Page 13 of 32
PA25.5 | Occupational & Interstitial Lung Disease — SDL Guide
Learning Objectives
- Define restrictive lung disease and distinguish its spirometric pattern from obstructive disease
- Define pneumoconiosis and explain how particle size, dose, solubility, and host factors determine lung injury
- Describe the pathogenesis, morphology, and complications of coal worker's pneumoconiosis, silicosis, and asbestosis
- Recognise the special risks of silicosis (TB susceptibility, eggshell calcification) and asbestosis (mesothelioma, bronchogenic carcinoma)
- Outline the key features of hypersensitivity pneumonitis, idiopathic pulmonary fibrosis, and sarcoidosis as additional causes of ILD
- List the major complications shared by all progressive pneumoconioses
INSTRUCTIONS
Occupational and interstitial lung diseases are a group of conditions where the lung parenchyma is progressively replaced by fibrosis. In India, mining, stone-cutting, and construction expose millions of workers to fibrogenic dusts every year. Understanding how inhaled particles trigger macrophage activation and irreversible fibrosis underpins both clinical recognition and preventive medicine — core skills for the PA25.5 competency and for your future practice.
References
- Robbins & Cotran Pathologic Basis of Disease, 10th ed., Ch 15 (textbook)
- Harsh Mohan Textbook of Pathology, 8th ed., Ch 16 (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old slate quarry worker from Rajasthan presents with progressive breathlessness and bilateral upper-lobe opacities. His sputum is positive for AFB. Chest X-ray shows calcified hilar lymph nodes with an 'eggshell' pattern. What single occupational exposure connects the fibrosis, the calcification pattern, AND the TB reactivation — and why does silica make the lung so vulnerable to mycobacteria? This module unravels the pathology of dusts, fibres, and antigens that turn the lung's own defence system into a fibrogenic engine.
WHY THIS MATTERS
India ranks among the world's highest-burden countries for silicosis and asbestos-related disease. Sandstone quarrying in Rajasthan, slate mining in Uttarakhand, and ship-breaking in Alang (Gujarat) expose hundreds of thousands to fibrogenic dusts. PA25.5 is tested in university practicals (gross specimen and slide identification) and in clinical postings where you will be asked to take occupational histories. Mesothelioma, although rare, is a direct consequence of asbestos exposure — a fact that connects this SDL to the RS tumours module.
RECALL
Before proceeding, quickly recall:
• What is FEV1/FVC ratio? In which direction does it change in obstructive vs restrictive disease?
• What cell type patrols the alveolar surface and engulfs inhaled particles?
• What is the difference between a granuloma and simple fibrosis at the histological level?
• Name two cytokines that activate fibroblasts.
If any of these feel uncertain, spend two minutes reviewing your Year-1 Physiology notes on spirometry and your Histology notes on macrophage function before continuing.
Restrictive Lung Disease — Pattern and Principle
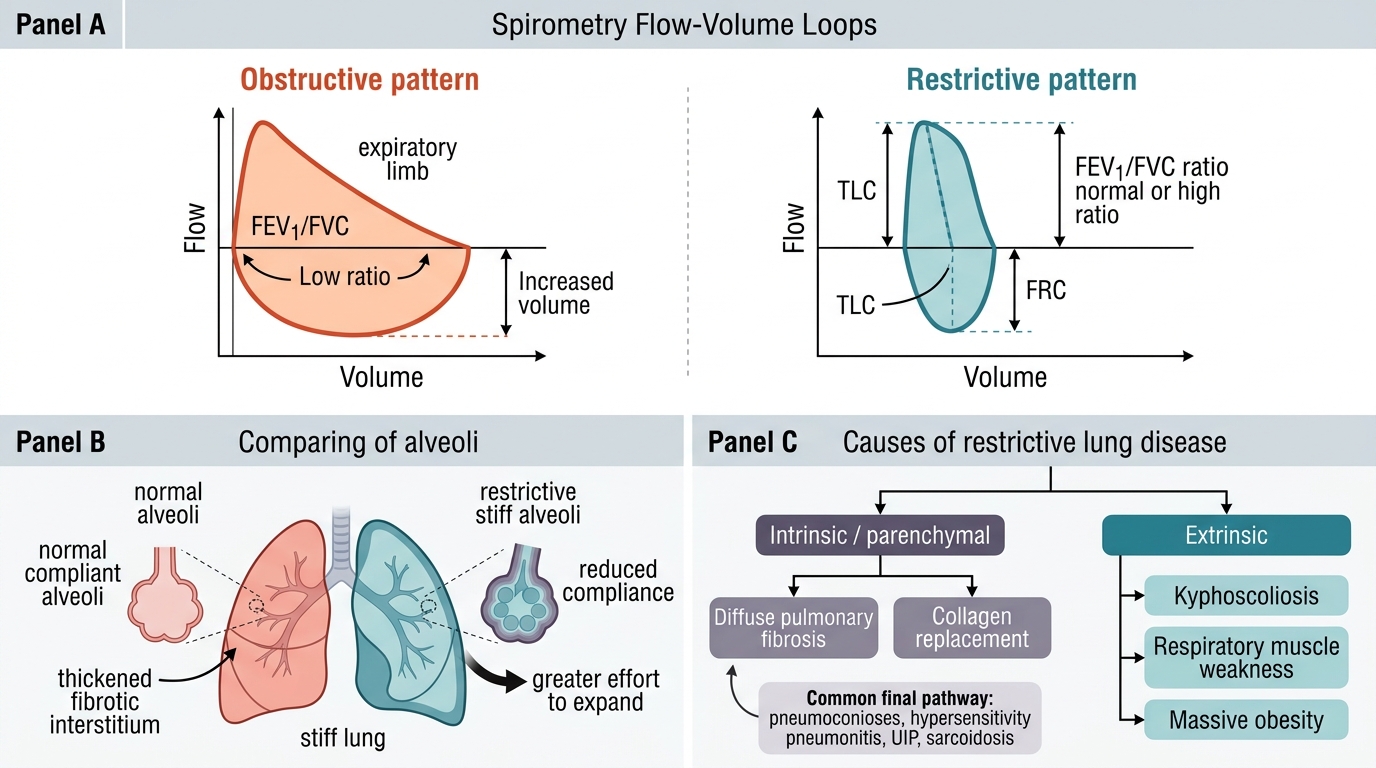
Restrictive Lung Disease: Pattern and Principle
Restrictive lung disease (RLD) is a functional category defined by reduced lung compliance — the lungs are stiffer than normal, so expanding them requires greater effort.
Key spirometric features:
• ↓ Total Lung Capacity (TLC)
• ↓ Functional Residual Capacity (FRC)
• ↓ Forced Vital Capacity (FVC)
• FEV1/FVC ratio — normal or elevated (both FEV1 and FVC fall proportionally, or FVC falls more)
This contrasts with obstructive disease (asthma, COPD, emphysema) where FEV1/FVC is reduced because airflow is the problem, not volume.
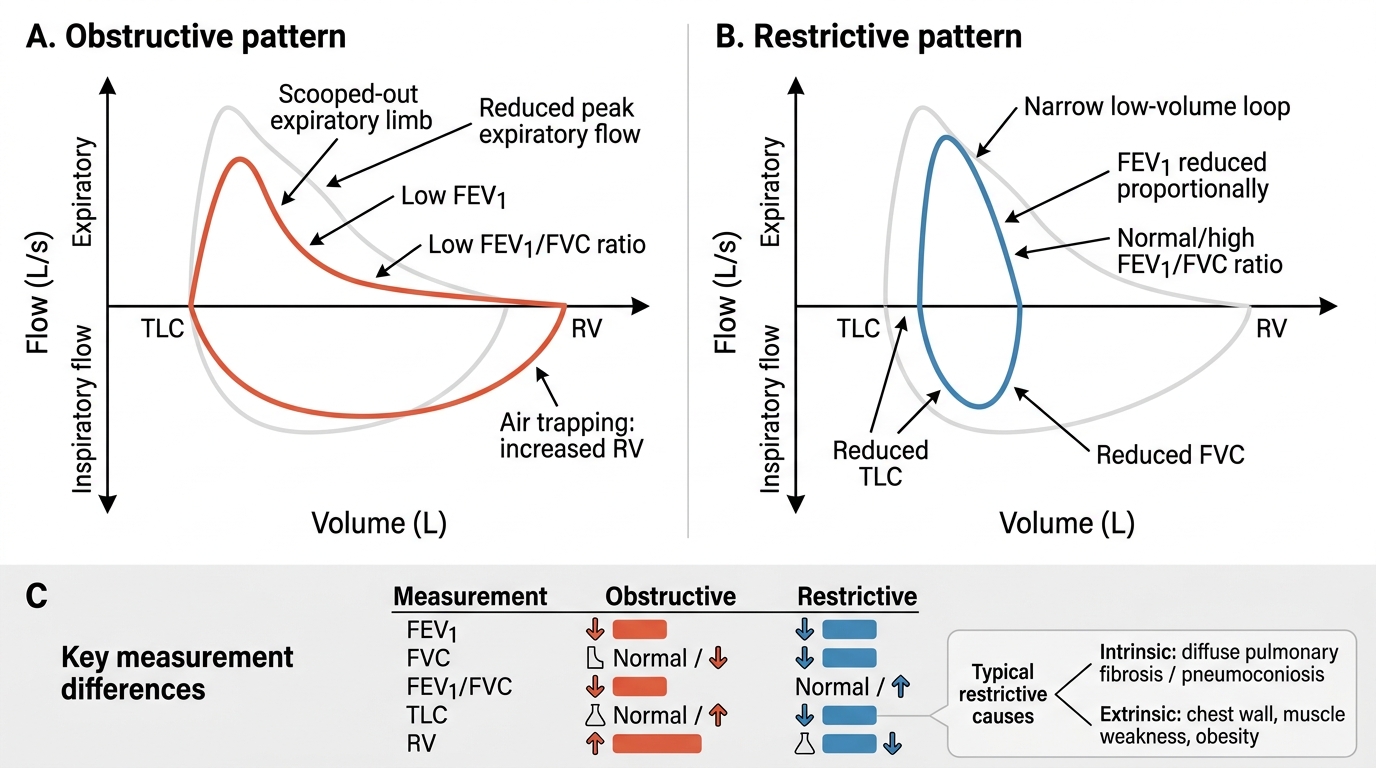
Obstructive vs Restrictive Flow-Volume Loops
Causes of RLD span two broad groups:
1. Intrinsic (parenchymal): diffuse lung fibrosis replaces elastic alveolar tissue with stiff collagen — the end-point of almost all interstitial lung diseases.
2. Extrinsic: chest wall deformities (kyphoscoliosis), respiratory muscle weakness, massive obesity — not covered here.
Diffuse pulmonary fibrosis is the common final pathway for pneumoconioses, hypersensitivity pneumonitis, UIP, and sarcoidosis.
Pneumoconiosis — Definition and Determinants
Pneumoconiosis: Definition and Determinants of Injury
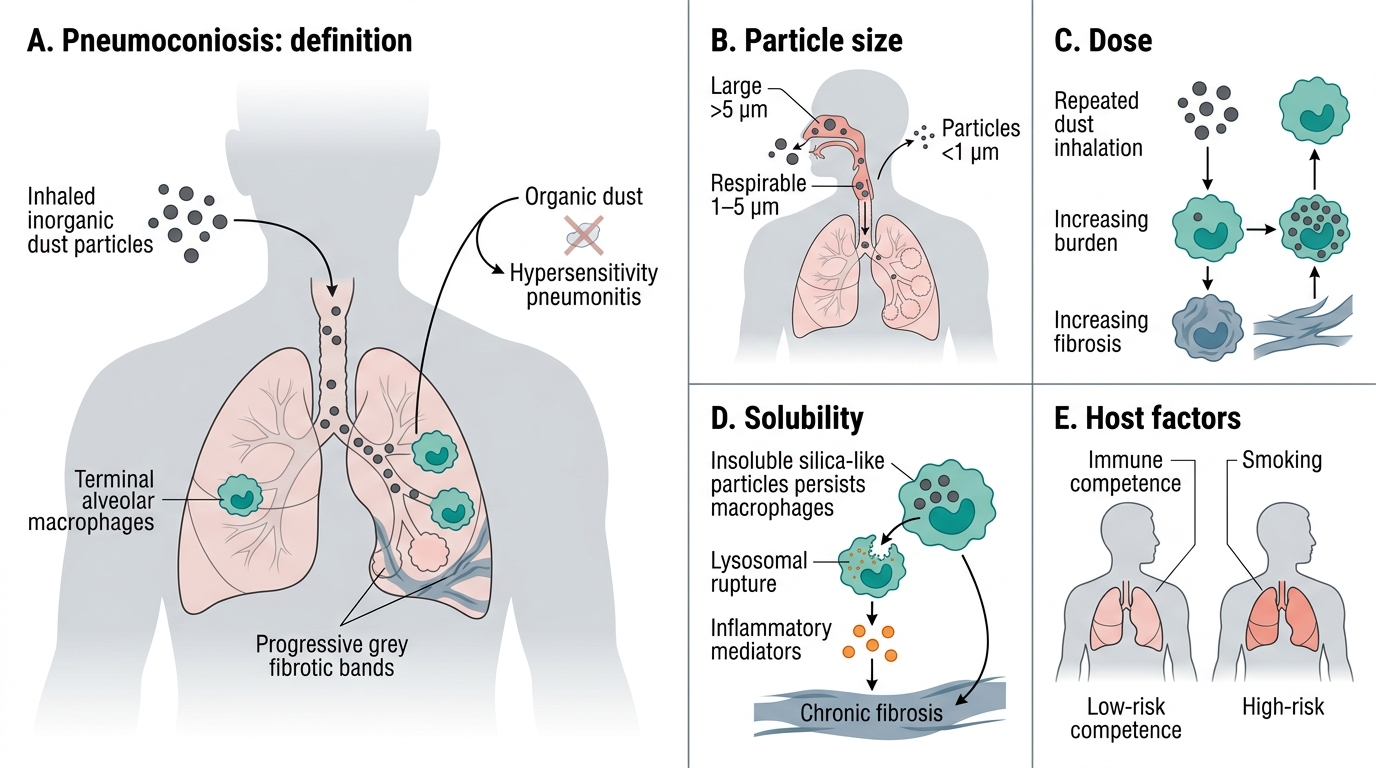
Pneumoconiosis is defined as the non-neoplastic reaction of the lung to inhaled mineral or inorganic dust, leading to pulmonary fibrosis.
The term is from Greek: pneumon (lung) + konis (dust). It excludes organic-dust diseases (those cause hypersensitivity pneumonitis).
Four determinants of injury severity:
| Determinant | High-risk extreme | Explanation |
|---|---|---|
| Particle size | 1–5 µm | Large particles (>5 µm) trapped in upper airways; tiny particles (<1 µm) exhaled. The 1–5 µm 'respirable fraction' reaches alveoli. |
| Dose | Cumulative lifetime exposure | Higher cumulative dose → more macrophage activation → more fibrosis |
| Solubility | Low solubility (e.g., silica) | Insoluble particles persist in macrophages; repeated lysosomal rupture drives chronic inflammation |
| Host factors | Immune competence, smoking | Smokers have impaired mucociliary clearance; immunosuppression ↑ TB risk in silicosis |
General pathogenesis (shared mechanism):
1. Respirable particles reach alveoli and are engulfed by alveolar macrophages.
2. Particles that are cytotoxic (especially silica) rupture the phagolysosome, killing the macrophage and releasing the particle — which is then re-ingested by a fresh macrophage (perpetual cycle).
3. Activated macrophages release fibrogenic cytokines: IL-1, TNF-α, TGF-β, PDGF.
4. Fibroblasts proliferate → collagen deposition → progressive fibrosis.
5. Ongoing inflammation may recruit lymphocytes and form granulomas (silicosis, sarcoidosis).
SELF-CHECK
Which particle size range is most dangerous in pneumoconiosis because it reaches the alveoli?
A. < 0.5 µm (ultrafine)
B. 1–5 µm (respirable fraction)
C. 5–10 µm (large respirable)
D. > 10 µm (upper airway trapped)
Reveal Answer
Answer: B. 1–5 µm (respirable fraction)
Particles > 5 µm are trapped in the nose, pharynx, and upper airways by turbulent flow and mucociliary clearance. Particles < 1 µm behave like gases and are largely exhaled. The 1–5 µm 'respirable fraction' follows laminar flow into respiratory bronchioles and alveoli where macrophages engulf them — this is where the fibrogenic reaction begins.
Coal Worker's Pneumoconiosis
Coal dust = predominantly carbon (anthracite/bituminous) with variable silica content. Carbon is relatively inert; the silica fraction drives more fibrosis.
Three morphological stages:
- Anthracosis — Inert carbon pigment deposition in macrophages and lymph nodes. Seen in all urban dwellers and smokers; causes NO functional impairment. Carbon pigment appears as black granules in macrophages around bronchioles and lymphatics.
- Coal macules and nodules — Aggregates of dust-laden macrophages (1–2 mm, black) around respiratory bronchioles → focal emphysema from bronchiolar dilation. Coal nodules are larger (>5 mm) with central collagen. Mild restrictive defect possible.
- Progressive Massive Fibrosis (PMF) — Large (>2 cm, up to 10 cm) black fibrotic masses, typically upper lobes. Central necrosis (ischaemia) may create cavities (not caseation). Severe restrictive disease + cor pulmonale.
Caplan syndrome: In coal workers (and other pneumoconioses) with co-existing rheumatoid arthritis, immune-mediated large necrobiotic nodules (0.5–5 cm) develop rapidly in the periphery of the lung. Caplan nodules represent the intersection of occupational exposure and autoimmune inflammation.
Key points:
• No proven ↑ risk of lung cancer from coal dust alone (unlike silica/asbestos)
• PMF can progress even after exposure ceases
• Cor pulmonale is the terminal event in severe disease