Page 25 of 32
PA25.7 | Lung Disease & Tumour Morphology — Practical — SDL Guide (Part 3)
Mesothelioma — The Pleural Rind
Pleural Mesothelioma: The Pleural Rind
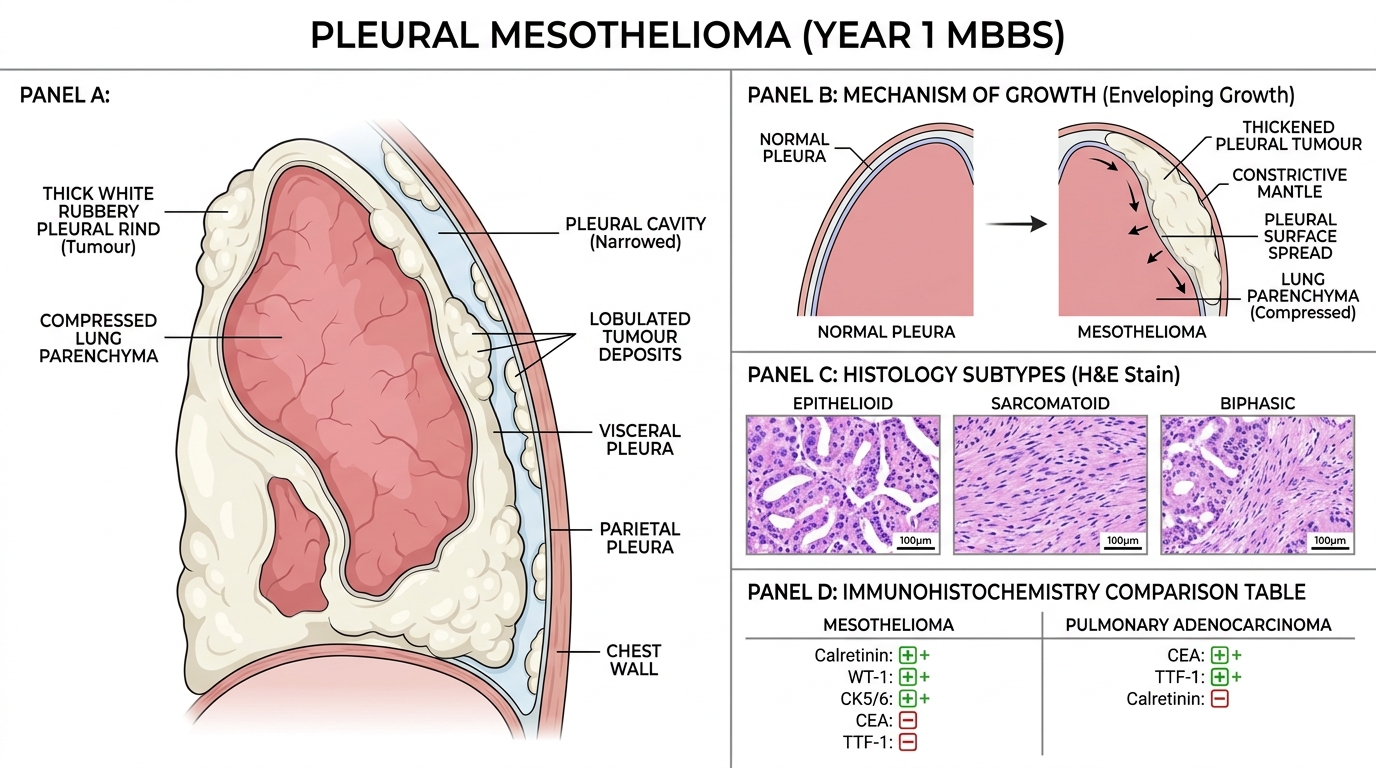
Mesothelioma is a primary tumour of mesothelial cells lining the pleura (rarely peritoneum or pericardium).
Gross: The classic appearance is a thick, white, rubbery pleural rind encasing the lung — the tumour envelops rather than invades; it grows along pleural surfaces forming a constrictive 'mantle'. Effusion is commonly bloody.
Micro: Three histological patterns:
• Epithelioid (most common, ~60%): Cuboidal/polygonal cells forming tubules, papillae, or solid sheets — can mimic adenocarcinoma (important distinction)
• Sarcomatoid: Spindle cells, fibrous stroma
• Biphasic: Mixed epithelioid + sarcomatoid
Key IHC panel (exam-level): Mesothelioma is calretinin+, WT-1+, CK5/6+, CEA−, TTF-1−. This separates it from pulmonary adenocarcinoma (CEA+, TTF-1+, calretinin−).
Aetiology: >80% asbestos-related; latency 20–40 years. Amphibole fibres (crocidolite — blue asbestos) are more carcinogenic than serpentine (chrysotile).
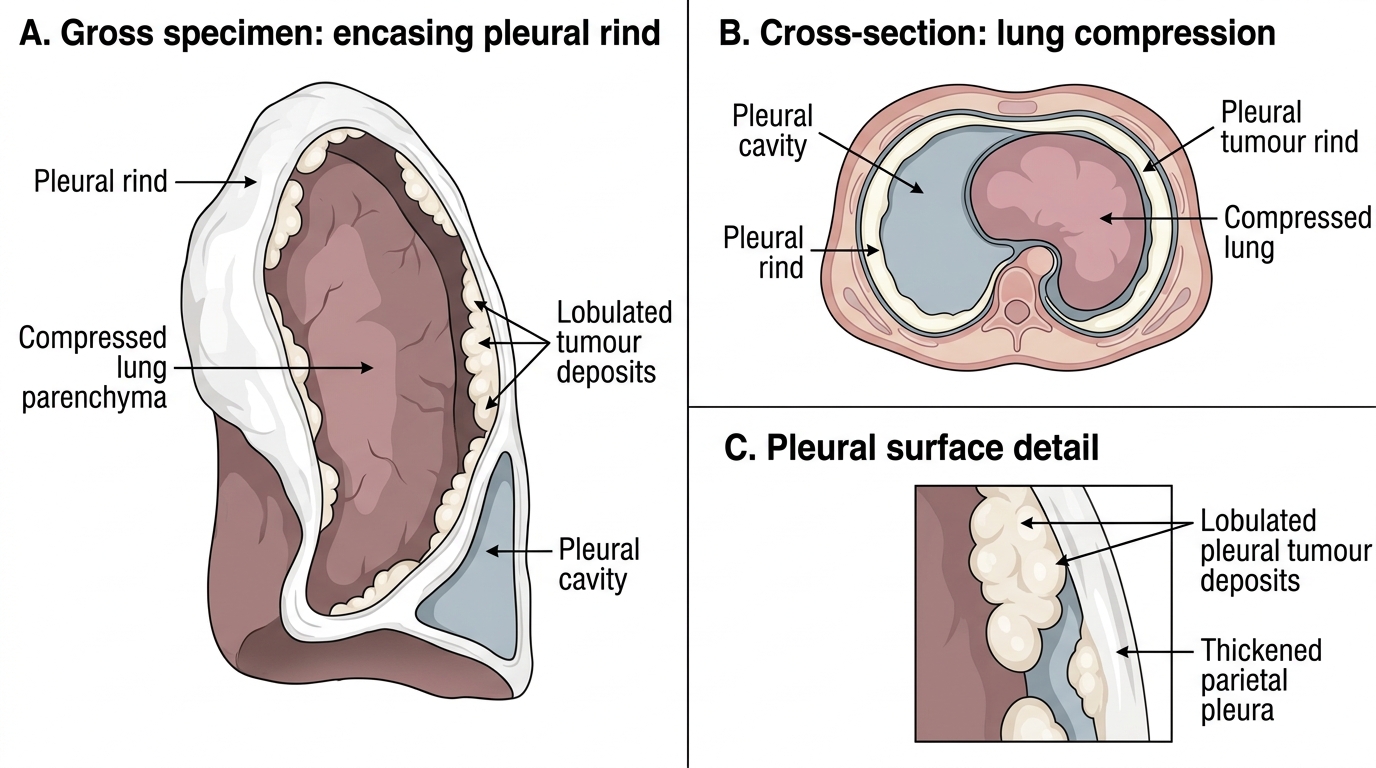
Pleural Mesothelioma: Encasing Pleural Rind
H5P Hotspot Activity — Four-Panel Specimen Grid
Four Lung Specimen Hotspot Grid
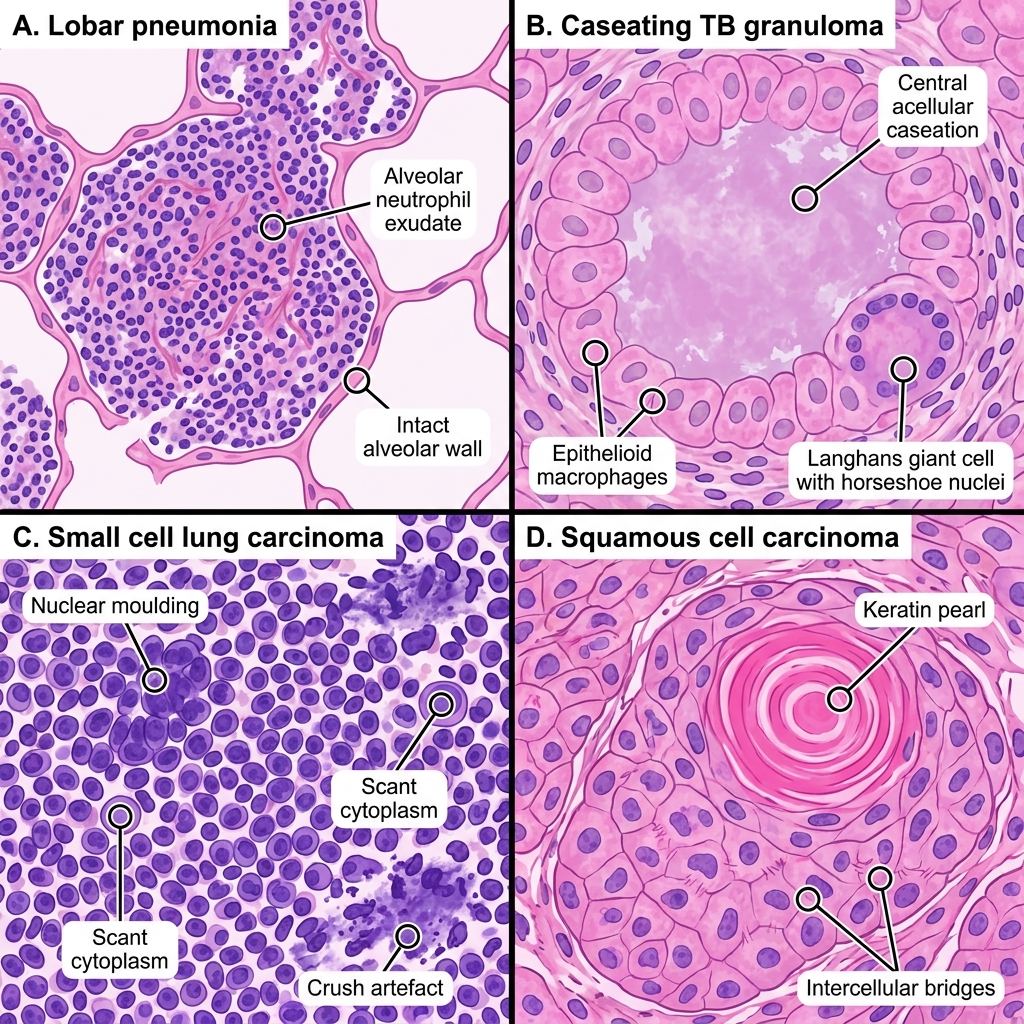
Study the four lung specimens in the composite image below. For each panel, identify the diagnosis using the gross and microscopic features described above. Use the hotspot markers to reveal labelled annotations.
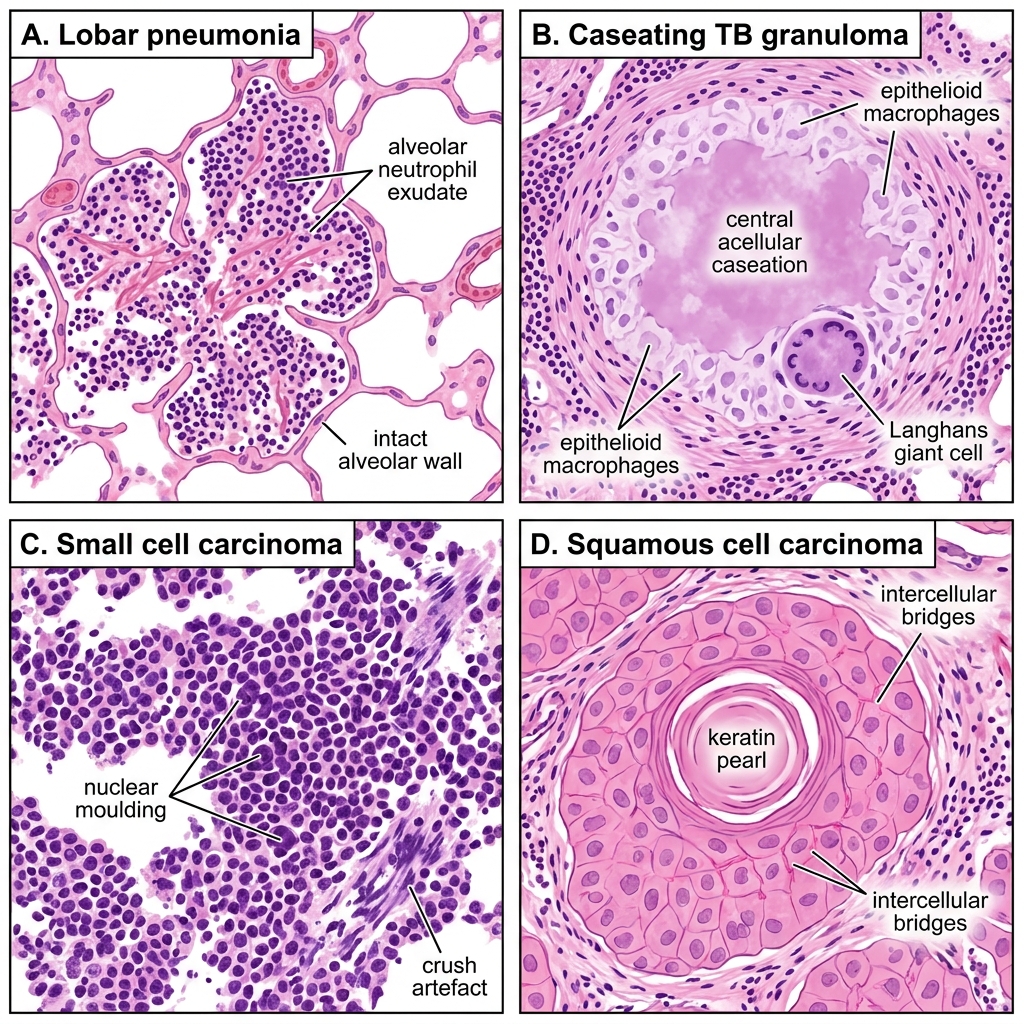
Lung Histopathology Hotspots: Inflammation, Granuloma, and Carcinoma
After reviewing each panel:
• Panel A — What exudate type fills the alveoli? (neutrophilic = bacterial)
• Panel B — What do the peripheral nuclei in the giant cell tell you? (Langhans type = TB)
• Panel C — Why does SCLC show crush artefact? (fragile neuroendocrine cells)
• Panel D — What is the significance of keratin pearls? (squamous differentiation = SCC)
SELF-CHECK
In the 2x2 panel grid, Panel B shows a granuloma with central acellular eosinophilic material and a multinucleated giant cell whose nuclei are arranged in a horseshoe pattern at the periphery. This giant cell morphology is:
A. Touton giant cell — characteristic of xanthogranuloma
B. Langhans giant cell — characteristic of TB and sarcoidosis
C. Foreign body giant cell — nuclei randomly scattered
D. Reed-Sternberg cell — characteristic of Hodgkin lymphoma
Reveal Answer
Answer: B. Langhans giant cell — characteristic of TB and sarcoidosis
Langhans giant cells have nuclei arranged in a horseshoe or peripheral wreath pattern — a hallmark of TB and sarcoidosis granulomas. Touton giant cells (lipid vacuoles centrally, peripheral nuclei wreath) are found in xanthogranulomas. Foreign body giant cells have haphazardly distributed nuclei. Reed-Sternberg cells are binucleated owl-eye cells of Hodgkin lymphoma, not giant cells of granulomas.
Putting It Together — Differential Pattern Grid
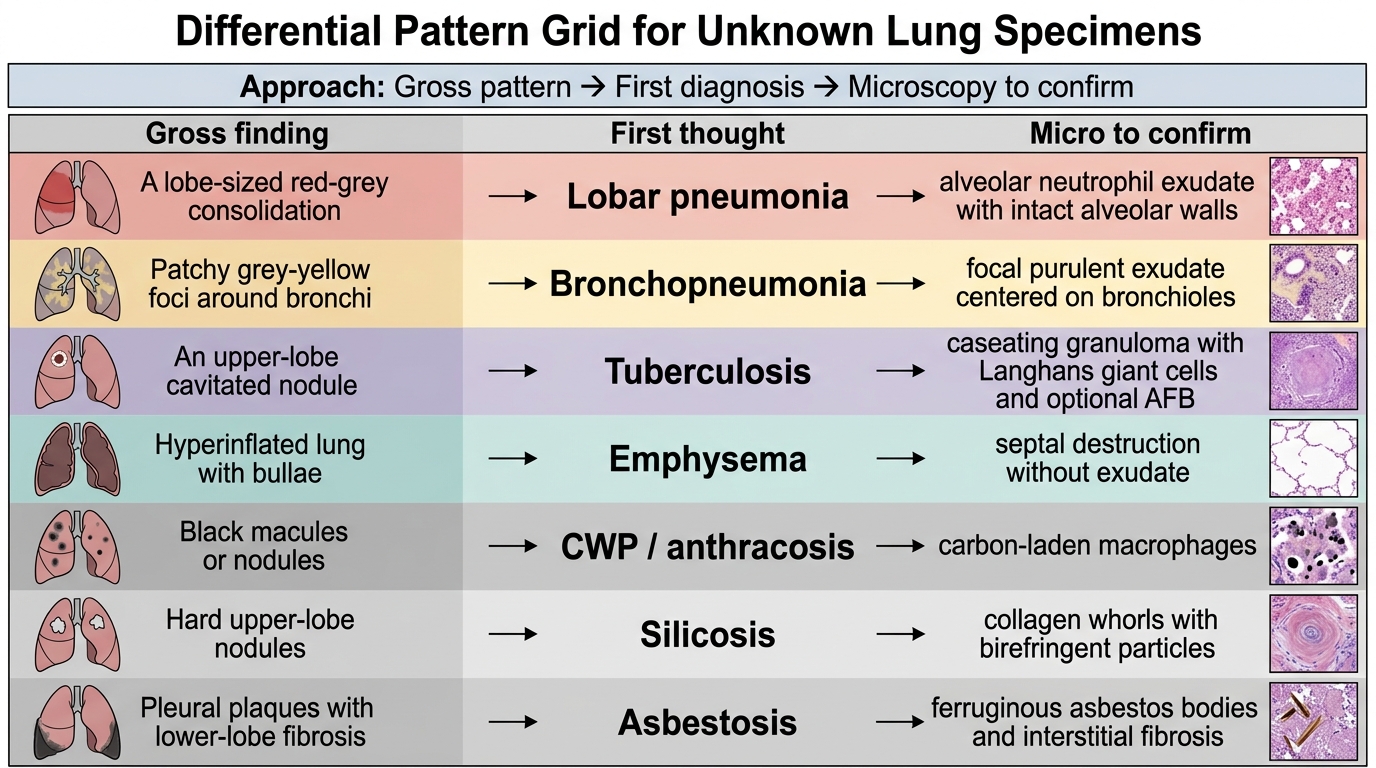
Differential Pattern Grid for Lung Specimens
Use this rapid-read grid when approaching an unknown lung specimen:
| Gross finding | First thought | Micro to confirm |
|---|---|---|
| Lobe-sized consolidation | Lobar pneumonia | Alveolar neutrophil exudate + intact walls |
| Patchy grey-yellow foci | Bronchopneumonia | Focal purulent exudate, bronchiolitis |
| Upper lobe cavitated nodule | TB | Caseating granuloma, Langhans cells, ±AFB |
| Hyperinflated + bullae | Emphysema | Septal destruction, no exudate |
| Black macules or nodules | CWP/anthracosis | Carbon-laden macrophages |
| Hard upper-lobe nodules | Silicosis | Collagen whorls, birefringent particles |
| Pleural plaques + lower fibrosis | Asbestosis | Asbestos bodies (ferruginous) |
| Central hilar mass | SCLC or SCC | SCLC: small cells, moulding; SCC: keratin pearls |
| Peripheral subpleural mass | Adenocarcinoma | Glands, mucin, TTF-1+ |
| Pleural rind | Mesothelioma | Epithelioid/biphasic; calretinin+ |
Whenever a diagnosis seems ambiguous, ask: Is there exudate (infection), destruction (emphysema/fibrosis), granuloma (TB/sarcoidosis), or abnormal architecture (neoplasm)? These four questions exclude 90% of conditions by pattern.