Page 7 of 32
PA25.3 | Obstructive Airway Disease & Bronchiectasis — SDL Guide (Part 3)
Bronchiectasis -- Definition, Causes, and the Obstruction-Infection Cycle
Bronchiectasis: Definition, Causes, and Obstruction-Infection Cycle
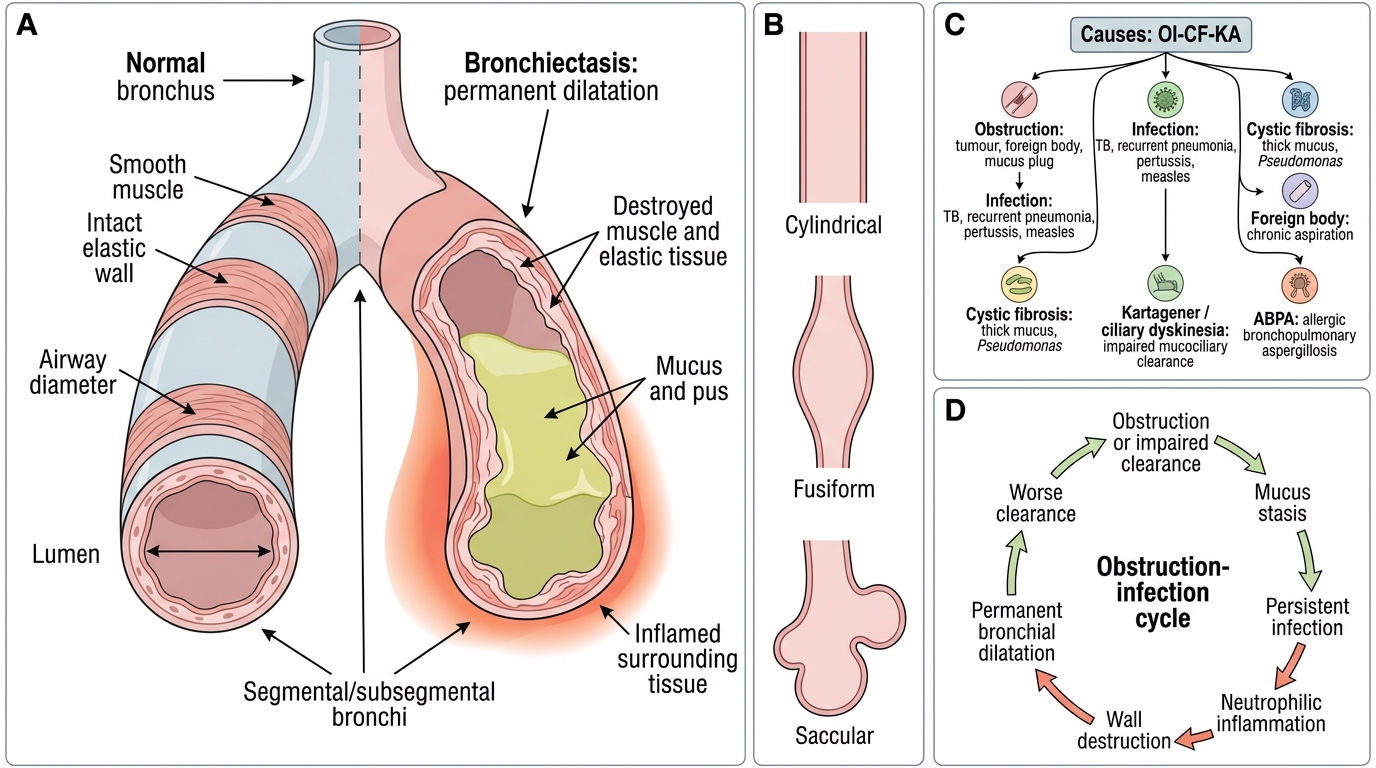
Bronchiectasis is defined as permanent, abnormal dilatation of bronchi and bronchioles resulting from destruction of the muscular and elastic components of the bronchial wall.
Key word: permanent (unlike reversible dilatation in acute pneumonia). The bronchi involved are typically segmental and subsegmental; they may be cylindrical, fusiform, or saccular (cystic).
Causes -- a practical mnemonic (OI-CF-KA):
| Category | Example |
|---|---|
| Obstruction | Tumour, foreign body, mucus plug (e.g., asthma, ABPA) |
| Infection | TB (most common in India), severe/recurrent pneumonia, pertussis, measles |
| Cystic fibrosis | CFTR mutation -> thick mucus -> chronic Pseudomonas infection |
| Foreign body (chronic) | Aspirated foreign body in children |
| Kartagener/ciliary dyskinesia | Primary ciliary dyskinesia -> impaired mucociliary clearance |
| ABPA | Allergic bronchopulmonary aspergillosis |
The obstruction-infection cycle (pathogenesis):
Airway obstruction or impaired clearance -> secretion retention -> bacterial colonisation and infection -> wall inflammation and destruction -> permanent dilatation -> further impairment of clearance -> more infection -> progressive expansion.
This vicious cycle is the unifying mechanism regardless of the initial insult. Breaking the cycle (airway clearance, antibiotics, surgery) is the therapeutic principle.
Bronchiectasis -- Morphology and Complications
Bronchiectasis: Morphology and Complications
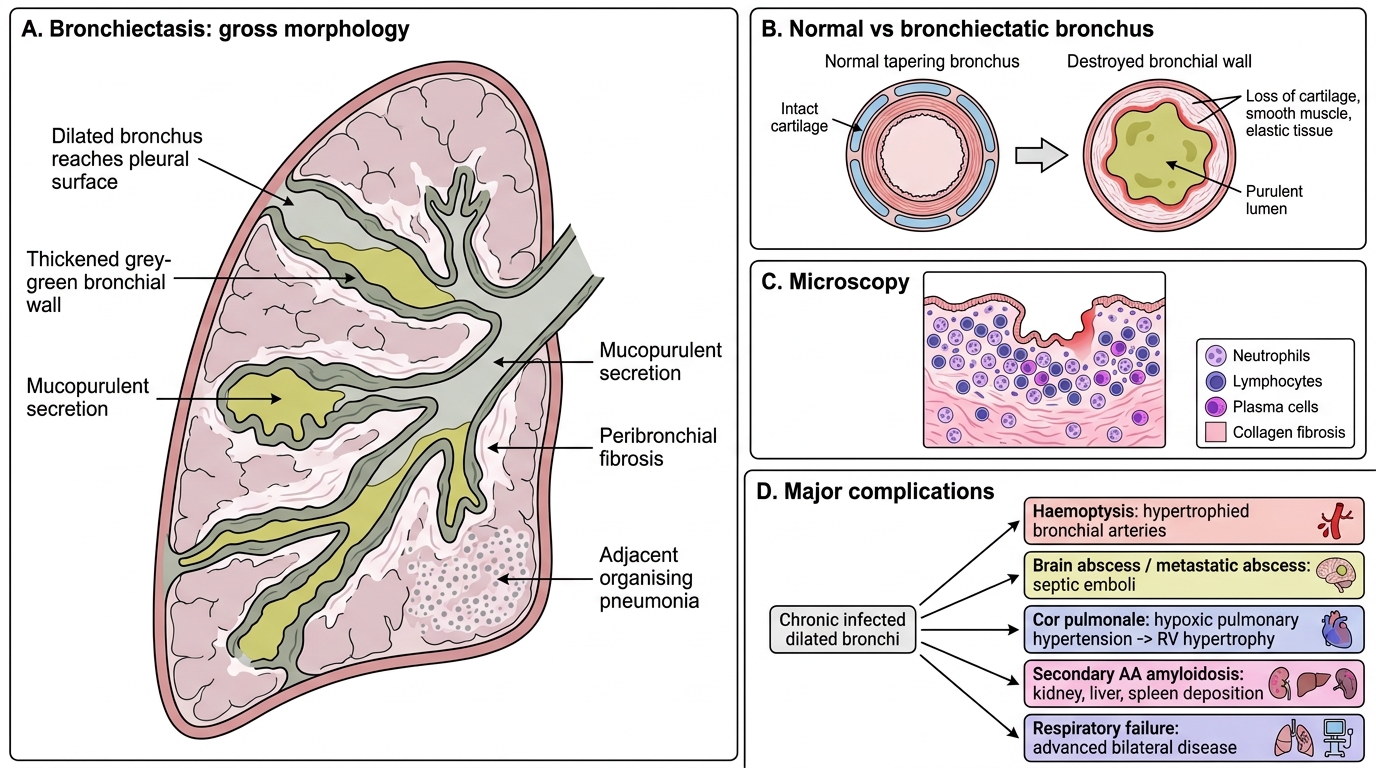
Macroscopy:
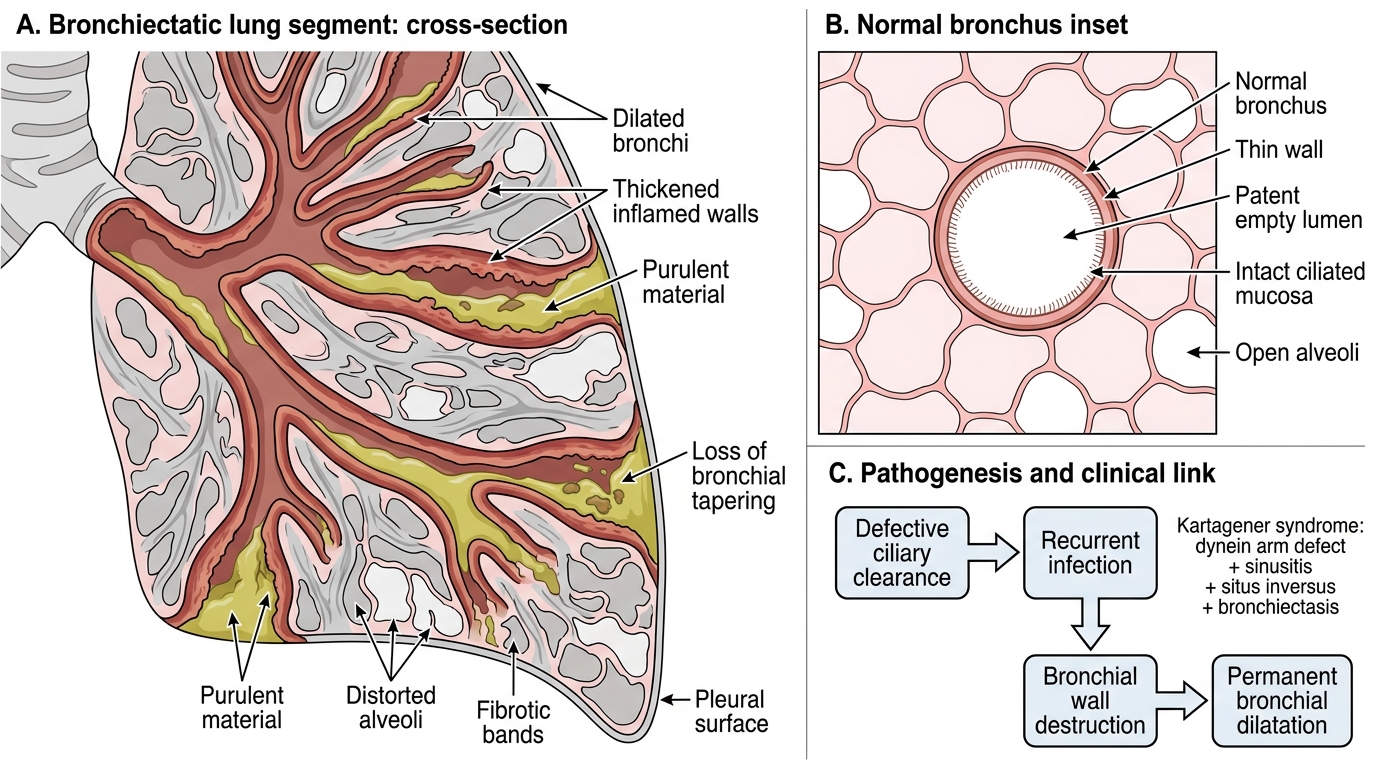
- Dilated bronchi extending to the pleural surface (normal bronchi taper and don't reach the pleura -- diagnostic clue on imaging).
- Bronchi filled with mucopurulent or frankly purulent secretions.
- Walls thickened, grey or greenish.
- Lower lobes most commonly affected (gravity-dependent drainage failure); also right middle lobe, lingula.
Microscopy:
- Destruction of bronchial wall -- loss of cartilage, smooth muscle, elastic tissue.
- Dense chronic inflammatory infiltrate (neutrophils, lymphocytes, plasma cells).
- Ulceration and fibrous replacement of bronchial wall.
- Adjacent lung: fibrosis, organising pneumonia.
Complications:
- Haemoptysis -- due to hypertrophied bronchial arteries; can be massive and life-threatening.
- Brain abscess / metastatic abscess -- septic emboli from infected bronchi.
- Cor pulmonale -- hypoxic pulmonary hypertension -> right ventricular hypertrophy and failure.
- Secondary amyloidosis (AA) -- from chronic suppurative infection -> serum amyloid A deposition in kidney, liver, spleen.
- Respiratory failure -- in advanced bilateral disease.
Bronchiectasis: Dilated Bronchi with Fibrosis
SELF-CHECK
A 35-year-old man with recurrent sinusitis and infertility is found to have bilateral lower-lobe bronchiectasis. CT of the chest shows situs inversus. Which underlying defect is responsible?
A. CFTR gene mutation
B. alpha-1-Antitrypsin deficiency
C. Dynein arm defect (primary ciliary dyskinesia)
D. IgA deficiency
Reveal Answer
Answer: C. Dynein arm defect (primary ciliary dyskinesia)
The triad of bronchiectasis + sinusitis + situs inversus is Kartagener syndrome -- a subset of primary ciliary dyskinesia caused by defective dynein arms of cilia. Immotile cilia fail to clear secretions, causing recurrent sinopulmonary infections; defective nodal cilia cause situs inversus. CFTR mutation (cystic fibrosis) causes bronchiectasis but not situs inversus. IgA deficiency causes recurrent infections but not situs inversus.
COPD Complications and Evaluation
COPD Complications and Evaluation
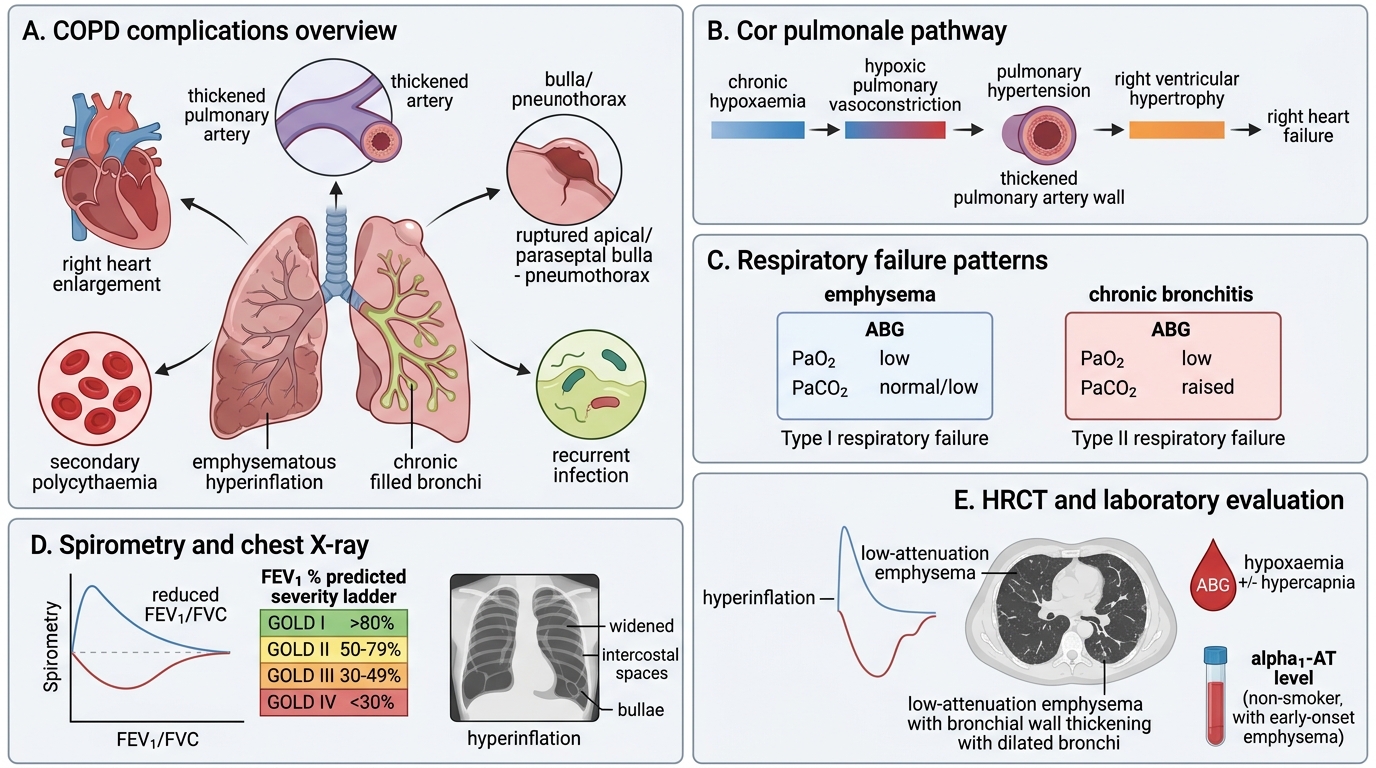
Complications of COPD (emphysema + chronic bronchitis):
- Cor pulmonale -- Hypoxia -> hypoxic pulmonary vasoconstriction -> pulmonary hypertension -> right ventricular hypertrophy -> right heart failure. More severe in chronic bronchitis (hypoxaemia more pronounced).
- Respiratory failure -- Type I (low PaO2, normal/low PaCO2) in emphysema; Type II (low PaO2 + raised PaCO2) in chronic bronchitis.
- Spontaneous pneumothorax -- Rupture of paraseptal bullae; classically in young, thin men or as a complication of emphysema.
- Secondary polycythaemia -- Chronic hypoxaemia -> increased erythropoietin -> raised haematocrit (compensatory, but increases viscosity).
- Recurrent respiratory infections -- Mucus retention (chronic bronchitis) impairs clearance.
Evaluation:
- Spirometry: FEV1/FVC <0.70 confirms obstruction; FEV1 % predicted grades severity (GOLD stages I-IV: >80%, 50-79%, 30-49%, <30%).
- Chest X-ray: Hyperinflation (>6 anterior ribs), flattened diaphragm, widened intercostal spaces, bullae in emphysema; peribronchial markings increased in chronic bronchitis.
- HRCT: Low-attenuation areas in emphysema; bronchial wall thickening, dilated bronchi in bronchiectasis.
- ABG: Hypoxaemia +/- hypercapnia.
- alpha1-AT level: In non-smokers with early-onset emphysema.
SELF-CHECK
Post-mortem examination of a 65-year-old with known COPD shows marked right ventricular hypertrophy and dilation. Pulmonary artery walls are thickened. Which mechanism best explains this finding?
A. Systemic hypertension transmitted retrogradely
B. Left ventricular failure leading to pulmonary venous congestion
C. Hypoxic pulmonary vasoconstriction causing pulmonary hypertension
D. Pulmonary thromboembolism from deep vein thrombosis
Reveal Answer
Answer: C. Hypoxic pulmonary vasoconstriction causing pulmonary hypertension
Cor pulmonale -- right ventricular hypertrophy from pulmonary causes -- in COPD results from chronic hypoxia. Hypoxia triggers vasoconstriction of pulmonary arterioles (the Euler-Liljestrand reflex), raising pulmonary vascular resistance. Sustained vasoconstriction leads to medial hypertrophy of pulmonary arteries and pulmonary hypertension, which the right ventricle must pump against. Systemic hypertension affects the left ventricle; left ventricular failure causes left-sided congestion, not right ventricular hypertrophy in isolation.
CLINICAL PEARL
Remember the spirometry rule for long-answer questions: COPD severity is graded by post-bronchodilator FEV1 (GOLD stages), not FEV1/FVC ratio alone. The ratio just confirms obstruction; the FEV1 % predicted tells you severity. In asthma, obstruction is reversible -- FEV1/FVC improves by >=12% and >=200 mL after bronchodilator. This reversibility distinguishes asthma from fixed obstruction in COPD in clinical examination stations.