Page 24 of 32
PA25.7 | Lung Disease & Tumour Morphology — Practical — SDL Guide (Part 2)
Emphysema — Airspace Destruction
Emphysema: Airspace Destruction
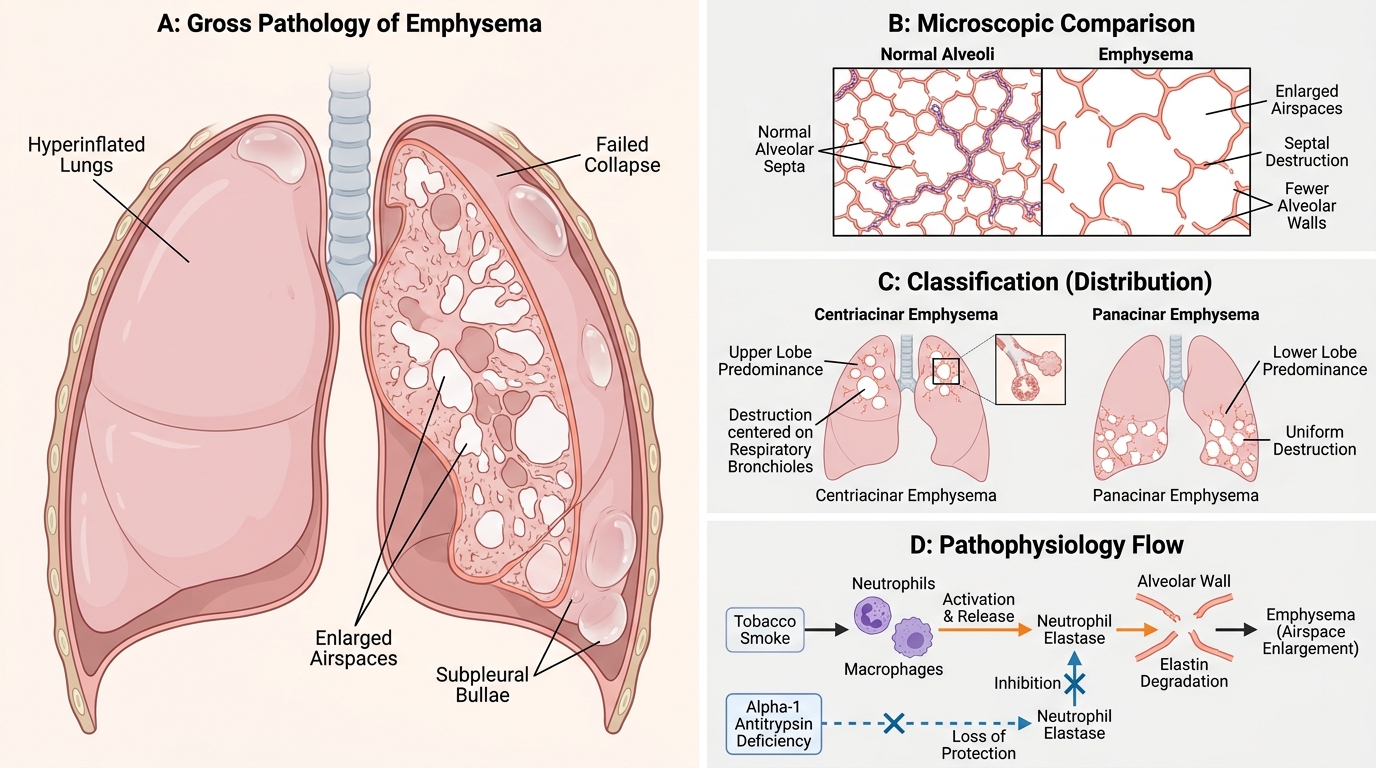
Emphysema is a permanent, abnormal enlargement of airspaces distal to the terminal bronchiole with destruction of alveolar walls — the defining word is destruction, not just dilation.
Gross appearances:
• Hyperinflated, voluminous lungs that do not collapse on opening the chest.
• Cut surface shows enlarged, irregular airspaces; bullae (emphysematous blebs >1 cm, often subpleural) are visible to the naked eye.
• Centriacinar (centrilobular) emphysema — upper lobe predominance, associated with smoking; enlargement centred on respiratory bronchioles.
• Panacinar emphysema — lower lobe predominance, associated with α₁-antitrypsin deficiency; uniform destruction from respiratory bronchiole to alveolar sac.
Microscopic appearances:
• Loss of alveolar septa — 'holes in the tissue', fewer alveolar walls per high-power field than normal.
• Remaining walls show capillary loss and mild chronic inflammation.
• No exudate, no granuloma, no tumour — the key diagnostic feature is architectural loss, not filling.
Pathophysiology link: Neutrophil elastase (from tobacco-smoke-activated neutrophils/macrophages) degrades elastin in alveolar walls. α₁-antitrypsin normally inhibits this; its deficiency accelerates destruction.
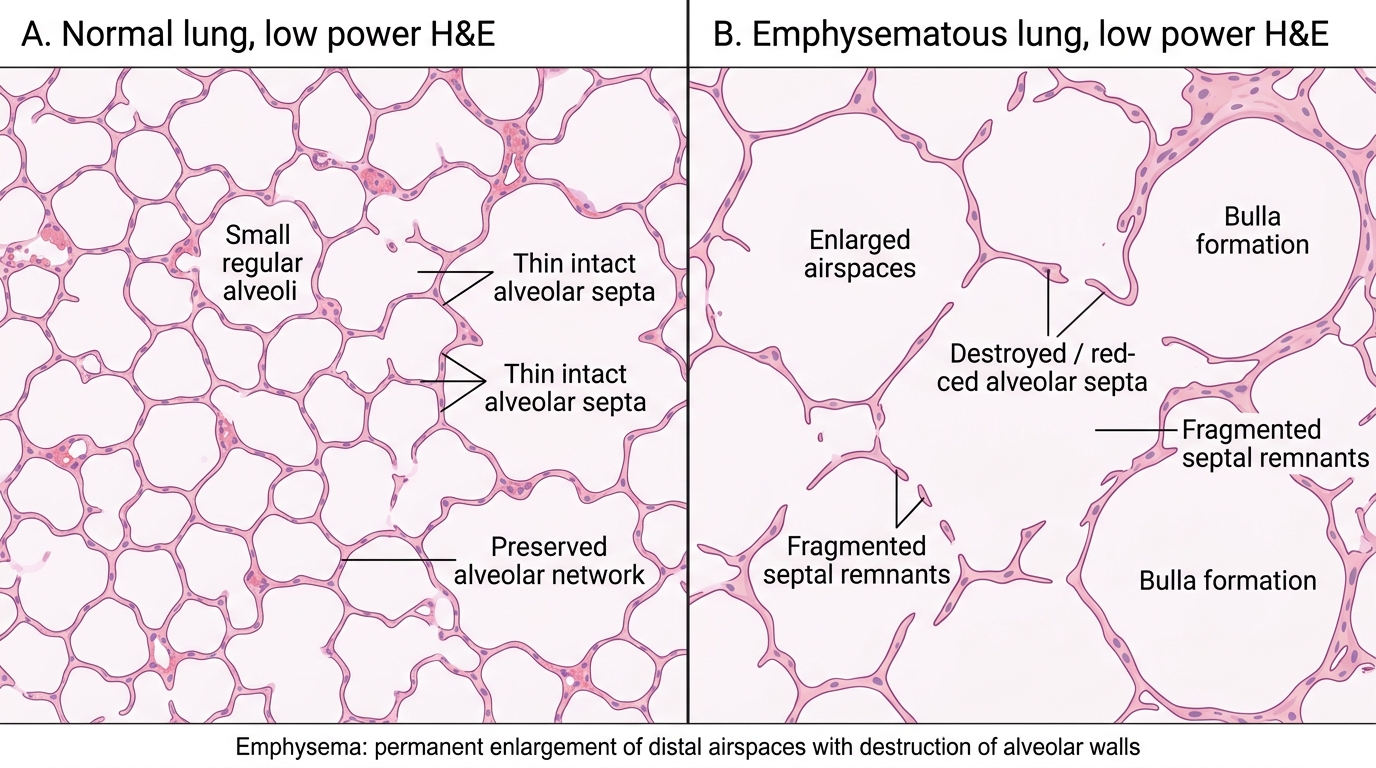
Emphysema: Airspace Destruction on H&E
SELF-CHECK
Which microscopic feature is MOST diagnostic of emphysema, distinguishing it from other causes of radiological hyperinflation?
A. Permanent loss and destruction of alveolar septa
B. Alveoli filled with neutrophilic exudate
C. Caseating granulomas in alveolar walls
D. Proliferation of type II pneumocytes lining intact alveoli
Reveal Answer
Answer: A. Permanent loss and destruction of alveolar septa
Emphysema is defined by permanent destructive enlargement of airspaces distal to the terminal bronchiole — alveolar wall destruction (septal loss) is the pathological hallmark. Neutrophilic exudate filling alveoli indicates pneumonia. Caseating granulomas indicate TB. Type II pneumocyte proliferation is a repair response (e.g., after diffuse alveolar damage) and does not feature septal destruction.
Pneumoconiosis — Dust-Induced Lung Disease
Pneumoconiosis: Gross and Microscopic Patterns
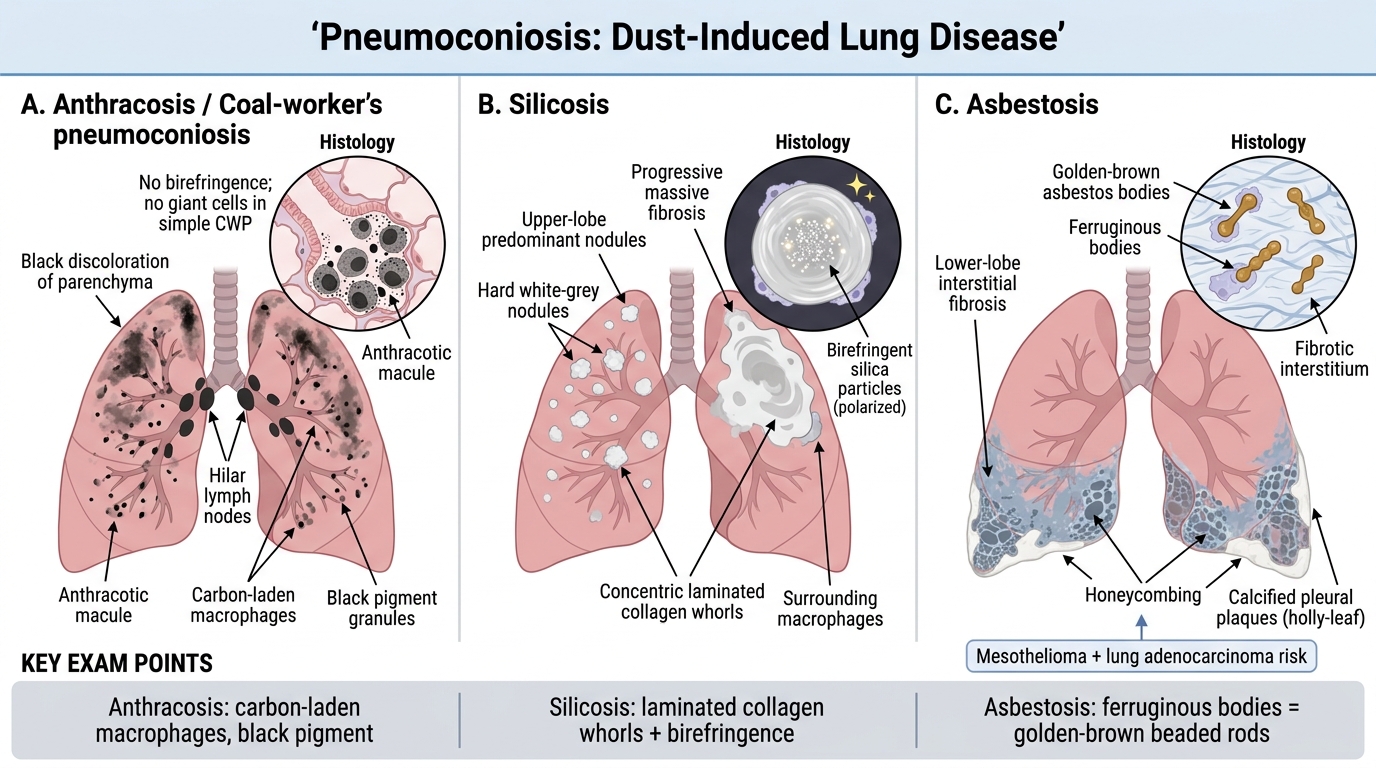
Pneumoconiosis refers to lung diseases caused by inorganic dust inhalation. The three most testable types are:
1. Anthracosis (Coal-worker's pneumoconiosis)
• Gross: Black discolouration of lung parenchyma and hilar nodes; in simple CWP, anthracotic macules (1–2 mm black foci) and slightly larger anthracotic nodules around respiratory bronchioles.
• Micro: Collections of carbon-laden macrophages (anthracotic pigment = black granules) in respiratory bronchioles and surrounding alveoli. No birefringence. No giant cells in simple CWP.
2. Silicosis
• Gross: Multiple hard, white/grey silicotic nodules (2–5 mm, palpable) in upper lobes; in advanced disease nodules coalesce → progressive massive fibrosis.
• Micro: Concentric laminated collagen whorls with birefringent silica particles under polarised light at the centre. Surrounding macrophage reaction.
3. Asbestosis
• Gross: Lower lobe fibrosis (honeycombing), pleural plaques (white, calcified, 'holly-leaf' pattern).
• Micro: Asbestos bodies — golden-brown, dumbbell or beaded rod morphology (ferruginous bodies) formed by protein-iron coating on asbestos fibre. Background interstitial fibrosis.
• Carcinogenic: strongly associated with mesothelioma (pleural) and lung adenocarcinoma.
KEY EXAM POINT: Asbestos bodies = ferruginous bodies = golden-brown beaded rods on H&E. Silica nodules = laminated collagen whorls with birefringence.
CLINICAL PEARL
The latency period for asbestosis-related disease is long — mesothelioma may present 20–40 years after first exposure. When you see a pleural-based tumour in an older male with a history of shipbuilding, construction, or plumbing work, asbestos exposure tops the differential. Silicosis predisposes to secondary TB ('silicotuberculosis') — always check for concurrent granulomas in silicosis sections.
Lung Carcinoma — Histological Classification
Histological Classification of Lung Carcinoma
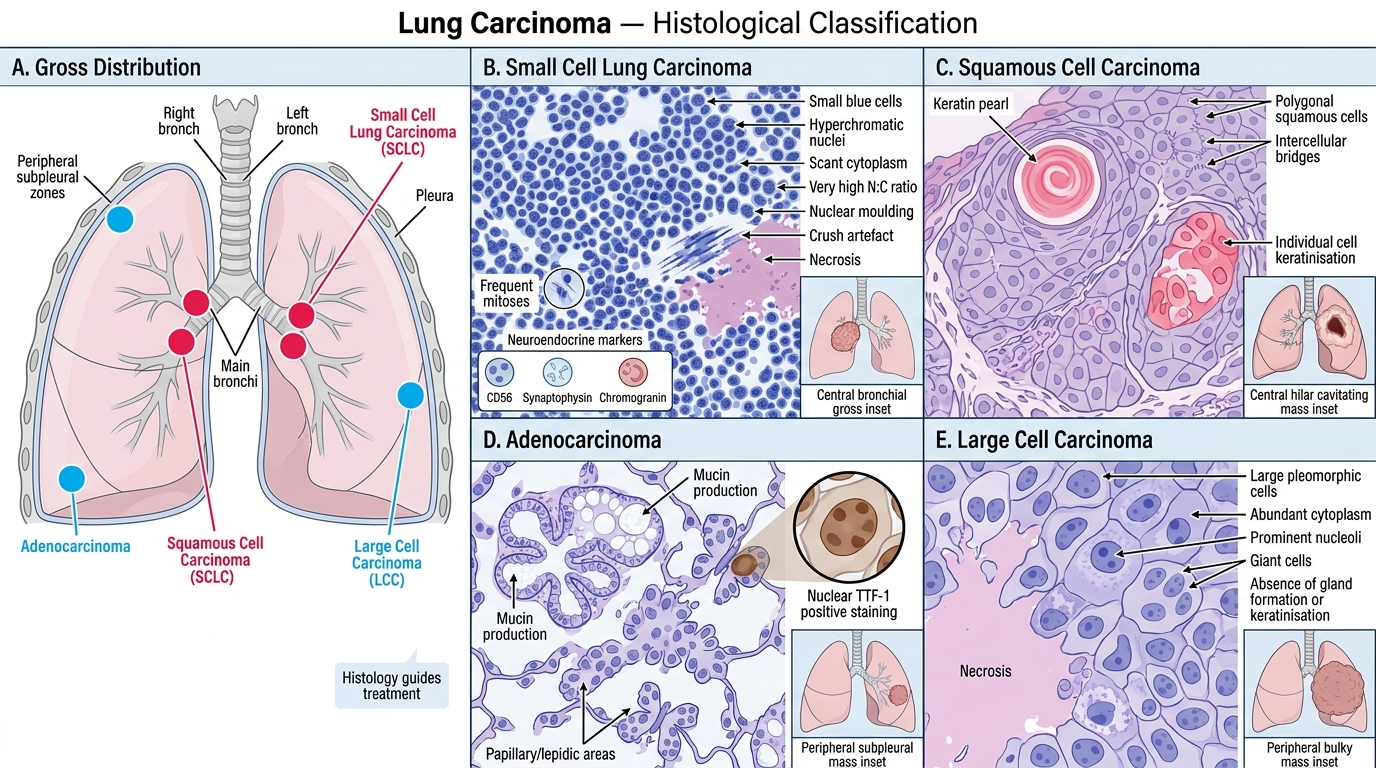
Lung carcinoma is classified primarily by histology because the type dictates treatment. The four main types and their microscopic hallmarks:
Small Cell Lung Carcinoma (SCLC)
• Micro: Sheets and clusters of small cells with:
- Hyperchromatic nuclei, coarsely granular ('salt-and-pepper') chromatin
- Scant cytoplasm — nuclear-to-cytoplasmic ratio is extremely high
- Nuclear moulding — nuclei conform to neighbours' shapes
- Crush artefact — nuclei smear in biopsy specimens (fragile cells)
- Necrosis common; mitoses abundant
• Gross: Central (perihilar) mass, bronchial origin, early mediastinal invasion
• Origin: Neuroendocrine (Kulchitsky cells); does NOT express TTF-1 in same pattern as ADC — immunostaining (CD56, synaptophysin, chromogranin) confirms
Squamous Cell Carcinoma (SCC)
• Micro: Sheets of polygonal cells with:
- Keratin pearls — concentric whorls of keratinising squamous cells, eosinophilic centre
- Intercellular bridges (desmosomes) between adjacent cells
- Individual cell keratinisation (bright pink cytoplasm)
• Gross: Central, hilar mass; may cavitate; often bronchial in origin
Adenocarcinoma
• Micro: Gland-forming structures and/or mucin production
- Acinar, papillary, micropapillary, lepidic patterns
- TTF-1 positive (nuclear)
• Gross: Peripheral mass, often subpleural; most common type in non-smokers and women
• Lepidic growth: tumour cells crawl along intact alveolar walls — 'spread along scaffolding'
Large Cell Carcinoma
• Diagnosis of exclusion: large anaplastic cells, no squamous/glandular/small-cell differentiation; requires IHC panel
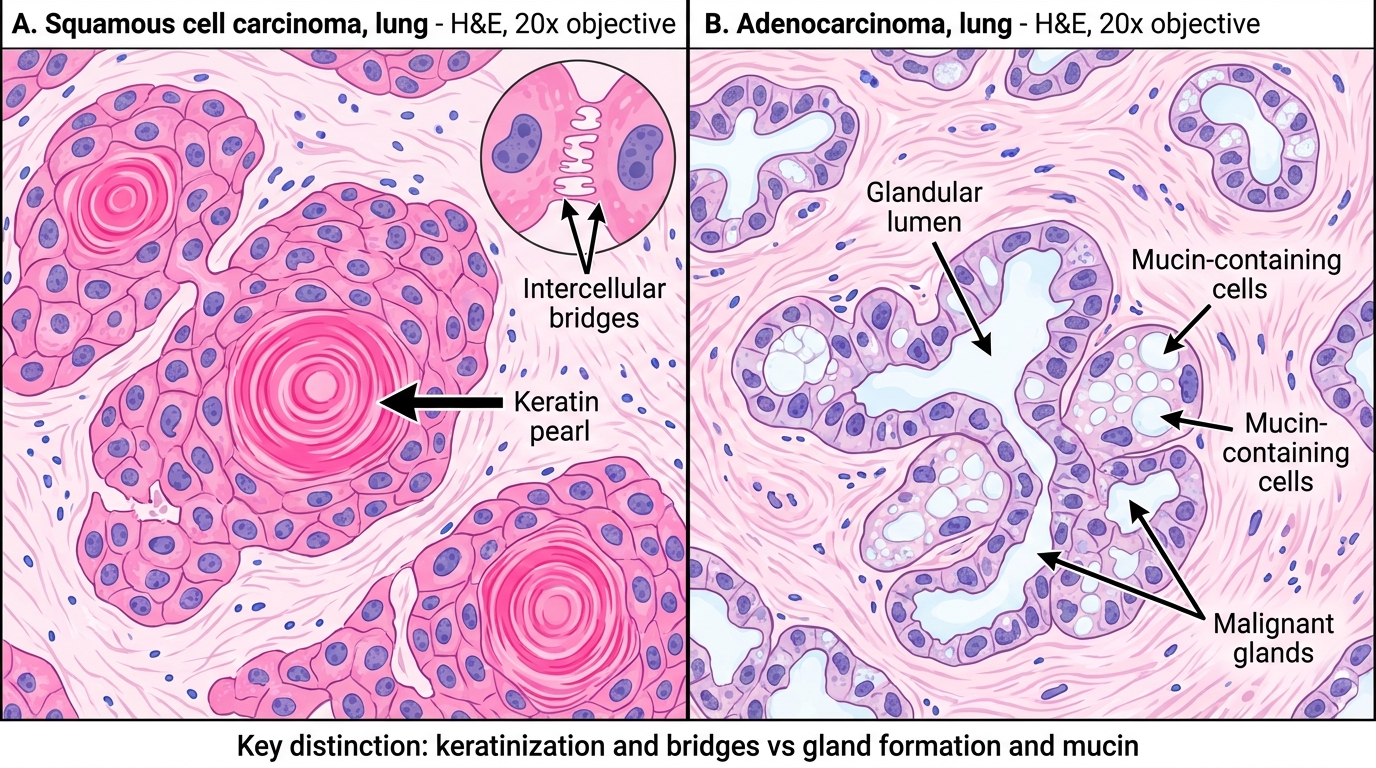
Lung Carcinoma Histology: Squamous Cell Carcinoma vs Adenocarcinoma
SELF-CHECK
A 52-year-old male heavy smoker presents with a central hilar mass. Biopsy shows small cells with scant cytoplasm, nuclear moulding, salt-and-pepper chromatin, and areas of crush artefact. The MOST likely diagnosis is:
A. Squamous cell carcinoma
B. Adenocarcinoma (lepidic pattern)
C. Small cell lung carcinoma
D. Carcinoid tumour
Reveal Answer
Answer: C. Small cell lung carcinoma
The combination of small hyperchromatic cells with scant cytoplasm, nuclear moulding, salt-and-pepper chromatin, and crush artefact is the classic SCLC picture. SCC shows keratin pearls and intercellular bridges. Adenocarcinoma shows gland formation and mucin. Carcinoid also has neuroendocrine features but cells are larger with more cytoplasm and absent crush artefact; carcinoid rarely shows moulding.