Page 5 of 32
PA25.3 | Obstructive Airway Disease & Bronchiectasis — SDL Guide
Learning Objectives
- Distinguish obstructive from restrictive lung disease using spirometry patterns (FEV1/FVC ratio)
- Define emphysema and describe its four morphological types with their distinct etiologies
- Explain the protease-antiprotease and oxidant-antioxidant imbalance in COPD pathogenesis
- Define chronic bronchitis clinically and histologically (Reid index); contrast with emphysema
- Describe the immunological basis and airway morphology of asthma including Curschmann spirals and Charcot-Leyden crystals
- Define bronchiectasis, enumerate its causes, and trace the obstruction-infection cycle
- List complications of COPD and bronchiectasis including cor pulmonale
INSTRUCTIONS
Obstructive airway diseases -- COPD, asthma, and bronchiectasis -- rank among the leading causes of chronic morbidity worldwide and are a high-yield area in final MBBS examinations and clinical postings. Building on your Year-1 knowledge of respiratory physiology and anatomy, this module uses the spirometric FEV1/FVC ratio as an anchor to organise the COPD spectrum, then extends to asthma and bronchiectasis. You will move from mechanism to morphology to clinical picture -- exactly the framework examiners expect.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 15 -- The Lung (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 16 -- Respiratory System (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old retired carpenter arrives breathless after climbing one flight of stairs. Chest X-ray shows hyperinflated lungs with a flattened diaphragm. Spirometry: FEV1/FVC = 0.52 (normal >0.70). He smoked 40 pack-years and has never had wheeze. Meanwhile, the patient in the next bed -- also breathless -- has a productive cough every winter for the past four years, a barrel chest, and a sputum culture growing Haemophilus influenzae. Same spirometry pattern, entirely different disease process. By the end of this session you will know exactly why.
WHY THIS MATTERS
COPD affects over 250 million people globally and is the third leading cause of death. Asthma affects 350 million. Bronchiectasis is common in post-tubercular lungs -- highly relevant in South Asian practice. These diseases appear in Short Answer Questions (SAQs), clinical case vignettes, and OSCE spirometry interpretation stations. Understanding the FEV1/FVC framework lets you classify any obstructive disease quickly -- a skill you will use every clinical posting.
RECALL
Before continuing, recall from your Year-1 respiratory physiology:
- FEV1 = forced expiratory volume in 1 second. Reflects airway resistance.
- FVC = forced vital capacity. Reflects total lung volume.
- Normal FEV1/FVC ratio >= 0.70.
- In obstruction, airways narrow -> FEV1 falls disproportionately -> ratio <0.70.
- In restriction, both FEV1 and FVC fall equally -> ratio preserved (>0.70) but absolute volumes are small.
- Surfactant (Year-1 biochemistry): produced by Type II pneumocytes; reduces alveolar surface tension.
Obstructive vs Restrictive Pattern -- The Gateway Distinction
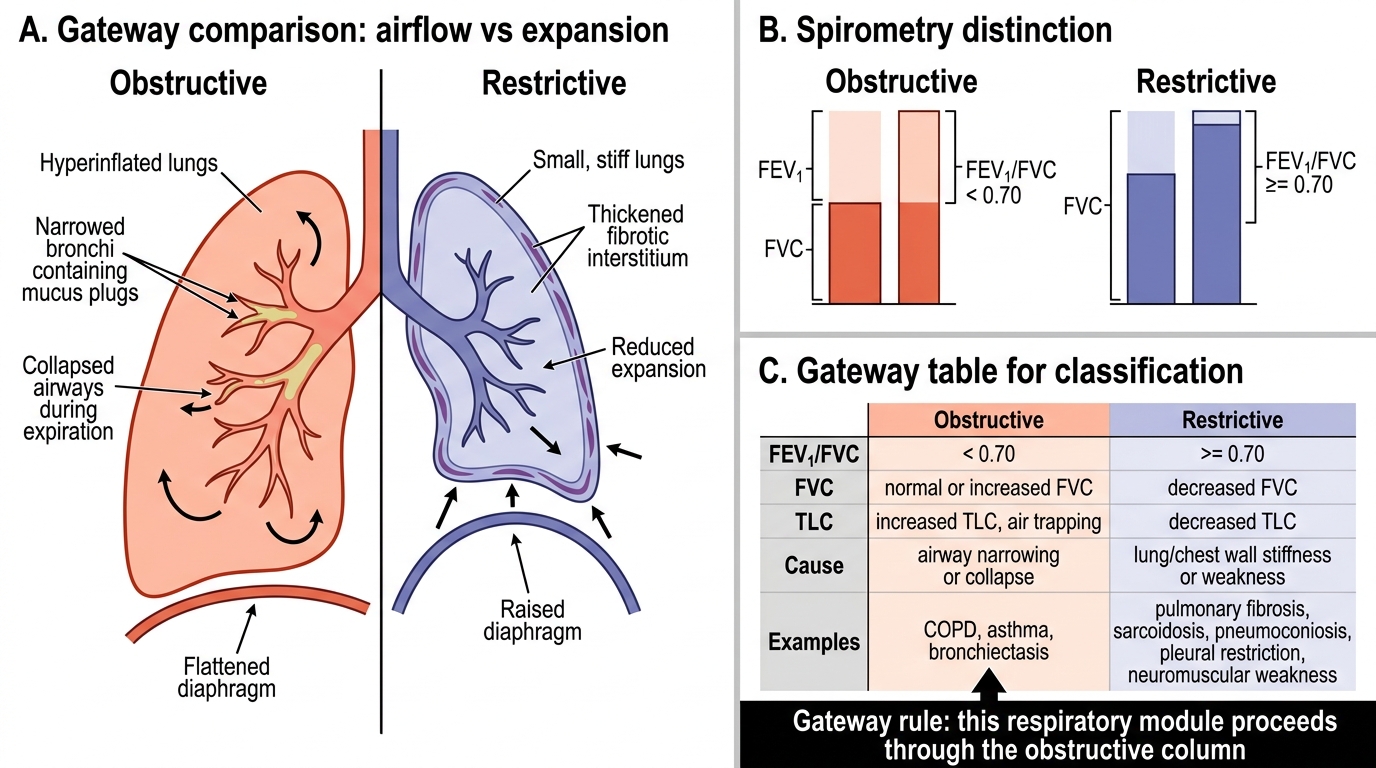
Obstructive vs Restrictive Lung Pattern: The Gateway Distinction
Obstructive lung disease is defined by a reduced FEV1/FVC ratio (<0.70). Airflow is impeded during expiration because airways are narrowed, collapsed, or plugged. Total lung capacity (TLC) is normal or increased (air trapping). Examples: COPD (emphysema + chronic bronchitis), asthma, bronchiectasis.
Restrictive lung disease shows a reduced FVC with a preserved or elevated FEV1/FVC ratio. The lung cannot fully expand. Examples: pulmonary fibrosis, sarcoidosis, pneumoconiosis, pleural restriction, neuromuscular weakness.
| Feature | Obstructive | Restrictive |
|---|---|---|
| FEV1/FVC | < 0.70 | >= 0.70 |
| FVC | Normal or increased | Decreased |
| TLC | Increased (air-trapped) | Decreased |
| Cause | Airway narrowing | Lung/chest wall stiffness |
This table is your single gateway. Every subsequent disease in this module falls in the obstructive column.
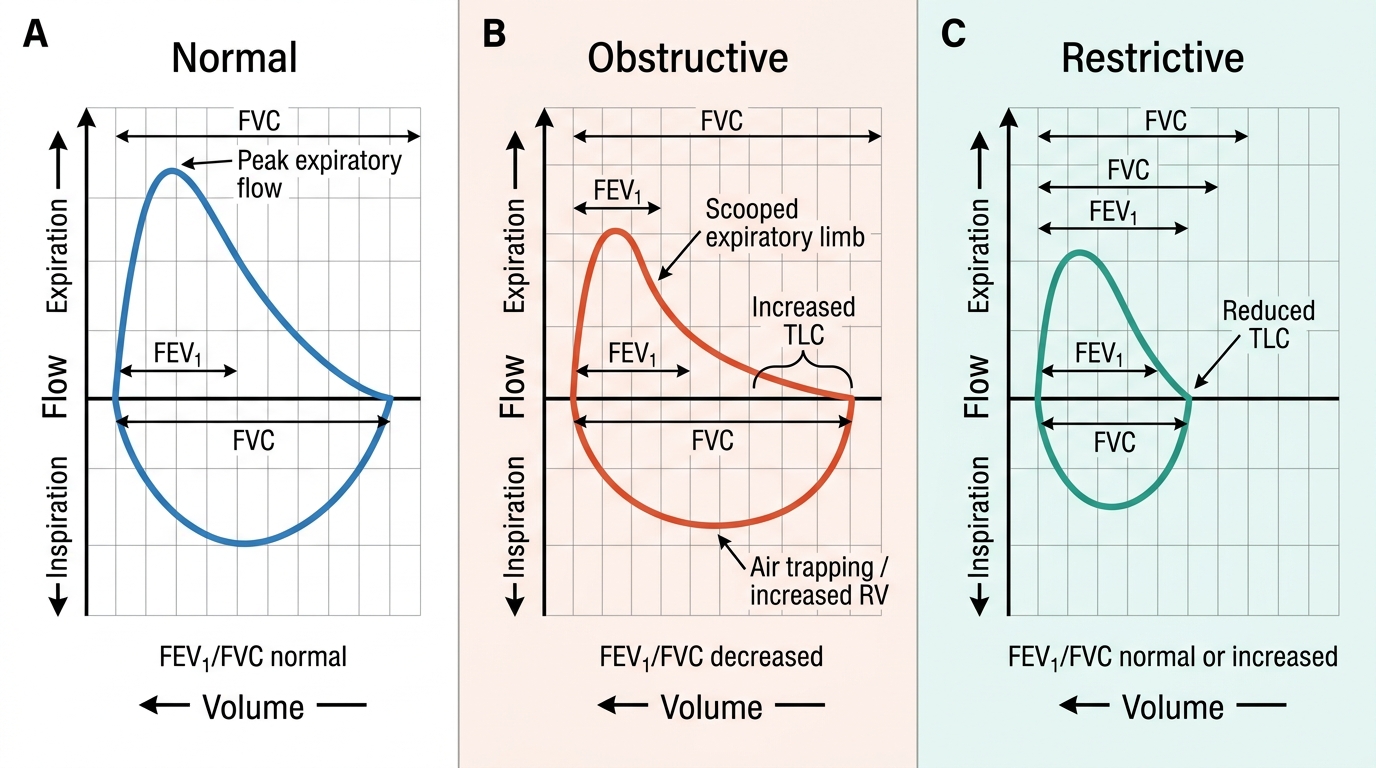
Spirometry Flow-Volume Loop Patterns
COPD -- Overview and Pathogenesis
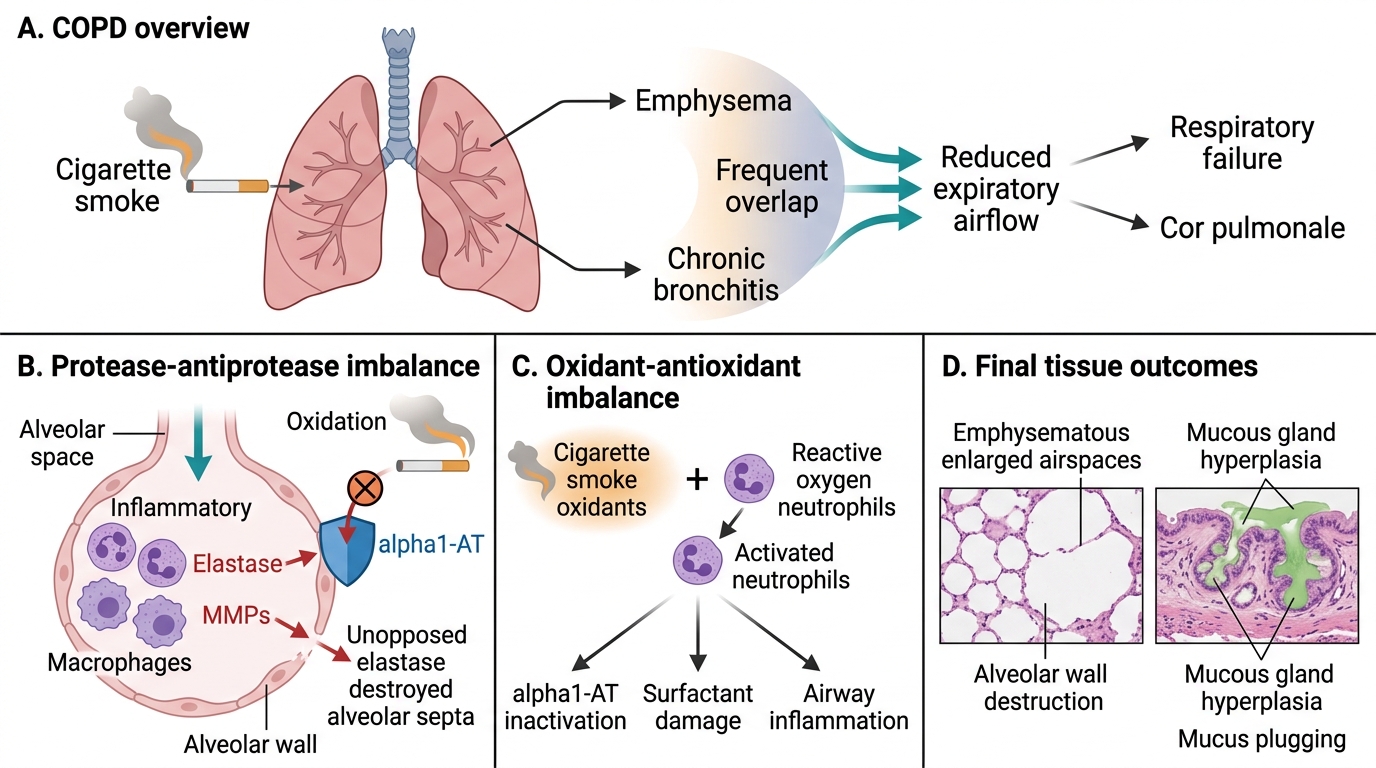
COPD: Overview and Pathogenesis
COPD (Chronic Obstructive Pulmonary Disease) is an umbrella term for two related but distinct conditions that frequently overlap -- emphysema and chronic bronchitis. Both reduce expiratory airflow, both are primarily caused by smoking, and both progress to respiratory failure and cor pulmonale.
Pathogenesis -- Two Imbalances:
- Protease-antiprotease imbalance: Cigarette smoke recruits neutrophils and macrophages into alveoli. These release elastase (and matrix metalloproteinases) that digest the alveolar wall. Normally, alpha-1-antitrypsin (alpha1-AT) inhibits elastase. Smoking inactivates alpha1-AT by oxidation -> unopposed elastase -> alveolar wall destruction.
- Oxidant-antioxidant imbalance: Cigarette smoke itself contains oxidants; activated neutrophils generate reactive oxygen species. These oxidants inactivate alpha1-AT, damage surfactant, and trigger airway inflammation directly.
Key link: Both imbalances converge on the same outcome -- destruction of alveolar walls and/or mucous gland hyperplasia depending on which zone of the lung is affected.
Emphysema -- Definition, Types, and Morphology
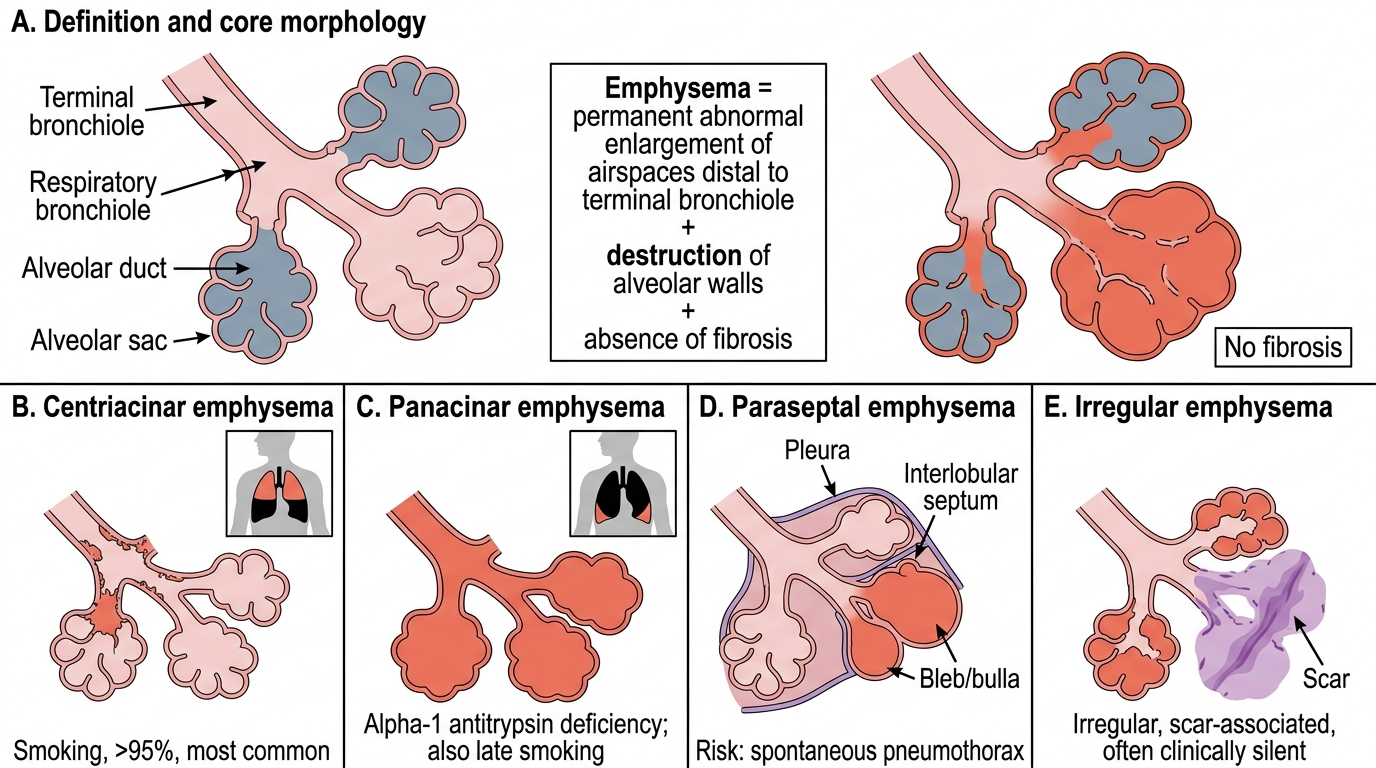
Emphysema: Definition and Morphological Types
Emphysema is defined as permanent abnormal enlargement of airspaces distal to the terminal bronchiole, accompanied by destruction of alveolar walls, without fibrosis.
Three elements are non-negotiable in the definition: permanent enlargement, wall destruction, absence of fibrosis.
Four morphological types:
| Type | Zone destroyed | Cause | Note |
|---|---|---|---|
| Centriacinar (centrilobular) | Proximal acinus -- respiratory bronchioles | Smoking (>95%) | Most common; upper lobe predominance |
| Panacinar (panlobular) | Entire acinus -- proximal to distal | alpha1-antitrypsin deficiency; also late smoking | Lower lobe predominance |
| Paraseptal (distal acinar) | Distal acinus near septa/pleura | Idiopathic; young adults | Causes spontaneous pneumothorax |
| Irregular (scar emphysema) | Irregular; around scars | Post-inflammatory fibrosis | No clinical syndrome |
Morphology:
- Gross: lungs voluminous, pale, fluffy, don't collapse on opening chest; bullae (>1 cm) in paraseptal type.
- Micro: enlarged airspaces with thinned, destroyed alveolar walls; pink puffer phenotype -- pursed-lip breathing to maintain positive end-expiratory pressure, thin, barrel-chested, markedly dyspnoeic but relatively pink (hyperventilates to maintain PaO2).
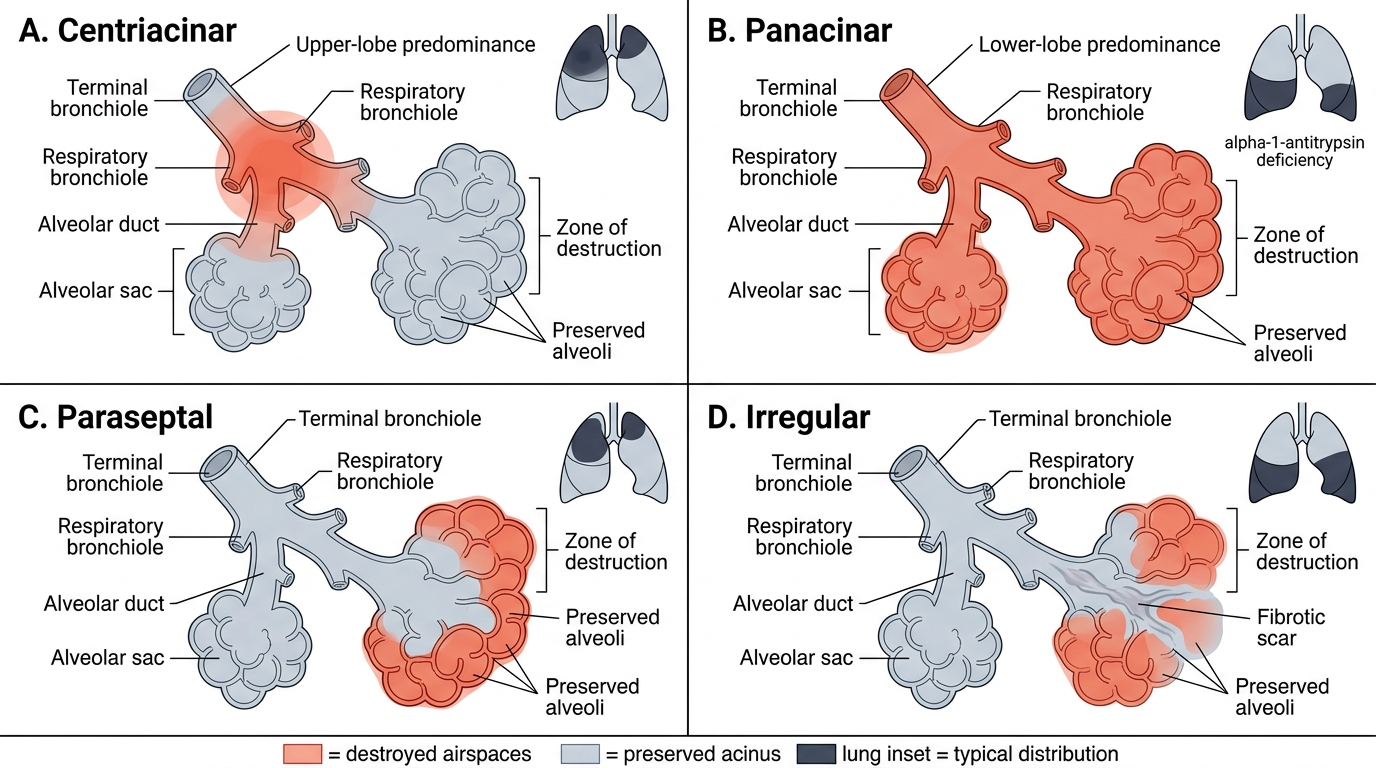
Types of Emphysema: Acinar Destruction Patterns
SELF-CHECK
A 45-year-old non-smoker with no respiratory symptoms is found to have lower-lobe predominant emphysema on CT. Which enzyme deficiency is most likely responsible?
A. Myeloperoxidase
B. alpha-1-Antitrypsin
C. Superoxide dismutase
D. Surfactant protein B
Reveal Answer
Answer: B. alpha-1-Antitrypsin
alpha-1-Antitrypsin (alpha1-AT) deficiency causes panacinar (panlobular) emphysema with lower-lobe predominance in non-smokers -- classically presenting in the 4th-5th decade. alpha1-AT normally inhibits neutrophil elastase; without it, alveolar walls are unprotected. Myeloperoxidase generates oxidants but its deficiency doesn't cause emphysema. Surfactant protein B deficiency causes neonatal respiratory distress, not adult emphysema.