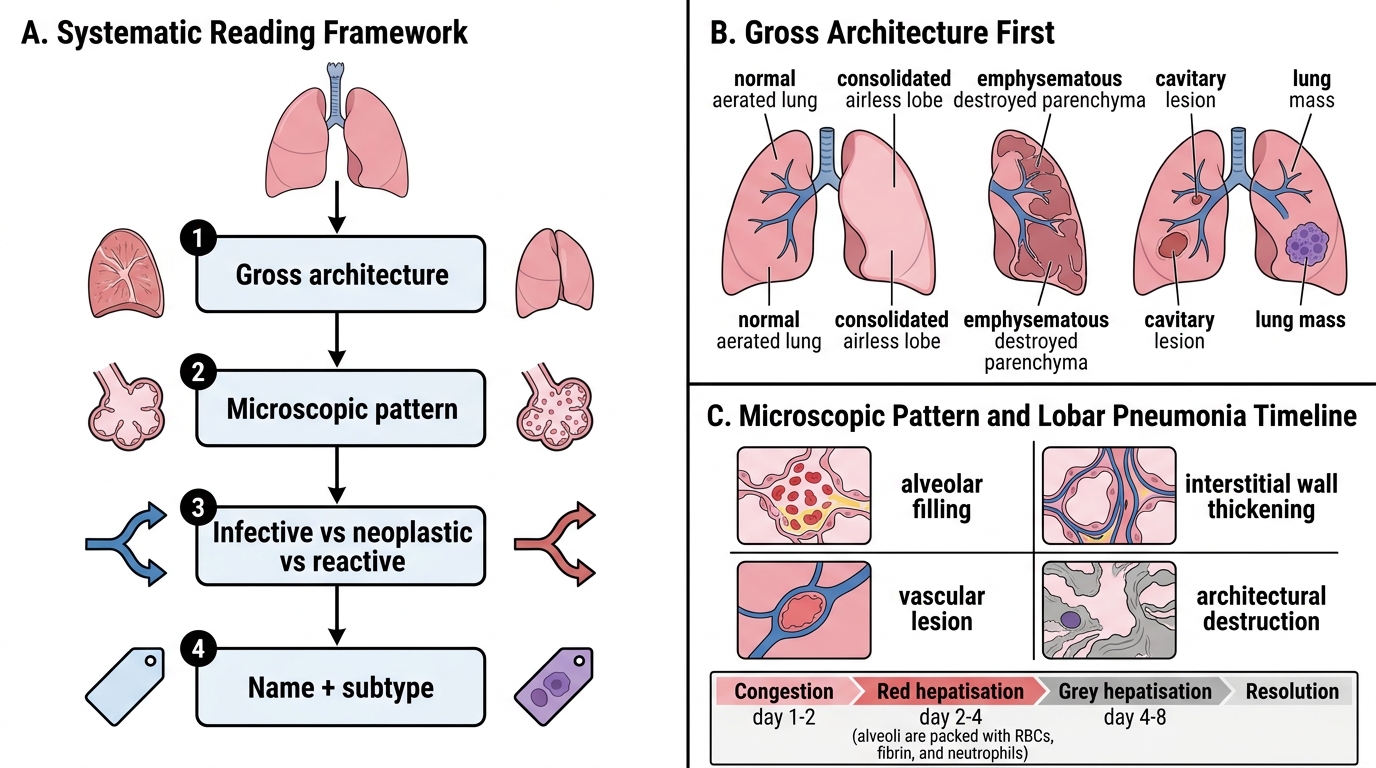
Every lung specimen — biopsy, resection, or autopsy lobe — should be read in four steps:
- Gross architecture first — Is the parenchyma airless (consolidation), destroyed (emphysema), cavitated, or occupied by a mass?
- Microscopic pattern — Is the abnormality alveolar (filling), interstitial (wall thickening), vascular, or architectural destruction?
- Infective vs. neoplastic vs. reactive — Inflammation implies exudate + intact architecture; tumour implies loss of architecture + abnormal cytology.
- Name + subtype — Combine gross + micro + context to assign a specific diagnosis.
This four-step approach works for every category covered in this module. We will apply it explicitly to each condition.
Pneumonia — Lobar vs. Bronchopneumonia
Lobar Pneumonia vs Bronchopneumonia
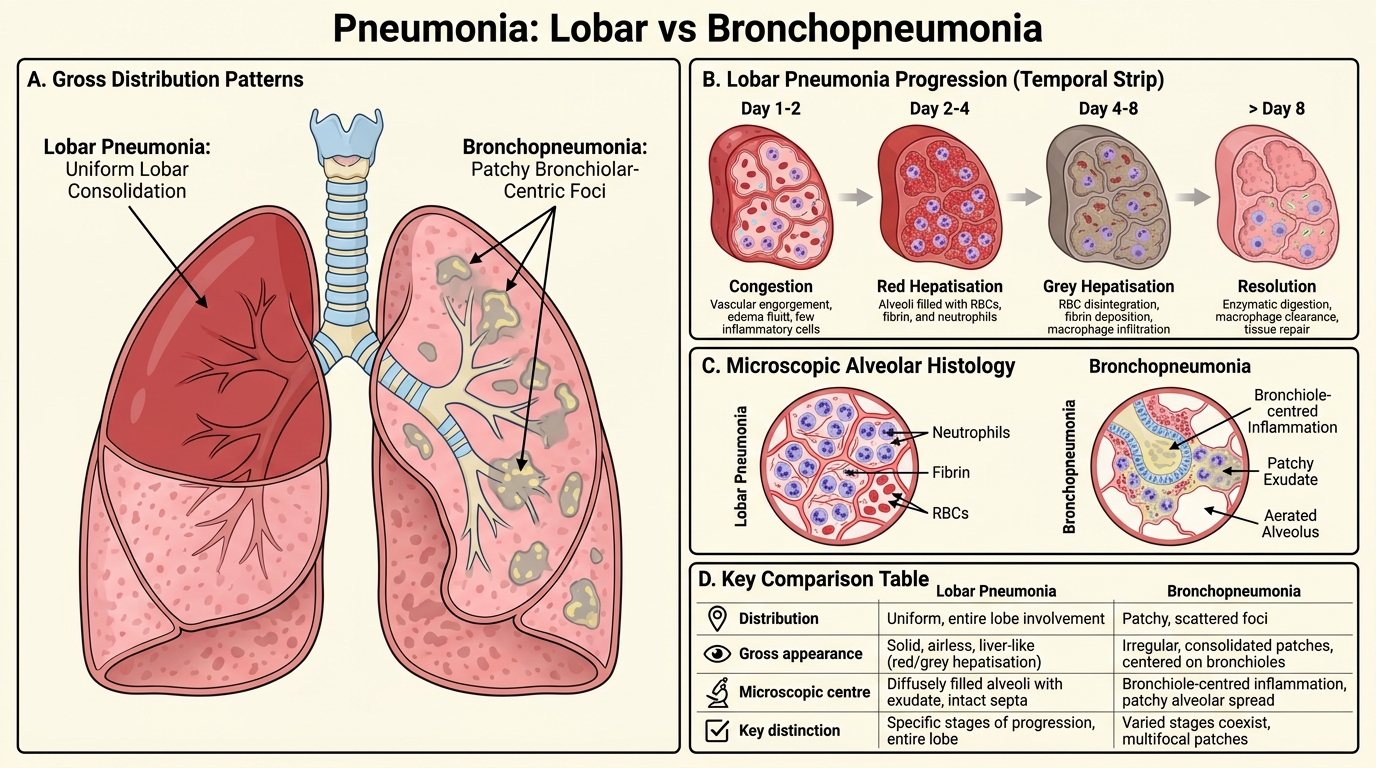
Lobar pneumonia is a classic bacterial consolidation (usually Streptococcus pneumoniae) affecting an entire lobe or segment in a predictable temporal sequence:
| Stage | Gross | Microscopic |
|---|---|---|
| Congestion (day 1–2) | Heavy, red, boggy | Vascular engorgement, serous exudate |
| Red hepatisation (day 2–4) | Liver-like, red, airless | Alveoli packed with RBCs + fibrin + early neutrophils |
| Grey hepatisation (day 4–8) | Grey, dry, firm | RBCs lysed; neutrophil + fibrin mesh; no airspace |
| Resolution | Returns to spongy | Macrophage clearance; architecture restored |
The defining microscopic feature is alveolar neutrophil exudate filling air spaces with intact alveolar walls — a key distinguishing feature from destructive processes.
Bronchopneumonia (lobular pneumonia) is a patchy, multifocal consolidation centred on bronchioles and adjacent alveoli. Gross: multiple grey-yellow foci 1–3 cm scattered across dependent lobes. Micro: acute bronchiolitis + surrounding alveolar neutrophil exudate, but with intervening aerated lung — the patchiness is the hallmark.
KEY DISTINCTION: Lobar = whole lobe airless, fibrinous exudate, preserved architecture. Bronchopneumonia = focal, purulent, centred on airways.
SELF-CHECK
A 65-year-old man has a right lower lobe that is uniformly airless, liver-like in consistency, and grey on cut section. Microscopically, alveoli are packed with neutrophils and fibrin mesh with intact alveolar walls. What stage of lobar pneumonia does this represent?
A. Congestion
B. Red hepatisation
C. Grey hepatisation
D. Resolution
Reveal Answer
Answer: C. Grey hepatisation
Grey hepatisation (days 4–8) shows grey-white, firm, airless lung on gross. Microscopically the alveoli are filled with neutrophils, fibrin, and cellular debris, while RBCs have been lysed — hence the grey colour. Red hepatisation is earlier (days 2–4) and shows RBC-rich exudate giving a red liver-like appearance.
Tuberculosis — Caseating Granuloma to Cavity
Tuberculosis: Caseating Granuloma to Cavity
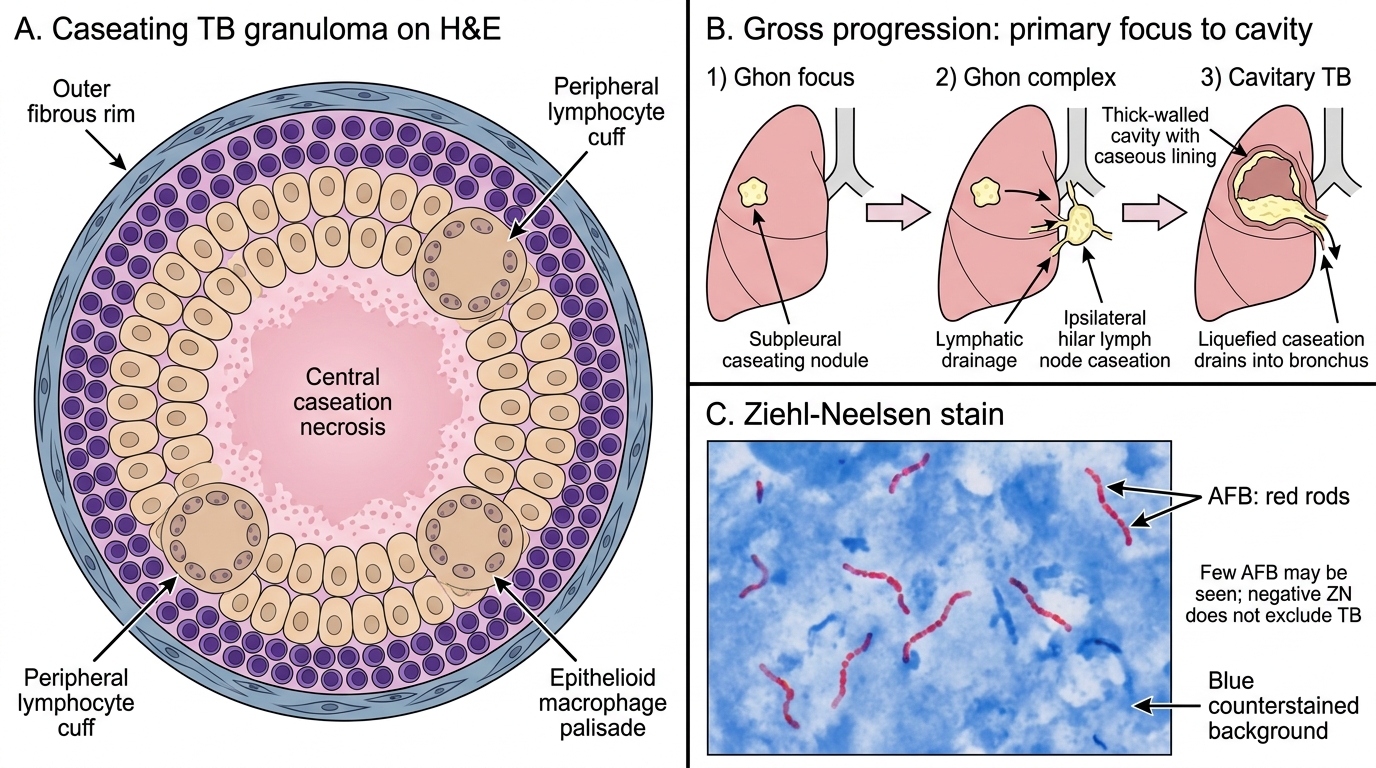
Tuberculosis produces one of pathology's most recognisable microscopic signatures: the caseating granuloma.
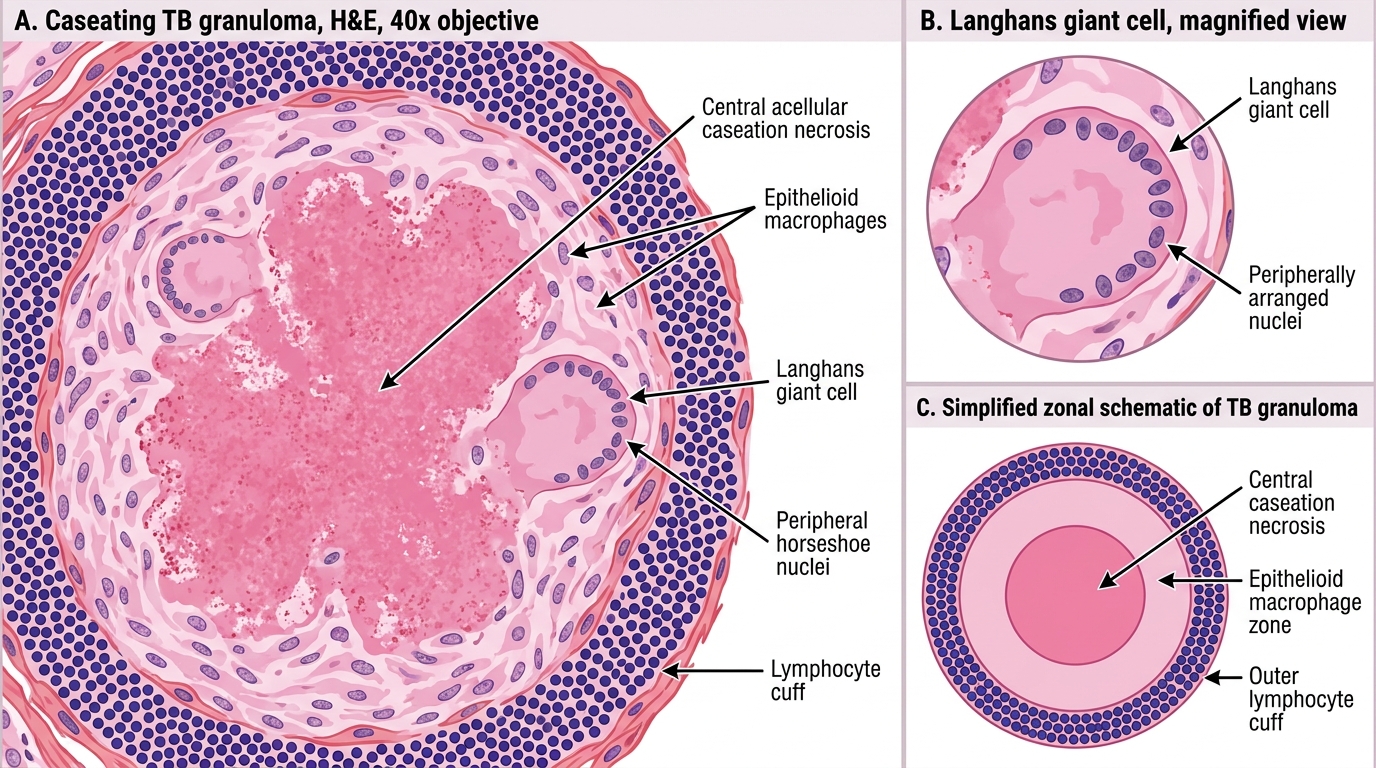
Microscopic anatomy of the TB granuloma:
• Central caseation necrosis — granular, eosinophilic, acellular material (ghost cells, lipid from mycobacterial wall). Looks like cottage cheese on gross.
• Surrounding epithelioid macrophages — plump, pale, kidney-shaped nuclei arranged in a palisade.
• Langhans giant cells — large multinucleated cells (nuclei arranged in a horseshoe or peripheral wreath) formed by macrophage fusion. Langhans ≠ Langerhans (islets). Hallmark of TB granuloma.
• Peripheral lymphocyte cuff — chronic inflammatory infiltrate.
• Outer fibrous rim — attempted walling off.
Gross progression:
1. Ghon focus — subpleural parenchymal caseating nodule (usually right upper lobe).
2. Ghon complex — Ghon focus + ipsilateral hilar lymph node caseation (primary TB).
3. Cavitary TB — post-primary, upper lobe; caseation liquefies and drains into bronchus leaving a thick-walled cavity with caseous lining. Cavity walls harbour actively replicating bacilli.
Special stain — ZN (Ziehl-Neelsen): AFB (acid-fast bacilli) stain red against blue background. Mycobacterium tuberculosis is the archetype AFB. Important: TB granulomas may have few AFB; a negative ZN does not exclude TB.
Caseating Tuberculous Granuloma on H&E
SELF-CHECK
On a ZN-stained section of lung, you see red-staining bacilli within an area of granulomatous inflammation. The finding is most consistent with:
A. Streptococcus pneumoniae — ZN-positive cocci
B. Fungal hyphae identified by ZN carbol-fuchsin
C. Haemosiderin-laden macrophages staining red on ZN
D. Acid-fast bacilli, consistent with mycobacterial infection
Reveal Answer
Answer: D. Acid-fast bacilli, consistent with mycobacterial infection
ZN stain (Ziehl-Neelsen) uses hot carbol-fuchsin; acid-fast organisms (mycobacteria) retain the stain and appear red/pink against a blue or green counterstain. Bacteria like Streptococcus are Gram-positive but not acid-fast, so they do not stain red on ZN. Fungi are identified by PAS or GMS stains. Haemosiderin appears golden-brown on H&E and does not stain red on ZN.