Page 6 of 32
PA25.3 | Obstructive Airway Disease & Bronchiectasis — SDL Guide (Part 2)
Chronic Bronchitis -- Definition, Reid Index, and Phenotype
Chronic Bronchitis: Definition, Reid Index, and Blue Bloater Phenotype
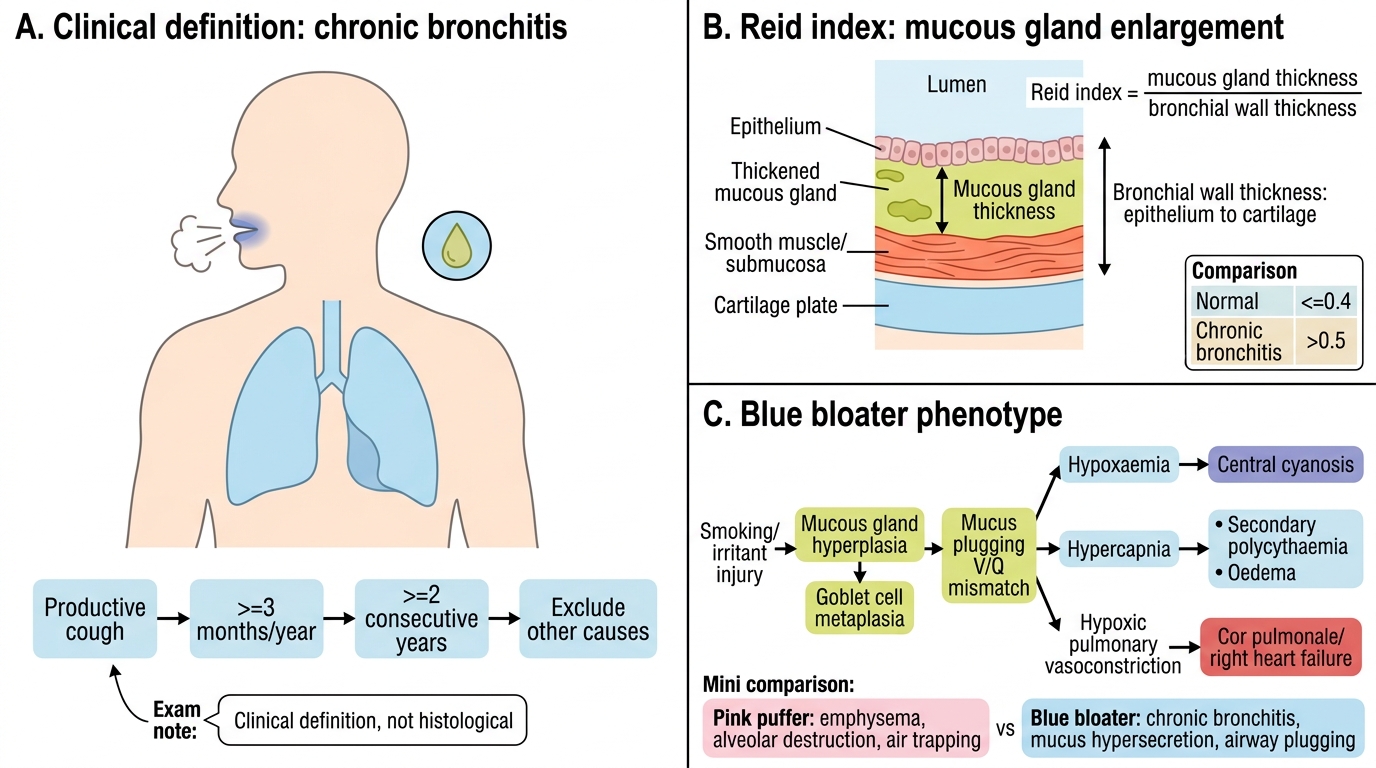
Chronic bronchitis is defined clinically, not histologically: productive cough for at least 3 consecutive months in at least 2 consecutive years, after exclusion of other causes.
This clinical definition is crucial -- examiners often test it against the morphological definition of emphysema.
Pathology -- Reid Index:
- Smoking -> irritant injury -> submucosal mucous gland hypertrophy and hyperplasia -> excessive mucus production.
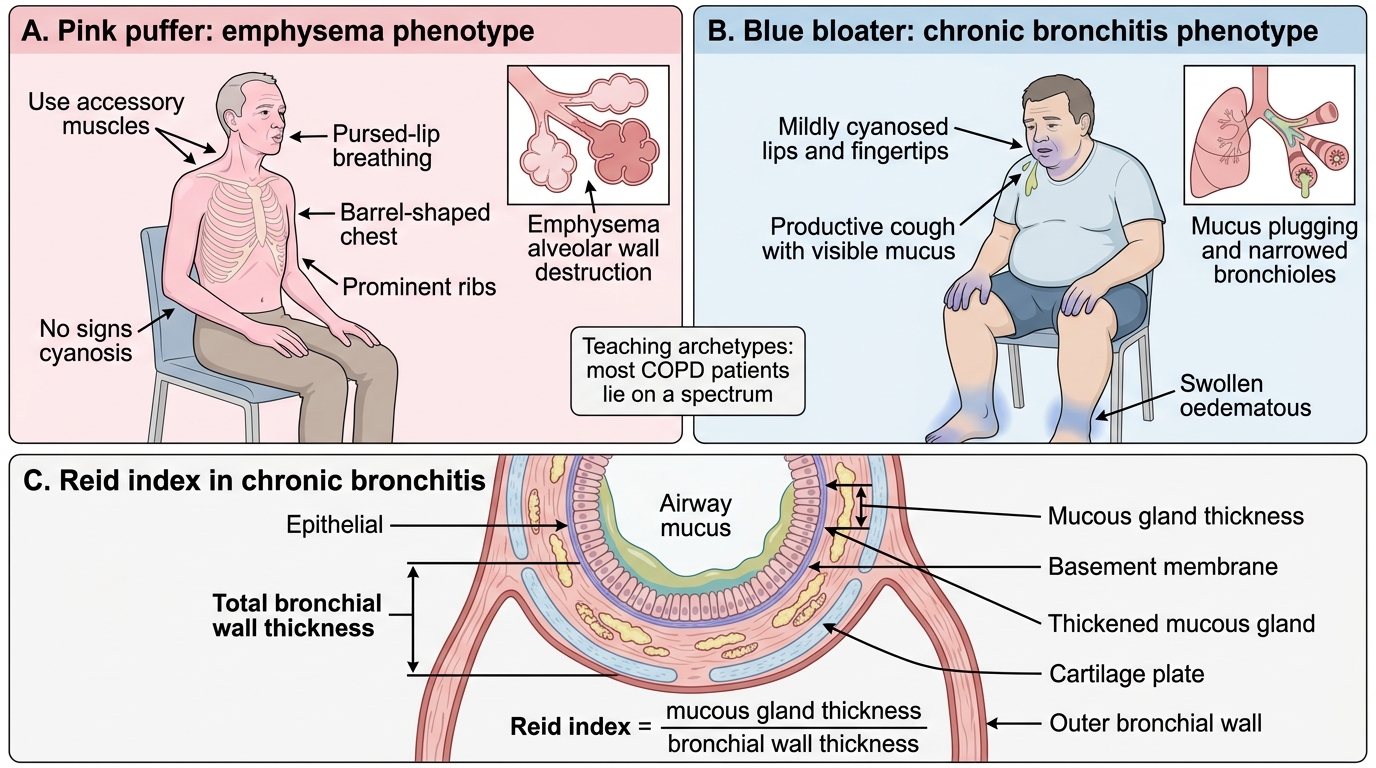
- Reid index = ratio of mucous gland thickness to bronchial wall thickness (from epithelium to cartilage). Normal <=0.4; chronic bronchitis >0.5.
- Additional histology: goblet cell metaplasia extending into peripheral airways; inflammatory infiltrate; bronchial wall oedema.
Clinical phenotype -- "Blue Bloater":
- Hypoxaemia (V/Q mismatch from mucus plugging) -> central cyanosis (blue).
- Hypercapnia -> secondary polycythaemia and oedema (bloater).
- Hypoxic pulmonary vasoconstriction -> cor pulmonale (right heart failure).
- Relatively less dyspnoeic than the emphysema patient; tends to be overweight.
Pink Puffer vs Blue Bloater -- a comparison:
| Feature | Pink Puffer (Emphysema) | Blue Bloater (Chronic Bronchitis) |
|---|---|---|
| Dominant mechanism | Alveolar destruction, air trapping | Mucus hypersecretion, airway plugging |
| PaO2 | Near normal (hyperventilates) | Low (cyanosis) |
| PaCO2 | Low or normal | Raised |
| Build | Thin, barrel chest | Stocky, oedematous |
| Cyanosis | Absent/late | Present |
| Cor pulmonale | Late | Early |
COPD Archetypes and Reid Index
CLINICAL PEARL
The 'Pink Puffer' and 'Blue Bloater' are teaching archetypes -- most COPD patients fall somewhere on the spectrum between the two, not at either extreme. The distinction is still high-yield for written exams because it maps directly onto two different pathophysiological mechanisms: alveolar destruction (emphysema) versus mucus-driven V/Q mismatch (chronic bronchitis). In clinicals, patients with COPD exacerbation often show features of both.
Asthma -- Pathogenesis and Classification
Asthma: Pathogenesis and Classification
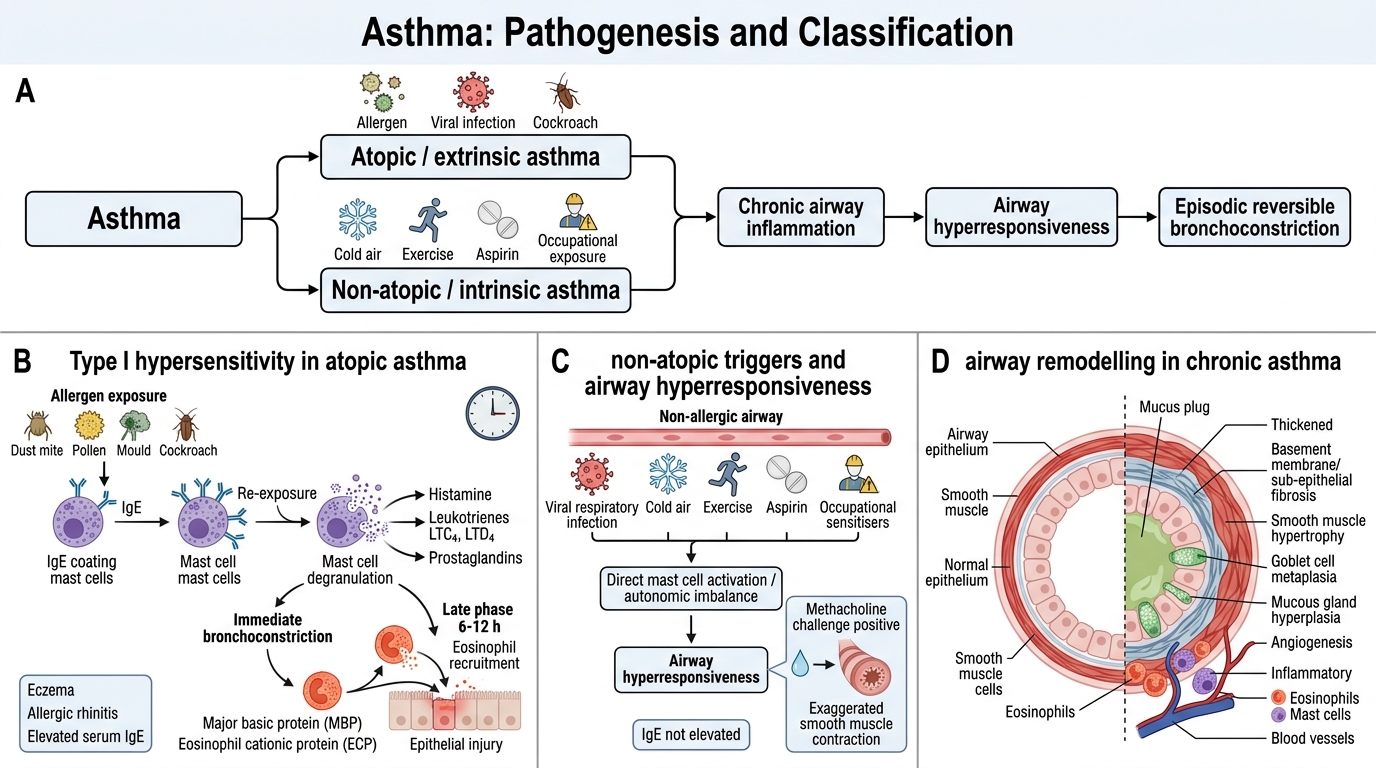
Asthma is a chronic inflammatory airway disease characterised by episodic, reversible bronchoconstriction, airway hyperresponsiveness, and airway remodelling.
Two main types:
1. Atopic (extrinsic) asthma -- Type I (IgE-mediated) hypersensitivity. Sensitisation to environmental allergens (dust mites, pollens, moulds, cockroach antigen) -> IgE production -> mast cell sensitisation. Re-exposure -> mast cell degranulation -> histamine, leukotrienes (LTC4, LTD4), prostaglandins -> immediate bronchoconstriction.
- Late-phase response (6-12 h): eosinophils recruited -> major basic protein (MBP) and eosinophil cationic protein (ECP) cause epithelial damage.
- Associated with eczema, allergic rhinitis (atopic triad). Elevated serum IgE.
- Non-atopic (intrinsic) asthma -- No demonstrable allergy. Triggered by respiratory infections (viral), cold air, exercise, aspirin, occupational sensitisers. IgE not elevated. Mechanism less well understood -- possibly direct mast cell activation or autonomic imbalance.
Airway hyperresponsiveness: Both types share exaggerated bronchoconstrictor response to nonspecific stimuli (methacholine challenge positive). This 'twitchy airway' reflects chronic inflammation lowering the threshold for smooth muscle contraction.
Airway remodelling (chronic/severe asthma): Repeated inflammation -> sub-epithelial fibrosis, smooth muscle hypertrophy, goblet cell metaplasia, mucous gland hyperplasia, angiogenesis -> partially irreversible obstruction.
Asthma -- Morphology
Asthma Morphology: Airway Remodeling and Sputum Findings
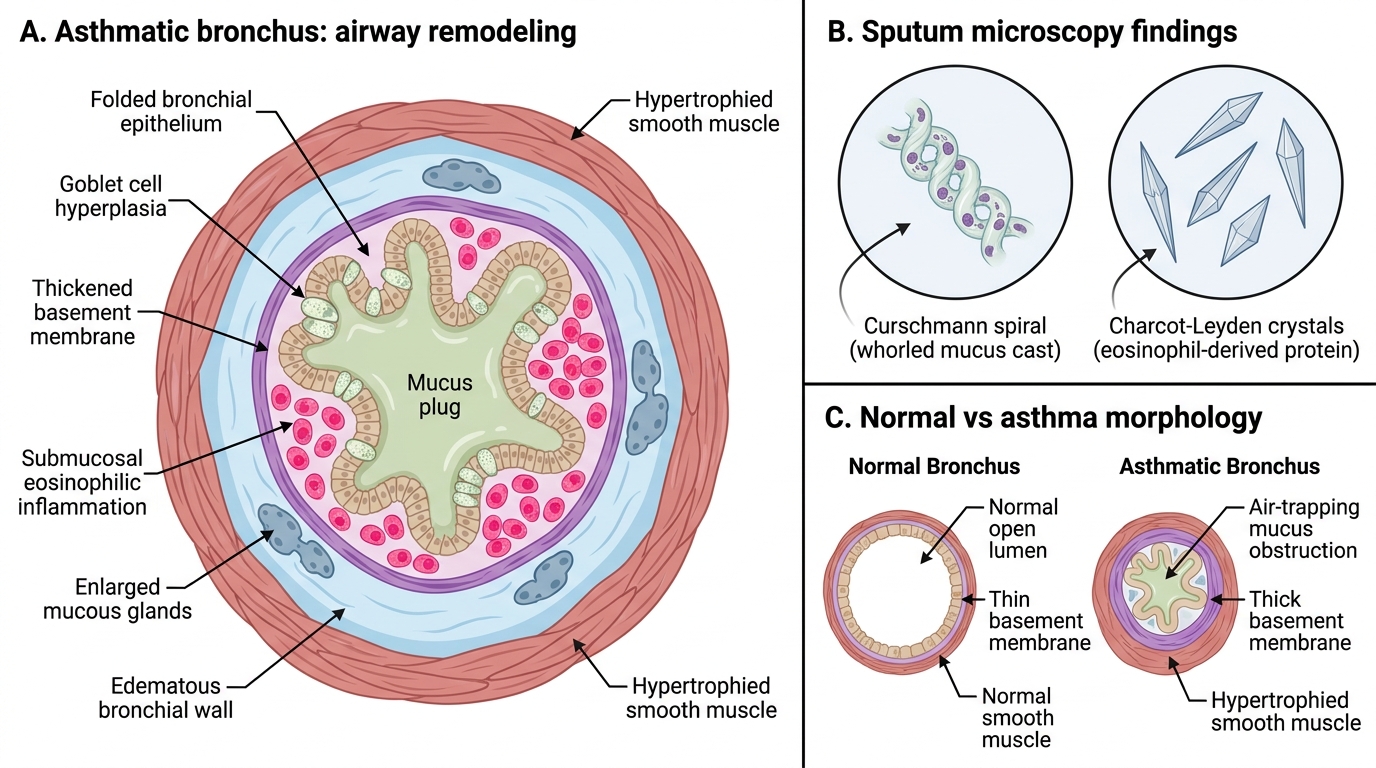
The histological picture of asthma is distinctive and high-yield.
Macroscopy:
- Overdistended lungs (air-trapping).
- Airways filled with thick, tenacious mucus plugs.
- Bronchial walls thickened.
Microscopy -- four cardinal features:
- Curschmann spirals -- whorled mucus plugs cast from small airways; seen in sputum cytology.
- Charcot-Leyden crystals -- bipyramidal crystals formed from eosinophil membrane protein (galectin-10/lysophospholipase); found in sputum and tissues.
- Eosinophils -- the dominant inflammatory cell in atopic asthma; submucosal and luminal.
- Basement membrane thickening -- sub-epithelial collagen deposition (Type III/V collagen); a hallmark of remodelling, often called 'hyaline thickening'.
Additional features: goblet cell hyperplasia; smooth muscle hypertrophy; mucous gland enlargement; oedema of the bronchial wall; mast cells increased.
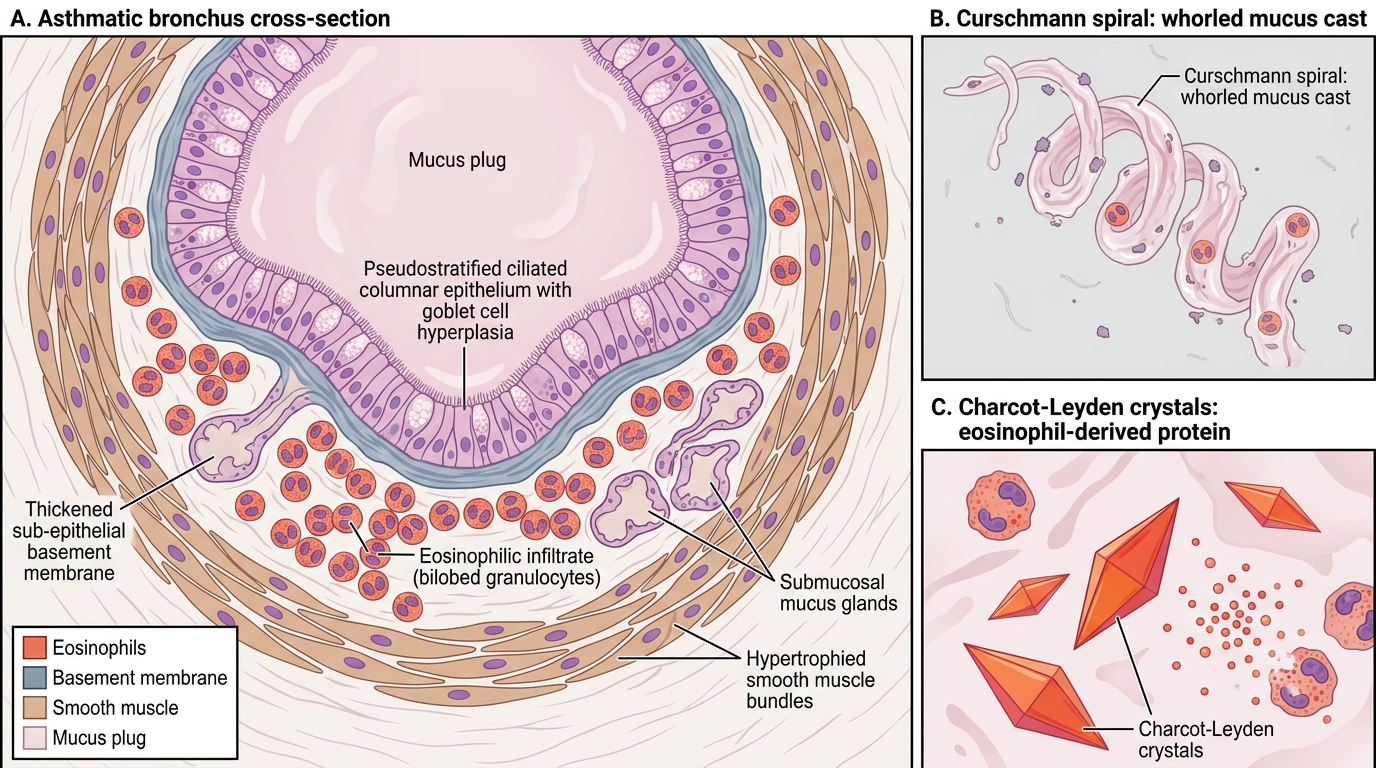
Asthmatic Bronchus: Histologic Features and Sputum Findings
SELF-CHECK
A 22-year-old medical student develops episodic breathlessness and wheeze since moving into a hostel. Sputum microscopy shows whorled mucus casts and bipyramidal crystals. Serum IgE is elevated. Which finding directly indicates eosinophil-derived protein deposition?
A. Elevated serum IgE
B. Curschmann spirals
C. Charcot-Leyden crystals
D. Sub-epithelial basement membrane thickening
Reveal Answer
Answer: C. Charcot-Leyden crystals
Charcot-Leyden crystals are formed from galectin-10 (lysophospholipase), a protein derived from eosinophil membranes -- they directly signal eosinophil degranulation. Curschmann spirals are whorled mucus casts from small airways (not eosinophil-specific). Elevated IgE indicates type I hypersensitivity, not eosinophil activity specifically. Basement membrane thickening reflects remodelling fibrosis rather than eosinophil protein.